Cytology of the prostate
Introduction
Cytology of prostatic tissue is performed when the gland is enlarged. Good quality samples of prostatic cells may be safely collected by ejaculation, prostatic massage, prostatic wash, traumatic catheterization, and impression smears during surgery.
Note that if manual ejaculation or prostatic massage is performed, the first and third fractions contain the prostatic epithelial cells (Kustritz, 2006). Additionally, ultrasound-guided, perirectal, or transrectal FNA can yield excellent quality samples, but these procedures have some risk for seeding the abdomen with neoplastic cells if the patient has a carcinoma. Powe et al. (2004) reported that cytologic interpretations of prostatic aspirates agreed with the histopathologic diagnosis 80% of the time. Only 2 of the 25 cytology samples they evaluated were nondiagnostic due to low cellularity; both of the nondiagnostic samples were collected by ultrasound-guided FNA.Inflammation
If inflammation is present, the prostate may be uniformly enlarged or may contain soft, swollen pockets consistent with abscesses. Cytologically, the sample contains large numbers of nondegenerate to markedly degenerate neutrophils. There also should be low numbers of prostatic epithelial cells that are arranged in clusters. Prostatic epithelial cells are small and cuboidal with scant basophilic cytoplasm, distinct cell junctions, and a round nucleus with stippled chromatin (Figure 11.45). Mild anisocytosis and anisokaryosis are not commonly observed in the epithelial cell population but may be caused by dysplastic changes secondary to the inflammation. A moderate amount of blue–gray amorphous debris consistent with necrotic cellular material also may be seen. The sample should be closely examined for bacteria, especially if neutrophils appear degenerate. Infectious organisms that can cause prostatitis include bacteria (Escherichia coli, Proteus vulgaris, Brucella canis, among others), fungi (Blastomyces dermatitis, Cryptococcus neoformans, Coccidioides immitis), and parasites (Leishmania spp.) (Palmieri et al., 2022).
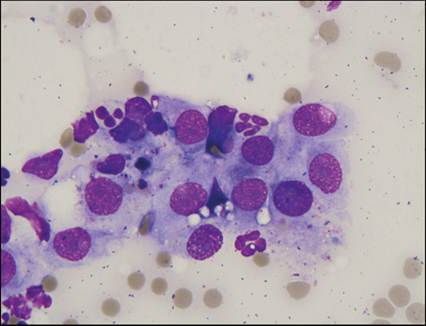
Figure 11.45 Prostatitis. Ultrasound-guided FNA of an enlarged prostate from a 12-year-old, intact male German Shepherd Dog. The image shows a slightly ruptured cluster of prostatic epithelial cells with abundant, lightly basophilic cytoplasm and a round nucleus with stippled chromatin. Closely associated with the prostatic epithelial cells are several neutrophils (Wright–Giemsa, 1,000? magnification).
Cysts
Cysts can develop in the prostate following obstruction of ducts. Clinical signs are usually associated with complications of prostatic enlargement. Fluid aspirated from prostatic cysts is typically straw-colored. Fluid cytology samples are of overall low cellularity and may contain low numbers of prostatic epithelial cells, macrophages, neutrophils, and lymphocytes (Boland et al., 2003).
Hyperplasia
Hyperplasia tends to cause uniform enlargement of the prostate, but may be irregular if cysts are present. Prostatic hyperplasia is detected in many middle-aged to older, intact dogs. Aspiration of hyperplastic prostatic tissue yields large clusters of prostatic epithelial cells with scant to moderate amounts of deeply basophilic, sometimes vacuolated, cytoplasm and a round nucleus with stippled chromatin (Figures 11.46, 11.47). Cells have a uniform appearance and lack significant criteria of malignancy. The treatment of choice for prostatic hyperplasia is castration.
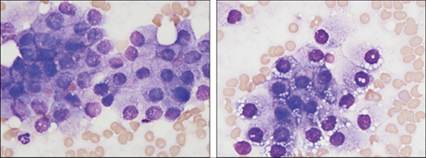
Figures 11.46,11.47 Benign prostatic hyperplasia. Transrectal FNA of an enlarged prostate from an adult neutered male Bernese Mountain Dog. Sheets of cuboidal epithelial cells with a moderate to abundant amount of basophilic cytoplasm and a round nucleus are observed. Cells often contain numerous, clear, cytoplasmic vacuoles. The nuclei are relatively uniform in diameter and have smooth chromatin.
A small, round nucleolus can be seen in low numbers of cells (Wright–Giemsa, 1,000? magnification).
Metaplasia
Squamous metaplasia may occur in the prostate following trauma, inflammation, or exposure to an increased concentration of estrogen (which may be observed with Sertoli cell tumors and interstitial tumors of the testes). It is not considered a preneoplastic process. This condition is diagnosed when mildly dysplastic squamous epithelial cells with abundant, pale, polygonal cytoplasm and a round dense nucleus are found within or near prostatic epithelial cell clusters (Figure 11.48).
