Endocrine System
Thomas Colville
OUTLINE
INTRODUCTION, 275
HORMONES, 276
Characteristics, 276
Hormone Chemistry, 276
Control of Hormone Secretion, 278
THE MAJOR ENDOCRINE GLANDS, 278
The Hypothalamus, 278
The Pituitary Gland, 279
The Thyroid Gland, 282
The Parathyroid Glands, 285
The Adrenal Glands, 285
The Pancreas, 287
The Gonads, 288
OTHER ENDOCRINE ORGANS, 289
The Kidneys, 289
The Stomach, 290
The Small Intestine, 290
The Placenta, 290
The Thymus, 290
The Pineal Body, 290
PROSTAGLANDINS, 290
LEARNING OBJECTIVES
When you have completed this chapter you will be able to:
• Describe the negative feedback system that controls the production of hormones.
• List the major endocrine glands and the hormones they produce.
• Describe the structure and functions of the pituitary gland.
• Describe the effects of growth hormone, prolactin, thyroid-stimulating hormone, adrenocorticotropic hormone, follicle-stimulating hormone, luteinizing hormone, melanocyte-stimulating hormone, antidiuretic hormone, and oxytocin.
• Describe the structure of the thyroid gland.
• Describe the effects of thyroid hormone, calcitonin, and parathormone.
• Differentiate between T3 (triiodothyronine) and T4 (tetraiodothyronine, or thyroxine).
• List the three categories of hormones produced by the adrenal cortex.
• List the hormones produced by the pancreatic islet cells and describe the effects of each.
• Describe the effects of androgens, estrogens, and progestins.
• List the hormones produced by the kidneys, stomach, small intestine, placenta, thymus, and pineal body.
VOCABULARY FUNDAMENTALS
Acromegaly ahck-rδ-mehg-ah-le
Adrenal cortex ah-dre-nuhl kohr-tehx
Adrenal gland ah-dre-nuhl glahnd
Adrenal medulla ah-dre-nuhl meh-duhl-uh
Adrenocorticotropic hormone (ACTH) ah-dre-nδ-kohr- tih-kδ-trδ-pihck hohr-mδn
Aldosterone ahl-dohs-tuhr-δn
Alopecia ahl-δ-pe-shuh
Anabolism ah-nahb-uh-lihz-ehm
Androgen ahn-drδ-jehn
Anterior pituitary gland ahn-teer-e-ar pih-too-
ih -taar-e glahnd
Antidiuretic hormone (ADH) ahn-te-dι-u-reht-ihck hohr-mδn
Atrophy aht-ruh-fe
Calcitonin kahl-sih-tδ-nihn
Calorigenic kuh-lohr-uh-jehn-ihck
Catabolism kah-tahb-uh-lihz-ihm
Catecholamine kaht-ih-kδl-ih-men
Cell-mediated immunity sehl me-de-a-tehd ihm-myoo-nih-te
Cholecystokinin kδ-leh-sihs-tδ-kι-nihn
Chorionic gonadotropin kohr-e-ohn-ihck gδ-nahd-uh-trδ-pihn
Chyme kιm
Corpus luteum kohr-pahs lu-te-uhm
Cortex kohr-tehx
Diabetes insipidus dι-ah-be-tes ihn sihp-eh-dihs
Diabetes mellitus dι-ah-be-tes mehl-eh-tihs
Diuresis di-u-re-sihs
Duodenum doo-o-den-uhm
Dysfunction dihs-fuhngk-shuhn
Eclampsia ih-klahmp-se-ah
Endocrine^ιd ehn-do-krihn glahnd
Endocrinology ehn-do-krihn-ohl-uh-je
Epinephrine ehp-ih-nehf-rihn
Erythropoietin e-rihth-ro-poy-eh-tihn
Estrogen ehs-tro-jehn
Exocrine^ιd ehcks-o-krihn glahnd
Feedback mechanism fed-bahck mehck-uh-nihz-uhm
Fight-or-flight response fit or flit reh-spohns
Follicle-stimulating hormone (FSH) fohl-ih-kuhl stihm-u-la-tihng hohr-mon
Gastrin gahs-trihn
Glucagon gloo-kah-gohn
Glucocorticoid hormone gloo-ko-kohr-tih-koyd hohr-mon
Gluconeogenesis gloo-ko-ne-o-jehn-eh-sihs
Glycosuria gli-kos-yar-e-ah
Gonad go-nahd
Gonadotropin go-nahd-uh-tro-pihn
Growth hormone (GH) groth hohr-mon
Homeostasis ho-me-o-sta-sihs
Hormone hohr-mon
Hydrophilic hi-dro-fihl-ihck
Hydrophobic hi-dro-fo-bihck
Hyperadrenocorticism hi-por-ah-dre-no-kohrt-uh- kihz-uhm
Hypercalcemia hi-por-kahl-se-me-ah
Hyperglycemia hi-por-gli-se-me-ah
Hyperplasia hi-por-pla-zhuh
Hypoadrenocorticism hi-po-ah-dre-no-kohrt-uh- kihz-uhm
Hypocalcemia hi-po-kahl-se-me-uh
Hypoglycemia hi-po-gli-se-me-uh
Hypothalamus hi-po-thahl-uh-muhs
