Crusty and Scaly Dermatoses
Crusts and scales are frequently associated with trauma, either caused by fights or self-inflicted, as in pruritic dermatoses. Most dermatoses of the ear margin are also associated with crusting.
Scales are a common feature of dermatophytosis. In some dermatoses that usually involve the whole pinna, including dermatophytosis, pemphigus, and zinc-responsive dermatitis, these symptoms can be a main feature (Figure 12-11).Dermatophytosis
Dermatophytes live on keratin, and the most common dermatophyte found in dogs and cats, Microsporum canis, invades mainly the hair; the primary lesions of dermatophytosis are follicular casts and scales. Infected hairs are abnormal and fragile; they break easily, and alopecia quickly results. The classical presentation of dermatophytosis in dogs and cats is annular alopecia associated with fine silvery scales, central healing, and peripheral follicular papules and crust. This lesion is commonly observed on the pinnae.4 In cats, pinnal lesions caused by dermatophytes are more common than they are in dogs. In both species, lesions usually are not symmetrical, as opposed to other causes of pinnal alopecia.
Dermatophytosis is a complex disease and its clinical manifestations are variable. They include seborrhea, localized folliculitis or furunculosis (especially on the face),

Figure 12-11
Generalized and severe scaling in a 5-year-old German Shepherd dog with advanced leishmaniasis. The pinnae are also involved. The dog goes to Portugal each summer.
kerion or other granulomatous reactions, papular dermatitis, erythematous dermatitis, pruritus, and even subcutaneous nodules (termed dermatophytic pseudomycetoma). Lesions with both macroscopic and dermatopathologic features of pemphigus foliaceous or pemphigus erythematosus have been reported that are caused by a dermatophyte (usually T mentagrophytes or M.
persicolor).The clinician should consider dermatophytosis as a possible differential diagnosis if the clinical features and the history are compatible:
• Age: Dermatophytosis is most commonly seen in young animals. Adults (more commonly cats) can be asymptomatic carriers, especially Persian cats. Sylvatic dermatophytosis (i.e., acquired from wild mammals) is usually seen in older animals. In these cases the causative dermatophyte is not M. canis, and the clinical signs can vary greatly.
• Breed: Persian cats in particular but also exotic short-haired cats, Yorkshire Terriers, and Pekingese are predisposed to M. canis infection. Yorkshire Terriers may be susceptible to develop severe forms. Dogs and breeds used for hunting or with hunting habits are predisposed to sylvatic dermatophytosis because of their more frequent contact with wild mammals.
• Contagion: Dermatophytes are transmitted by contact with fungal elements (infected hair or scales, soil); they also may be present on infected animals, in the environment, or on fomites. Contact with infected animals is the most common source for the most prevalent dermatophytes. Exact identification usually allows identification of the source of infection.
Experimental diagnosis is mainly based on positive fungal culture. A recent study has confirmed the importance of daily observation if dermatophyte test medium (DTM) is used because contaminants can also cause the color to change from yellow to red. Most dermatophytes do not develop fully on this medium, and they can be difficult to identify precisely unless cultured again on Sabouraud’s medium.
Microscopic observation of infected hair or scales in skin scrapings can be sufficient if the clinician is experienced. Because infected hairs are fragile and break easily and dermatophytes can infect the stratum corneum, skin scraping is probably more favorable than trichography for sample collection (both microscopic examination and fungal culture). Trichography can be performed under the Wood’s lamp to collect fluorescent hair (Figure 12-12).
M. canis is the only commonly encountered dermatophyte that fluoresces. In order to reduce false positives, the clinician should make sure that the fluorescence involves the hair shaft and/or the follicular ostia. A diffuse positive reaction over the skin is probably caused by topical drug application. False negatives are also encountered. Some cases of dermatophytosis, especially atypical clinical presentations, can be detected on dermatopathologic examination.Treatment of dermatophytosis should always involve the whole body surface even if the pinna is the only site with macroscopic lesions. Systemic and/or topical treatments
Figure 12-12
Positive Wood's lamp examination of a cat with dermatophytosis caused by Microsporum canis.
are widely available (griseofulvin, ketoconazole, itraconazole, econazole, Ierbinafme). Dermatophytosis is zoonotic, and the practitioner has the responsibility to inform owners to seek medical attention if they develop lesions.
Pemphigus Complex
The classification of the pemphigus group of diseases is still controversial. They are the most frequent autoimmune skin diseases in dogs and cats, the most common being pemphigus foliaceus (PF) and then pemphigus erythematosus (PE). In the pemphigus group, these two diseases have a characteristic facial and aural involvement.
Pemphigus complex diseases are primarily pustular in dogs and cats. Most pustular dermatoses involve the hair follicle. PF and PE are almost the only diseases to cause numerous pustules and crusts in the concave surface of the pinna (Figure 12-13). They can be restricted to the inner pinna but commonly also affect the dorsal pinna.
In PF, lesions usually also affect other areas of the skin: face (periocular area, nasal planum), feet, clawbed, footpads, and inguinal area. General involvement is not uncommon. In PE, lesions are almost always restricted to the face and ears.
Because pustules are transient in dogs and cats, observed lesions in PF and PE are usually secondary and include thick crusts, scales, and alopecia overlying oozing and erosive skin bordered by epidermal collarettes. Pain and/or pruritus can be present but are not primary features. Depigmentation is common in PE but occurs rarely or late in the course of the disease in PF (Figure 12-14).Differential diagnosis should include contact dermatitis, cutaneous adverse drug reaction, dermatophytosis, demodicosis, bacterial folliculitis, discoid and systemic lupus erythematosus, leishmaniasis, and zinc-responsive dermatitis. Both dermatophytosis and drug reactions can cause pustular acantholytic dermatoses.
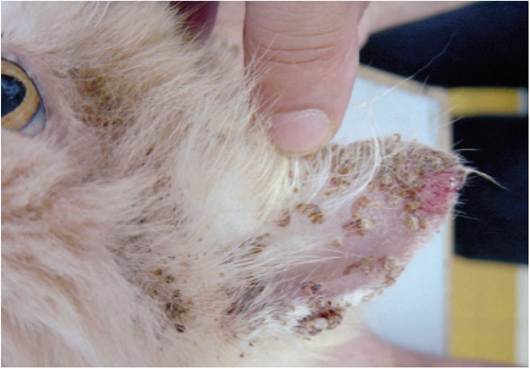
Figure 12-13
Erosive and crusted lesions on the concave surface on the pinna of a cat with PF.

