Dermatoses of the Ear Margin
Vasculitis
Extremities (pinna, digits, tail) have a vasculature that lacks anastomosis and is particularly susceptible to environmental injuries (trauma, temperature). Clinical manifestations of diseases causing vascular lesions such as inflammation (vasculitis) and thrombosis often involve the extremities, particularly the pinna borders (Figure 12-7).
Nevertheless, some specific types of vasculitis induce local lesions such as rabies vaccine-related vasculitis (lesions at the injection site) or lesions resulting from perivenous injection of irritant substances.Clinical manifestations of pinna vasculitis are quite stereotypic, regardless of the cause of the vasculitis. The pinna borders are preferential sites, especially the apex and its concave surface. Primary lesions include purpura, plaques, papules, pustules, and in severe cases, hemorrhagic bullae. Purpura can be distinguished from erythema because it does not blanch on diascopy (looking through a glass slide firmly applied on the lesion). Punched-out ulcers and necrosis quickly result from
160" class="lazyload" data-src="/files/uch_group75/uch_pgroup311/uch_uch7298/image/image160.jpg">
Figure 12-7
Crusts and scales on the apex of a female Malinois Shepherd dog. The cause of the vasculitis was not identified.
the lack of perfusion. The shape and disposition of the lesions clearly correlate with the vascular pathways. As the disease evolves, the whole pinna border can become involved. Differential diagnosis includes arthropod bite, fight wounds, cold agglutinin diseases, frostbite, and coagulopathies.
Because necrosis occurs within hours of the infarct, biopsy should be taken preferably on the most recent lesions. The biopsy should involve both diseased tissue and the border of the lesions because the vascular event is situated there. The owner should be aware that biopsy of the pinna can cause lifelong and visible deformation and tissue defects.
If the submitted sample includes the area where vascular injury occurred, dermatopathology allows the diagnosis of vasculitis, but it usually does not permit precise identification of the cause. This part of the diagnosis is mandatory if an appropriate treatment regimen is to be chosen and relapse is to be prevented.Underlying causes of vasculitis are divided into the following:
• Precipitating factors: Infection, drugs, low temperatures. Vaccines are reported to cause injection site vasculitis as well as lesions on the apex of the pinna and often on the concave surface. Other extremities, the face (periocular area), and bony prominences can also be affected.
• Concurrent diseases: Infection, insect bite, neoplasia, food-related causes, connective tissue disorders (e.g., lupus erythematosus), cold agglutinin diseases.
In one study, no underlying cause for vasculitis could be found in about 50% of cases.14 Two idiopathic conditions have been described that can affect the pinna: familial cutaneous vasculopathy of German Shepherd dogs and proliferative thrombovascular necrosis of the pinna. They are described in the following sections. Cold agglutinin diseases are described under Frostbite.
The outcome and treatment depend on the suspected or diagnosed underlying cause(s). Because vasculitis is a severe complication, it should be treated while the underlying cause is being explored or at the beginning of its correction. Pentoxyfylline has many effects, including increased red blood cell pliability and immunomodulation. It is considered the first-line treatment in vasculitis and other ischemic diseases. Propentoxyfylline is licensed in many countries for geriatric dogs with behavioral problems related to microvascularization disorders in the brain. Pentoxyfylline itself remains in the peripheral circulation. This latter drug has not been thoroughly evaluated in dogs, but the proposed dosage is 10 mg/kg q8h to q24h. Side effects appear to be minimal and are considered to regress after treatment cessation.
They include vomiting and diarrhea; the author has also observed a few cases of rectal bleeding. An anecdotal report of thrombocytopenia indicates that care should be taken when prescribing pentoxyfylline in affected dogs.Steroids can be added to pentoxifylline. Topical treatment is usually suficient. Systemic prednisolone (2 to 4 mg/kg, q24h, by mouth) can be necessary in the most severe cases (especially in cases of neutrophilic vasculitis), if no underlying infectious process has been identified. Other possible treatments that have been proposed include large doses of vitamin E (adjunct therapy), dapsone (to be used with caution in cats), cyclophosphamide, azathioprine, and the association tetracycline/niacinamide.
Familial Cutaneous Vasculopathy of German Shepherd Dogs
In German Shepherd puppies, a familial cutaneous vasculopathy has been recognized with an autosomal, recessive mode of inheritance.17 Initial lesions include depigmented and swollen footpads. The pinnae, tail, and nasal planum are usually also affected, displaying alopecia, crusts, and ulceration. Dermatopathology demonstrates vascular degeneration and vasculitis, as well as other dermal changes: nodular dermatitis, collagenolysis, and cell-poor interface dermatitis with basal cell apoptosis.