Hypoxia hi-pohx-e-ah
Iatrogenic i-aht-ro-jehn-ihck
Insulin ihn-suh-luhn
Interstitial cell ihn-tor-stihsh-halhl se
Interstitial cell-stimulating hormone (ICSH) ihn-tor-
stihsh-halhl se stihm-u-la-tihng hohr-mon
Lactation lahck-ta-shuhn
Luteinizing hormone (LH) loo-te-eh-niz-ihng hohr-mon
Luteolysis loo-te-ohl-i-sihs
Medulla meh-duhl-uh
Melanocyte-stimulating hormone (MSH) mehl-ahn-o-sit
stihm-u-la-tihng hohr-mon
Melatonin mehl-ah-to-nihn
Metabolism meh-tahb-uh-lihz-ehm
Milk fever mihlk fe-vor
Milk let-down mihlk leht-doun
Mineralocorticoid hormone mihn-or-ahl-o-kohr-tih-koyd hohr-mon
Monoamine hormone mohn-o-ah-men hohr-mon
Myoepithelial cell mi-o-ehp-ih-the-le-ahl sehl
Myometrium mi-o-met-re-uhm
Neurotransmitter nor-o-trahnz-miht-or
Nonsteroidal anti-inflammatory drug (NSAID) nohn-
stear-royd-ehl ahn-te-ihn-flahm-uh-tohr-e druhg
Norepinephrine nohr-ehp-ih-nehf-rihn
Oogenesis o-o-jehn-eh-sihs
Ovary o-vor-e
Oxytocin ohck-se-to-sihn
Pancreas pahn-kre-ahs
Pancreatic islet pahn-kre-aht-ihck i-leht
Parathyroid gland peor-ah-thi-royd glahnd
Parathyroid hormone (PTH) peor-ah-thi-royd
hohr-mon
Parturition pahr-tuhr-ih-shuhn
Pmeopntied e hor pehp-tid hohr-mon
Pineal body pi-ne-ahl boh-de
Pinuitary^ιd pih-too-ih-teor-e glahnd
Placenta pluh-sehn-tah
Polydipsia pahl-e-dihp-se-ah
Polyphagia pahl-e-fa-je-ah
Polyuria pahl-e-yar-e-ah
sPtoermta l sy pohr-tehl sihs-tehm
Posterior pituitary gland po-steer-e-or pih-too-ih-teor-e
glahnd
Precursor pre-kuhr-sor
Progesterone pro-jehs-tor-on
Progestin pro-jehs-tihn
Prohormone pro-hohr-mon
Prolactin pro-lahck-tuhn
Prostaglandin prohs-tuh-glahn-duhn
Prostate^ιd prah-stat glnhnd
Secretin seh-kret-ihn
Seminal vesicle sehm-ihn-uhl vehs-uh-kuhl
Sex hormone sehx hohr-mon
Spermatogenesis spor-mah-to-jehn-eh-sihs
Steroid hormone stear-oyd hohr-mon
Superovulation soo-por-ohv-u-la-shuhn
Target tahr-giht
Testes tehs-tes
Testosterone tehs-toh-stor-on
Tetraiodothyronine (T4) teht-ruh-i-o-do-thi-ro-nen
(tee fohr)
Thymopoietin thi-mo-poy-e-tehn
Thymosin thi-mo-suhn
Thymus thi-muhs
Thyroid ^ιd thi-royd glahnd
Thyroid hormone thi-royd hohr-mon
Thyroid-stimulating hormone (TSH) thi-royd stihm-u-
la-tihng hohr-mon
Thyroxin thi-rohck-sihn
Triiodothyronine (T3) tri-i-o-do-thi-ro-nen
(tee thre)
Unsaturated fatty acid uhn-sahch-or-ra-tihd faht-e
ah-sihd
INTRODUCTION
The endocrine system and the nervous system share the work of controlling and coordinating all the intricate parts and functions of the animal body.
Put most simply, the two systems each help maintain homeostasis (balance) in the body. They constantly send instructions to the rest of the body, telling it how to respond to changes in internal and external conditions.Table 11-1 summarizes the similarities and differences between the endocrine and nervous systems, but let's discuss some of the main ones. Both systems use chemicals to transmit their messages, but they do it by different means. The endocrine system messengers, hormones, are produced by endocrine gland cells, or modified neurons. They travel through the bloodstream to distant cells and tissues, where they produce their effects. The nervous system messengers, called neurotransmitters, are produced only by neurons. They travel very short distances across synaptic spaces to produce their effects. The targets of hormones are all of the cells and tissues in the body. The targets of neurotransmitters are generally only muscle cells, glands, and other neurons. The endocrine system reacts slowly to changes but can sustain its responses for long periods. The nervous system reacts quickly to changes but cannot sustain prolonged responses.