Figure 12-14
Erythema and large, fluctuant, fragile pustules on the inner pinna of an 8-month-old Golden Retriever with PF. These lesions are seldom seen.
Diagnosis is based on the elimination of other differential diagnoses, compatible histologic examination of biopsy samples, and positive immunofluorescence and/or immunochemistry results. Most pemphigus cases are considered spontaneous, but some anecdotally reported cases have been identified or suspected to be paraneoplastic or food related.16
Treatment includes mainly immunosuppressive drugs such as prednisolone, azathioprin (dogs), or chlorambucil.
Zinc-Responsive Dermatosis
Zinc-responsive dermatosis causes hyperkeratotic or crusty skin lesions on the pinna. Other parts of the body are also usually involved, especially the face.
Two syndromes are recognized. A strong breed predisposition is observed in syndrome I for Siberian Huskies and Alaskan Malamutes. Other breeds such as the Bull Terrier have been mentioned.
The early lesions occur at 1 to 3 years of age. Erythema affects the ears, mouth, chin, eyes, and pressure points (elbows, hocks). Alopecia, crusting, and scaling (with or without underlying suppuration) quickly occur, often associated with secondary pruritic bacterial and/or Malassezia infection. Otherwise, pruritus is variable. The hair coat is usually dull with a generalized seborrhea. Other signs are less common (onychomalacia, modifications in the sense of taste or smell). Stress of any kind could be a precipitating factor. The pathogenesis of this syndrome is controversial, considering that in these dogs the zinc intake is usually normal, but the condition responds to zinc supplementation.Syndrome II is seen in rapidly growing dogs (mainly of large or giant breeds) with insufficient zinc intake resulting from inappropriate food formulation or the presence of elements in the diet that interfere with zinc such as phytates (zinc chelation)

Figure 12-15
Areas of alopecia, hyperkeratosis, and hyperpigmentation of both pinnae and the face of a dog with generic food dermatosis.
and calcium (modification of zinc absorption). Oversupplementation with minerals and vitamins can be sufficient to cause zinc-responsive dermatosis. Hyperkeratotic plaques are seen on areas of repeated trauma on pressure points, including the pinna, footpads, and nasal planum. Treatment should be aimed at correction of the diet.
Generic Food Dermatitis
Generic food dermatosis is often difficult to differentiate from zinc-responsive dermatosis syndrome II because the causes, predisposed animals, clinical signs, and treatment are similar (Figure 12-15).