Proliferative Thrombovascular Necrosis of the Pinna
This condition is recognized in the dog and differs from other types of vasculitis affecting the ear by its histopathologic features—arterioles initially develop into folds in the lumen. Sclerosis and hyaline degeneration are also observed, and eventually thrombosis. Clinical features are similar to those of other types of vasculitis affecting the pinna border. Pentoxyfylline is usually partially to 100% effective.14,18 Topical steroids are an option. Because this condition is restricted to the pinna, more potent immunosuppressive treatments with potential systemic side effects should be avoided. If medical treatment is unrewarding, surgical removal of diseased tissue is effective.
Relapses are reported following excisions with a narrow margin.3Solar Dermatitis and Actinic Keratosis of the Ear
Repeated exposure to direct or reflected sunlight (especially ultraviolet B [UVB] and ultraviolet C [UVC]) on white skin causes actinic reactions (from the Greek actin, ray) that can vary from the so-called sunburn (solar dermatitis) to actinic keratosis and eventually squamous cell carcinoma. Animals with white ears or white spots that include the pinna are at risk if they live in a sunny region; these include white cats, Dalmatians, American Staffordshire Terriers, Bull Terriers, and white Bulldogs.
In animals with erect ears, especially cats, the pinna borders are seldom protected from sunlight by the fine pinnal hair coat. In white animals, erythema and fine scaling (solar dermatitis) can appear as early as 3 months of age. As the lesions aggravate, the erythema is more pronounced and associated with crust formation. The lesions bother the animal and are usually painful; self-trauma aggravates the condition. Careful observation shows that the border of the pinna is finely curled. The nasal planum is usually also affected, especially in dogs, where it can be the only involved area. The lower eyelids and the lips may also be involved. Differential diagnosis includes insect bites, fight wounds, vasculitis, and early sarcoptic or notoedric mange. At this stage, keeping the animal indoors (including the prevention of lying in the sunlight) from 10 AM to 4 PM should be sufficient.
In the summer, lesions recur and worsen (Figure 12-8). The ear margins become thickened, indurated, and hyperkeratotic. Atypia and dysplasia of the epidermis, as well as follicular keratinocytes and solar elastosis, are observed on dermatopatho- logic examination. Sun avoidance is sufficient only in early cases. Systemic retinoids

Figure 12-8
Squamous cell carcinoma on the right ear of a white domestic short-hair cat.
The right ear apex is finely curled, an almost pathognomonic early symptom of sun-related injury.or surgical excision of damaged tissue is usually necessary. If the lesions are pruritic and/or painful, topical or systemic glucocorticoids are indicated.
Squamous cell carcinoma can result, especially if the disease is neglected or the animal cannot be kept inside. The neoplasm can be proliferative or ulcerative, but usually bleeds easily. Squamous cell carcinoma is considered to be mainly locally invasive and slow to metastasize, so amputation of the pinna is effective in many cases.
Frostbite
Frostbite is caused by prolonged exposure to temperatures below freezing (cold climate, contact with cold objects). All extremities are predisposed to frostbite, but especially the pinnae, which are very thin but have a large surface area (Figure 12-9). Other predisposing factors include previous frostbite, vasculopathy, internal illness, insufficient acclimatization to cold weather, lack of shelter, freezing wind, and wetting. All these factors decrease the time needed for lesions to appear. Frozen skin is pale and cold, with reduced sensitivity. The skin should be thawed as soon as possible to prevent necrosis. Warm water is gently applied on affected areas. Thawing of the skin may be painful. In areas that are not necrotic, erythema and edema are usually present.
In mild cases, frostbite may induce no lesions besides mild ear-border curling, whitening of the hair, alopecia, and in more severe cases, necrosis. It may take some time for the skin to reveal the total extent of the damage, so the affected tissue can take some weeks to heal. Pentoxyfylline associated with aspirin has been shown to improve tissue viability in rats.14
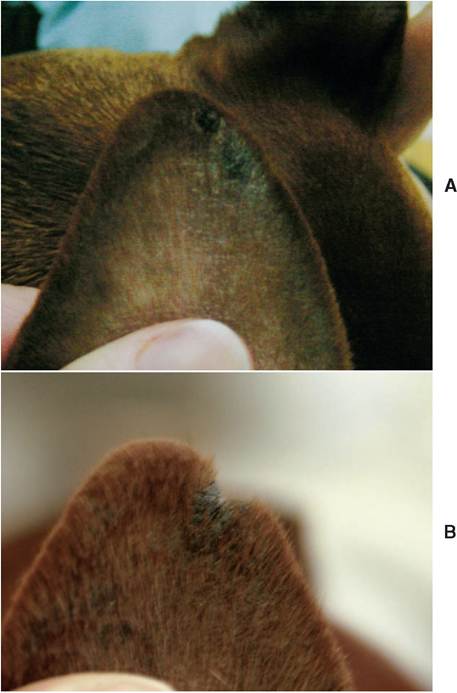
Figure 12-9
A, Early lesions of cold agglutinin-related pinnal vasculitis (December) in a 1-year-old male Pinscher cross: crusts and hyperpigmentation are present on the concave surface of the apex of the auricle.