The basic units of the endocrine system are endocrine glands. Located throughout the body, endocrine glands secrete tiny amounts of hormones directly into the bloodstream. This method of secretion gives them the nickname ductless glands. This feature differentiates them from exocrine glands (exo means "out" or "external"),
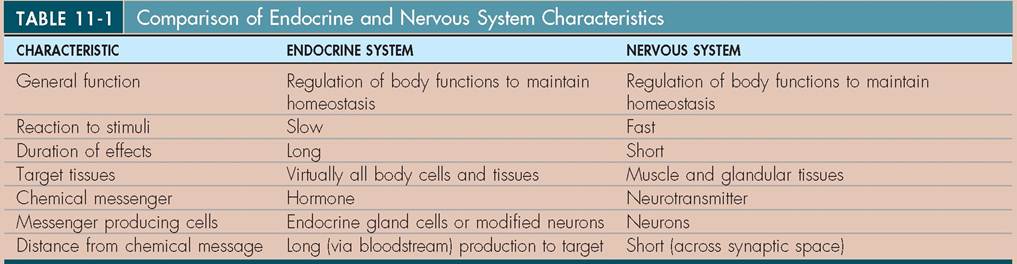
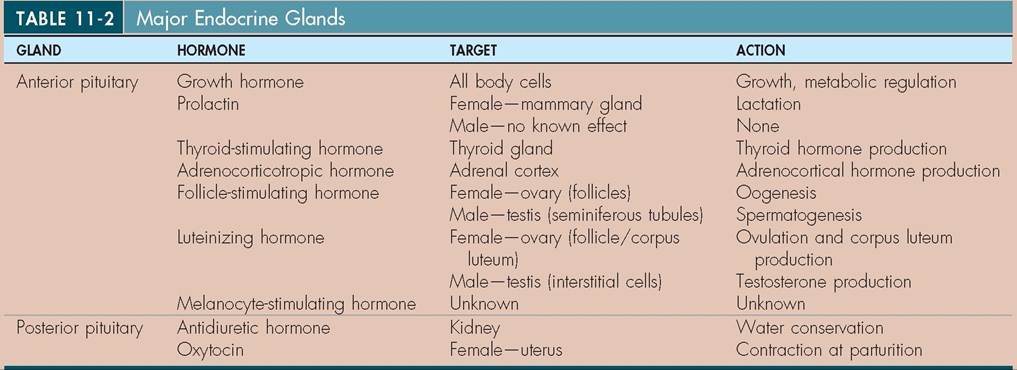
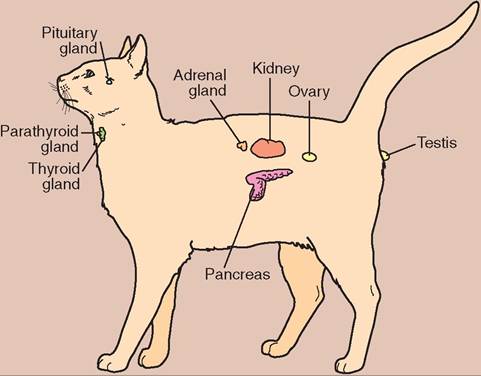
FIGURE 11-1 Relative locations of major endocrine glands in the cat. (Modified from McBride DF: Learning veterinary terminology, ed 2, St Louis, 2002, Mosby.)
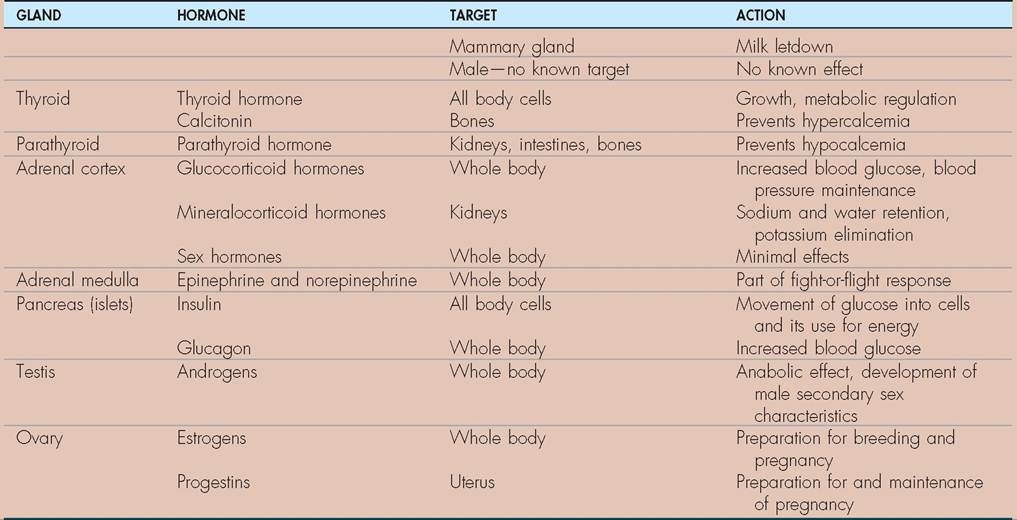
TABLE 11-2 Major Endocrine Glands—confd
which secrete their products onto epithelial surfaces through tiny tubes called ducts.