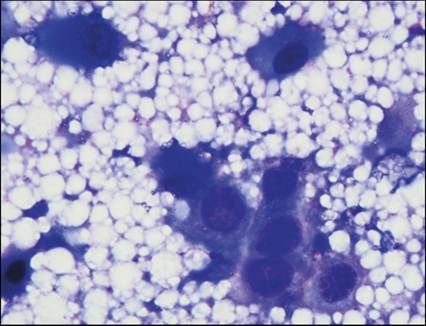
Figures 11.48 Squamous metaplasia. FNA from the enlarged prostate of a 6-year-old, neutered male Samoyed. Dysplastic prostatic epithelial cells have abundant, deeply basophilic cytoplasm and a large, round nucleus with clumped chromatin. Four individualized cells to the left and upper aspects of the image have glassier, blue, keratinized cytoplasm and a more condensed nucleus consistent with squamous metaplasia. The background is filled with basophilic proteinaceous material and lipid vacuoles (Wright–Giemsa, 1,000? magnification).
Neoplasia
Neoplastic changes in the prostate tend to form in one of the lobes of the prostate, and so the prostate palpates unevenly. The most common neoplasm of the canine prostate is prostatic carcinoma/adenocarcinoma and this can occur in intact or neutered male dogs. Transitional cell carcinomas, squamous cell carcinomas (SCCs), and mixed carcinomas are other relatively frequent neoplasms of the prostate. Less commonly, sarcomas (including fibrosarcoma, leiomyosarcoma, osteosarcoma, and hemangiosarcoma) have been reported (Foster, 2012c; Lawrence & Saba, 2013).
Prostatic/urothelial carcinoma
Cytology samples from neoplastic lesions of the prostate are often highly cellular. Morphologic differentiation between prostatic adenocarcinoma (originating from glandular prostatic epithelium) and urothelial carcinoma (originating from the prostatic urethra or periurethral ducts) is not possible without immunochemical stains.
Uroplakin III and cytokeratin 7 expression by tumor cells support a diagnosis of urothelial carcinoma, but have relatively poor sensitivity and specificity (Palmieri et al., 2022). Neoplastic cells tend to be grouped in clusters and exhibit marked criteria of malignancy. Variable amounts of deeply basophilic cytoplasm can be seen. The cytoplasm may contain numerous small, clear vacuoles or one large, clear to eosinophilic vacuole that pushes the nucleus to the edge of the cell. Nuclei are variably sized and have coarse, clumped chromatin and one or more prominent nucleoli. Binucleation, nuclear molding, and mitotic figures often are observed (Figures 11.49–11.51). Prostatic (adeno)carcinomas tend to metastasize to regional lymph nodes, lung, and bone, particularly the lumbar vertebrae. It is a very common tumor of humans, but is less common in dogs (1% of all canine tumors) and is rare in cats (Lawrence Saba, 2013b). The median survival time of dogs with prostatic adenocarcinoma is less than 30 days and most cats die within 3 months of diagnosis (Lawrence Saba, 2013c). 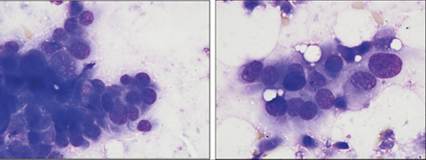
Figures 11.49,11.50 Prostatic adenocarcinoma. Ultrasound-guided FNA from the enlarged prostate of a 9-year-old, neutered male mixed-breed dog. The sample is highly cellular and has several crowded clusters of epithelial cells with rounded, lightly basophilic cytoplasm, a large rounded nucleus, and stippled to clumped chromatin. One or two prominent nucleoli are seen in low numbers of cells. Nuclear molding can be appreciated. Marked anisocytosis and anisokaryosis are observed (Wright–Giemsa, 1,000? magnification).
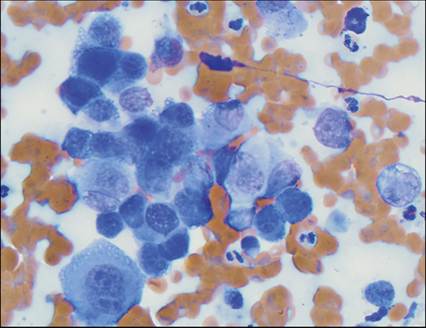
Figure 11.51 Urothelial carcinoma (metastatic). FNA of a lytic bone lesion from a 14-year-old, spayed female dog. The sample is highly cellular and has several clusters of transitional epithelial cells with rounded, lightly basophilic cytoplasm, a large round nucleus, and stippled chromatin. One to three prominent nucleoli are seen in many cells. Binucleation and nuclear molding can be appreciated. Marked anisocytosis and anisokaryosis are observed (Wright–Giemsa, 800? magnification).