B, In February, crusted, punched-out lesions are present on the same dog. Two episodes of bleeding were associated with temperatures below 0°C.Cryoglobulinemia and Cryofibrinogenemia
Different components of the serum (cryoglobulins) or the plasma (cryofibrinogens) may precipitate under cold temperature. The process is usually reversed when the temperature rises again. These diseases were formerly termed cold agglutinin diseases. At least three types of cryoglobulinemia have been identified. Symptoms result from the anemia and/or hemagglutination associated with the process. Because of the lack of anastomoses on their margins, the ear pinnae are more commonly affected.
Ear-Margin Seborrhea
Ear-margin seborrhea or dermatosis is most commonly observed in pendulous-eared breeds such as the Dachshund, Springer and Cocker Spaniels, Beagles, Basset Hounds, and Dobermans with uncropped ears.3 The pathogenesis of this condition is not established, even though predisposing factors have been proposed.
On both sides of the pinna but restricted to the margins, numerous follicular casts (“waxy plugs”) can be seen adhering to the skin and hair. As the disease evolves, lesions become confluent and involve the whole ear margin. Partial alopecia is observed. Later on, the debris remains tightly adherent but becomes hard and thick. Fissuring of both the aggregate and underlying skin results. This is painful and bothers the dog so that it shakes its head even more and aggravates the process.
History and careful clinical observation are usually diagnostic early in the course of the disease. As the lesions become fissured and crusty, the differential diagnosis includes most other causes of ear margin lesions such as sarcoptic mange, vasculitis, and some insect-bite dermatoses, especially stick-tight flea infestation. Severe hyperkeratosis and follicular keratosis that may lead to a pseudopapillomatous appearance are observed on dermatopathologic examination.
No underlying causes are usually associated, and the treatment is symptomatic: removing the seborrheic aggregates and decreasing further production. Ceruminolytic shampoos containing salicylic acid as well as sulfur are used regularly. Because tar has been shown to be carcinogenic in humans (squamous cell carcinoma19), it might be preferable to avoid dispensing tar-containing products; most clients do not wear gloves when applying products to their animals. To initiate the dissolution of the waxy aggregates, the lesions can be soaked 15 minutes before the shampoo with warm water or a ceruminolytic ear solution. These solutions can be irritating, especially those that contain toluene derivatives, but they are removed by the shampoo shortly after their application. Peroxide, vitamin A, or retinoids can be applied topically between shampoos to slow down the buildup of the waxy material. Gel formulations are preferred because they penetrate the coat better and do not build up as much as do ointments. Because these treatments are symptomatic, their frequency is based on the clinical appearance of lesions. When fissuring is extensive, surgical ear cropping is indicated.
Acquired Folding of the Pinna
This benign condition is reported in adult cats. The apexes of both pinnae suddenly fold rostrally and, usually, somewhat laterally (Figure 12-10). On palpation, the cartilage is usually lacking in the folded apex. Most affected cats have a history of long-term steroid treatment; when performed, adrenocorticotropic hormone (ACTH) stimulation test results are depressed. Stopping the glucocorticoid treatment may improve the condition.

Figure 12-10
Acquired folding associated with partial alopecia on both pinnae of a Siamese cat. No history of steroid treatment could be found. One year later, the ears were back to normal without treatment.
More on the topic Dermatoses of the Ear Margin:
- Crusty and Scaly Dermatoses
- Dermatoses of the Concave Pinna
- A Note in the Margin
- Pruritic Dermatoses
- Careful examination of a clean, dry ear canal in a dog or cat with otitis externa may reveal many conditions that affect the ear canal.
- Lateral Ear Canal Resection and Ear Canal Ablation
- EAR DISORDERS
- The Normal Ear
- Stenotic Ear Canals
- Ear Therapy
- Ear Mites