The hormones produced by the endocrine glands circulate throughout the body in the blood and produce effects whenever they find specific receptors to which they can attach, either in or on cells.Endocrine glands are found throughout the body, and the list of them grows as we learn more about endocrinology. In this chapter we focus mostly on the major endocrine glands. Table 11-2 summarizes the major endocrine glands and their hormones, and Figure 11-1 shows their relative locations in the body. Like many other parts of the body, hormones and endocrine structures are known by more than one name or abbreviation. We use common clinical veterinary usage as our guide, with alternative terms included where appropriate for clarity.
TEST YOURSELF 11-1
1. How do endocrine glands differ from exocrine glands?
2. In what ways are the functions and characteristics of the endocrine system similar to those of the nervous system? In what ways are they different?
HORMONES
CHARACTERISTICS
Hormones are chemical messengers produced by endocrine glands and secreted directly into blood vessels. They travel in the bloodstream to all parts of the body and produce effects only when they bind to their particular receptors in or on cells. Figure 11-2 shows examples of cell membrane and intracellular receptor binding. Each body cell has specific receptors for a variety of hormones. These receptors are like locks into which only specific keys (hormones) can fit. When a hormone (key) binds to its receptor (lock) in or on a cell, it changes some activity of that cell. If a cell does not have receptors to a particular hormone, that hormone just passes by and has no effect on that cell. A cell that has receptors for a particular hormone is referred to as a target of that hormone.
HORMONE CHEMISTRY
Animal hormones have diverse chemical structures, but they can be categorized into three main groups: peptide hormones, steroid hormones, and monoamine hormones. Box 11-1 shows which major hormones belong to each group.
Peptide hormones consist of chains of a few to 200 or more amino acids arranged like pearls in a necklace. They are hydrophilic (soluble in water), so they can easily travel in the blood plasma, which is mostly water. Receptors for peptide hormones are located on the cell membranes of their target cells.
Steroid hormones are lipids that are synthesized from cholesterol (Figure 11-3). They are hydrophobic (insoluble in water), so they must bind to hydrophilic transport proteins in order to travel in the plasma. The portion of hormone molecules that are attached to transport protein molecules is called “bound hormone,” and the portion that is not attached is called “unbound, or free, hormone.” Only the free fem of the hormone can leave the bloodstream and reach a target cell. Receptors for steroid hormones are iocated within the cell—either in the cytoplasm or the nucleus. The lipid structure of these hormones allows them to pass easily through the cell membrane to reach their receptors.
Monoamine hormones are; derived from amino acids aetnadinr an amino group, which gives the group its name.
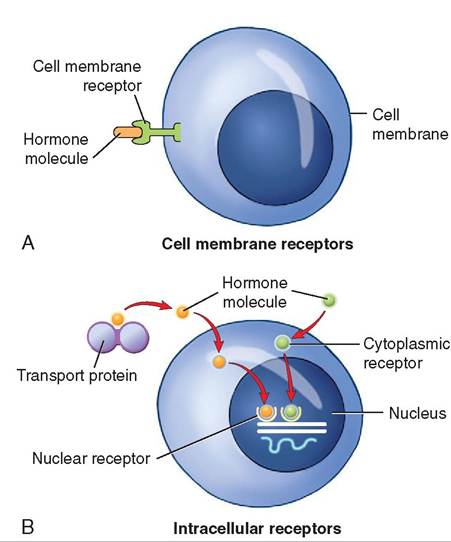
FIGURE 11-2 Hormone receptor binding. A, Water-soluble hormones such as peptides anb catecholamines bind to receptors on the cell membrane. B, Lipid-soluble hormones such as steroid and thyroid hormones pass through the cell membrane and bind to receptors in the cytoplasm or nucleusi
The catecholamine IiotanOTes (epinephrine and norepinephrine) are hydrophilic, and are transported dissolved in the plasma like the peptide hormones. Thyroid hormones, however, are hydrophobic like the steroid hormones, and require transport proteins. Receptors for catecholamine hormones are located on the cell membranes of their target cells,
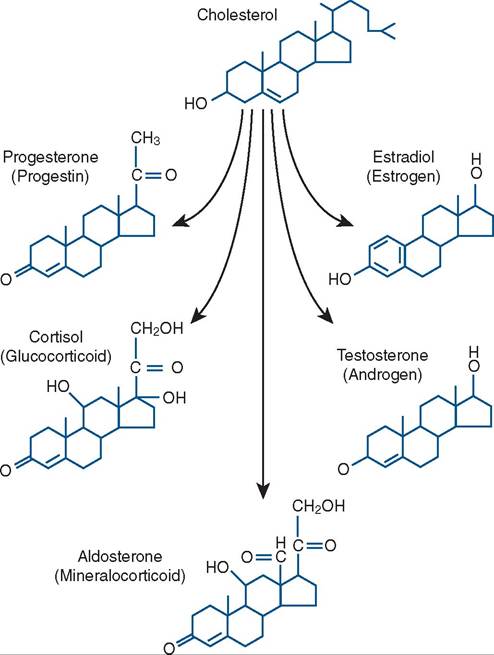
FIGURE 11-3 Structure oo steroid normones.
BOX 11-1 Chemical Categori es of Hormones
Monoamine
• Catecholamines (e.g., epinephrine and norepinephrine)
• Thyooid hormones
Peptide Hormones
• Adrenocorticotropic hormone (ACTH)
• Antidiuretic hormone (ADH)
• Calcitonin
• Cholecystokinin
• Chorionic gonadotropin
• Erythropoietin
• Follicle-stimulating hormone (FSH)
• Gastrin
• Glucagon
• Growth hormone (GH)
• Insulin
• Luteinizing hormone (LH)
• Melanocyte-stimulating hormone (MSH)
• Melatonin
• Oxytocin
• Parathyroid hormone (PTH)
• Prolactin
• Relaxin
• Secretin
• Thymic normones(o.g.r thymopoietin)
• Thyroid-stimulating hormone
Steroid Hormones
• Androgens (e.g., testosterone)
• Eistrogens (e.g., estradiol)
• Glucocorticoid hormones (e.g., cortisol)
• Mineralocorticoid hormones (e.g., aldosterone)
• Progestins (e.g., progesterone) whereas receptors for thyroid hormones are located in the nucleus, like those for some of the steroid hormones.
CONTROL OF HORMONE SECRETION
Hormone secretion is commonly controlled by what are called feedback systems. This means that the level of hormone in the blood directly or indirectly “feeds back” to the gland that produced it and affects the activity of the gland. If the activity is decreased by rising levels of the hormone, the feedback is said to be negative feedback. If the activity is increased by falling levels of the hormone, the feedback is said to be positive feedback.
Negative hormonal feedback systems are the most common type in the animal body. They function in a similar fashion to a thermostatically controlled room heater on a cold day. When the heater's thermostat is set to a temperature higher than the current ambient temperature, the heater is turned on to heat the air. When the room's rising temperature reaches the thermostat setting, the heater is turned down or off. Without a source of heat, the air in the room cools. When the temperature falls below the thermostat setting, the heater is turned back on again, and so forth. The rising temperature of the room air feeds back to the thermostat and has a negative effect on the heater; that is, the heater is turned down or off. This is an example of a negative feedback system.
The secretion of many hormones is controlled in a similar fashion. For example, let's assume the “heater” is the thyroid gland, which produces its hormone as a result of stimulation by another hormone, called thyroid-stimulating hormone (TSH), from the anterior pituitary gland. When the level of thyroid hormone drops below needed levels—the “thermostat setting”—the anterior pituitary produces more TSH, which stimulates the thyroid gland to produce more of its hormone. This “turns on” the heater (thyroid gland) and tells it to produce more heat (thyroid hormone). The rising level of thyroid hormone in the bloodstream eventually reaches the level required in the body. Once that level is reached, the production of TSH by the anterior pituitary is turned down.
This reduces the stimulation of the thyroid gland, causing it to produce less thyroid hormone (the heater has been turned down). When the level of thyroid hormone again drops below what the body needs, the anterior pituitary ramps up its production of TSH, which turns the production of thyroid hormone back up, and the process continues.Positive feedback systems, in which rising levels of hormone produced by a gland feed back and further increase hormone production, are less common, because of their potential to lead to “vicious cycles” of out-of-control hormone production. Positive feedback systems do play specific, limited roles, for example in the complicated interplay of hormones involved in the female estrous cycle, but the system they are part of prevents vicious cycles of hormone production from developing.
One endocrine gland uses a totally different, non-feed- back-related control mechanism for hormone secretion— direct stimulation from the nervous system. The secretion of hormones from the medulla of the adrenal gland is directly stimulated by sympathetic nerve impulses when an animal feels threatened. The adrenal medullary hormones that are released into the bloodstream as a result of this stimulation contribute to the whole-body fight-or-flight response that prepares the animal's body for intense physical activity. (The adrenal gland is discussed more fully later in this chapter.)
TEST YOURSELF 11-2
1. What is a hormone?
2. What is a hormone target?
3. What are the three main chemical groups of hormones?
4. Which chemical hormone group(s) bind to receptors on the target cell membrane? In the cytoplasm or nucleus?
5. How does the negative feedback system control the secretion of many hormones?
THE MAJOR ENDOCRINE GLANDS
THE HYPOTHALAMUS
CHARACTERISTICS
The hypothalamus is a part of the diencephalon of the brain. It is located in the ventral part of the brain just caudal to the optic chiasma, where the optic nerves partially cross. It has many important nervous system functions, including appetite control, body temperature regulation, and control of wake-sleep cycles. It also links the conscious mind with the rest of the body by connecting higher centers in the cerebral cortex with lower brain centers and the endocrine system. This link with the endocrine system is accomplished through the control the hypothalamus has over the activities of the pituitary gland. This makes it a very important bridge between the nervous system and the endocrine system.
Relationship with pituitary gland
The pituitary gland is an endocrine gland that is located ventral to the hypothalamus and is attached to it by a slender stalk. Blood vessels and nerve fibers in the stalk enable the hypothalamus to control the activity of the pituitary gland and therefore most of the rest of the body.
A system of tiny blood vessels called a portal system links the hypothalamus with what is called the anterior portion of the pituitary gland. Figure 11-4 shows this pituitary portal system. Modified neurons in the hypothalamus secrete hormones into these portal blood vessels. The hormones travel the short distance down to the anterior pituitary and regulate much of its function. These hypothalamic hormones, called releasing and inhibiting factors, are each specific for a particular anterior pituitary hormone. As their name implies, a releasing factor causes the anterior pituitary to produce and release a particular hormone, and an inhibiting factor has the opposite effect, inhibiting the production and release of a hormone. Because some anterior pituitary hormones influence all of the body's cells, the hypothalamus indirectly affects the whole body by
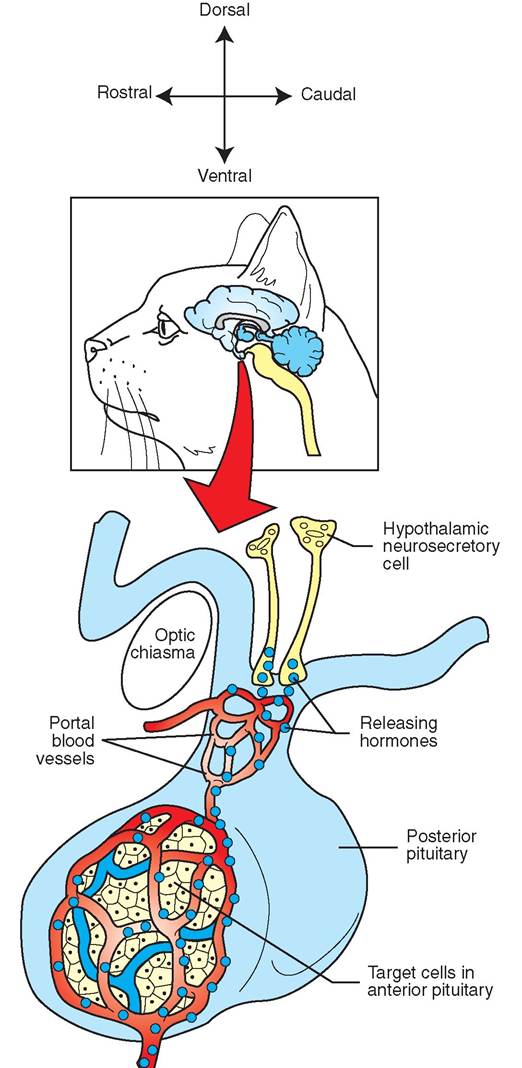
FIGURE 1 1 -4 Relationship of hypothalamus and anterior pituitary. Releasing and inhibiting hormones from the hypothalamus are secreted into portal blood vessels that carry them to the anterior pituitary. There they stimulate or inhibit release of anterior pituitary hormones.
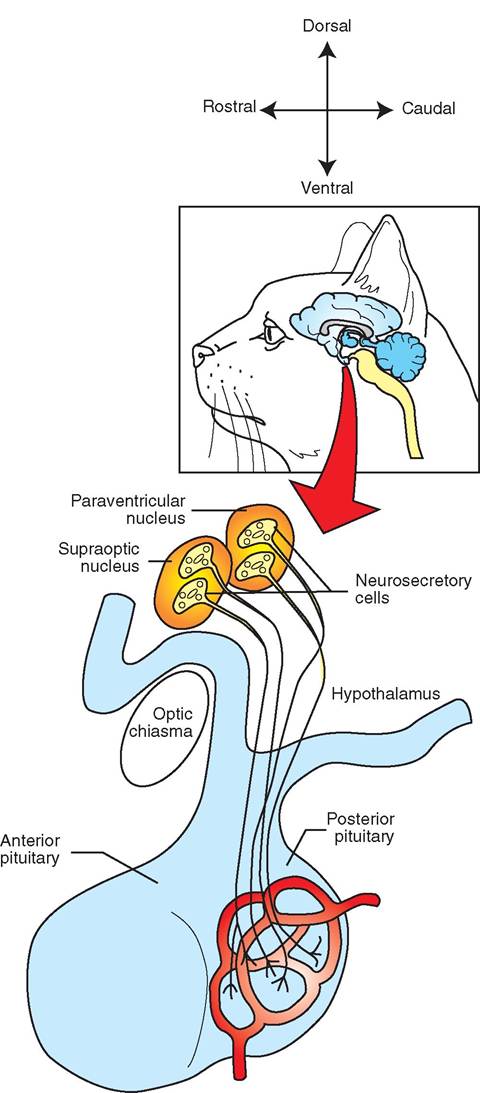
FIGURE 11-5 Relationship of hypothalamus and posterior pituitary. Neurosecretory cells (modified neurons) in the hypothalamus produce hormones that are transported down nerve fibers to the posterior pituitary, where they are stored. Their release is controlled by nerve impulses from the hypothalamus.
regulating anterior pituitary gland functions. In part, this is how the state of an animal's mind can influence its susceptibility and reaction to illnesses.
The effect of the hypothalamus on the posterior part of the pituitary gland is more direct. Modified neurons in the hypothalamus produce two hormones, antidiuretic hormone (ADH) and oxytocin, which are transported down nerve fibers (axons) to the posterior pituitary gland, where they are stored. They are then released into the bloodstream by nerve impulses from the hypothalamus. Figure 11-5 illustrates this process.
THE PITUITARY GLAND
CHARACTERISTICS
The pituitary gland (also referred to as the hypophysis) is often called the master endocrine gland because many of its hormones direct the activi ty of other endocrine glands around the body. Physically the pituitary gland is tiny, about the size of a small pea Ot bean. It is connected to the hypothalamus above it by a slender stalk and is securely housed in a small pocket in the sphenoid bone of the skull called the pituitary fossa.
Although it looks like one structure, the pituitary gland is actually two separate glands with completely different structures, functions, and embryologic origins. The rostral (front) portion is called the anterior pituitary, or the adenohypophysis. It develops from glandular tissue in an embryo eaonkds lo lik normal glandular tissue under the microscope. The caudal (rear) portion is called the posterior pituitary, or the neurohypophysis. It Jowlops from the embryo's nervous system and looks like nervous tissue under the microscope.
Thn functions of the two parts of the pituitary gland are as different as their appearance. The anterior pituitary produces seven known hormones, when stimulated by the hypothalamus and direct feedback from target organs and tissues. The posterior pituitary does not produce any hormones. Rather, it stores and releases two hormones that are produced in the hypothalamus and transported to the posterior pituitary along nerve fibers.
THE ANTERIOR PITUITARY
oTlhloewfing are the seven known anterior pituitary hormones:
• Growth hormone
• Prolactin
• Thyroid-stimulating hormone
• Adrenocorticotropic hormone
• Follicle-stimulating hormone
• Luteinizing hormone
• Melanocyte-stimulating hormone
GROWTH HORMONE. Growth hormone (GH) is also known as somatotropin and somatotropic hormone. Its name oomes from its most obvious effect—the promotion of body growth in young animals, particularly the growth of bone and muscle. It has other important roles in animals of all ages, however. It helps regulate the metabolism of proteins, carbohydrates, and lipids in all of the body's cells.
The effect of GH on protein metabolism is to encourage the anabolism,r o synthesis, of proteins by body cells. This supplies the materials for growth, as well as for the ongoing regeneration and repair of body tissues that have undergone injury or normal wear and tear.
fTfehcetse of GH on carbohydrate and lipid metabolism are linked. GH causes the mobilization (release) of lipids from storage in adipose (fat) tissue and their catabo- lismre(bakdown) in body cells for energy production. At itmhee,same t it discourages the cells from using carbohydrates, especially glucose, as energy sources. Because less egmlucoovseed is r from the blood by the cells, the level of glucose in the blood tends to rise. This is called a hyperglycemic effect. This effect is opposite to that of the pancreatic hormone insulin, which tends to lower blood glucose levels. Because glucose is such an important energy source foodry'tshe b cells, a balance between GH and insulin is iomportant t maintaining homeostasis of glucose levels in ltohoedb.
CLINICAL APPLICATION
Growth Hormone (GH)
Because of its whole-body effects, deficiencies or excesses of GH can produce some very obvious effects. The most pronounced effect of a GH deficiency is dwarfism, a condition in which a young animal does not grow normally. Other, less dramatic effects of GH deficiency relate to its metabolic effects and interrelationships with other hormones and endocrine glands. These can include alopecia (hair loss), thin skin, and development of secondary abnormalities of thyroid, adrenal, and reproductive hormones. Animals with eGfiHciedncies often respond to the therapeutic adminis- ftration o GH. An excess of GH can result in a form of gigantism referred to as acromegaly. The cause of this condition is often a pituitary gland tumor.
yAntshetic GH-like drug is also used to increase milk production in dairy cows. The drug bovine somatotropin (BST) is used for its generalized anabolic effect, which ehnehances t production of milk by the mammary glands. As it often the case with hormone-related drugs, some potentially isdereious s effects are associated with the use of BST. The drug is hewn to elevate animals' body temperatures, reduce conception rates, increase the risk of mammary gland infection (mastitis), and increase the risk of digestive disorders.
PROLACTIN. Prolactin is named for its effect in the female. ft helps trigger and maintain lactation, tire secretion of milk by the mammary glands. Once lactation has begun, prolactin production and release by the anterior pituitary golnatninduce as long as the teat or nipple continues to be stimulated by nursing or milking. If nursing or milking ceases, the production of prolactin will cease as well. Without stimulation from prolactin, the mammary gland “dries up,” rmoidlkucption stops, and the mammary gland shrinks boack t its nonlactating size. In the male, prolactin has no ekcniofiwc n sp function.
THYROID-STIMULATING HORMONE. Thyroidstimulating hormone (TSH) is also known as thyrotropic hormone. As its name implies, it stimulates the growth and development of the thyroid gland and causes it to produce its hormones. Increased TSH secretion increases thyroid hormone production and vice versa. TSH secretion is regu- leyaetdebdabck f from its target organ—the thyroid gland. cTchuirsso both through direct effects on the anterior pituitary gland and through changes in TSH-releasing factor yproduced b the hypothalamus. If thyroid hormone levels rise higher than the body needs, TSH production diminishes. Witft less sti m illation, the thyroid gland decreases its hormone production, causing the thyroid hormone level in the bloodstream to drop. If the level drops too low, TSH production increases, stimulating the thyroid gland to increase its hormone production again. Homeostasis of thyroid hormone production is maintained through this interaction among the hypothalamus, anterior pituitary gland, and thyroid gland.
ADRENOCORTICOTROPIC HORMONE. Adrenocorticotropic hormone (ACTH) stimulates the growth and development of the cortex (outer portion) of the adrenal gland and the release of some of its hormones. Its production is generally regulated by feedback from the hormones of the adrenal cortex in rwh the same manner as TSH production iesgur lated by feedback from thyroid hormones. In times of sudden stress to an animal, however, ACTH can be released quickly us a result of stimulation of the hypothalamus by other harts of the brain. When stimulated in this way, the hypothalamus sends a burst of ACTH-releasing factor down to the ante- irtiuoirtapry through the portal system of blood vessels that lhinemks, t which causes ACTH to be released quickly.
Follicle-Stimulating hormone. Folliclestimulating hormone (FSH) is another hormone that is onramed f its effect in the female. It stimulates the growth and development of follicles in the ovaries. Etoh follicle is an “incubato” for a single, large female reproductive cell (otchyete)o, which develops and matures as the follicle enlarges. This process is termed oogenesis. FSH also stimulates the lining cells of the follicles to produce and secrete estrogens, which are the female sex hormones. Estnogens easrpe ornsible for the physical and behavioral changes that
prepare the female for breeding and pregnancy.
In the male, FSH has an effect similar to one of its effects in the female. It stimulates spermatogenesis, the development of male reproductive cells, the spermatozoa, in the seminiferous tubules of the testes.
CLINICAL APPLICATION
Superovulation
Drugs like FSH are often used to “oupeeovulale” animals in preparation for embryo transfer. They cause the ovaries to orodure mo re follicles and ova than normal. This production hf Ijrger ⅛ιn normal numbers of ova is called superovulation. Once the animal is bred, the resulting fertilized embryos are eearieved from the uterus (usually by flushing) before they implant in its wall. They can then be transferred to other recipient animals, whose IsItous cycles have been synchronized with the donor animal, for the remainder of the gestation (pnegnancyj period. This allows females of particularly good genetic stock to produce more offspring in their lifetimes tohramnanl reproductive mechanisms would allow.
LUTEINIZING HORMONE. Luteinizing hormone (LH) is yht another hormone whose name is derived from its effect in tire female. (Are you seeing a pattern here?) LH completes the process of follicle development in the ovary that was started by FSH. As a follicle grows, it produces increasing amounts of estrogens that feed back to the hypothalamus and anterior pituitary. They cause the production of FSH to necrease and the production of LH to increase. By the time a follicle is Mly mature, LH levels reach a peak. In most animal species, this causes ovulation, or rupture of the mature follicle and subnequent release of the reproductive cell. Once ovulation has occurred, the high LH level stimulates the cells left behind in the empty follicle to multiply and develop into anothen endocrine structure—the corpus luteum. Thu ∞rpus luteum produces progestin hormones, principally progester- onei w⅛h will be necessary for the maintenance of preg- noncy should it occur. In the male, LH stimulates cells in the testes called interstitial cells to dovelop and produce the male sex hormone testosterone. Theodore LH is sometimes called interstitial cell-stimulating hormone (ICSH) in the male.
FSH and LH are sometimes grouped together under the term gonadotropins, bautinse they stimulate the growth and development of the gonads—the ovaries and testes.
MELANOCYTE-STIMULATING HORMONE. Everything in the animal body exists for a reason, although the reason may just be that something is left over from some iong-ago time in the species’ history. That seems to be the case with our little toe and a horse’s splint bones. Melanocytestimulating hormone (MSH) may be another remnant of an ea⅛r time, but we have no conclusive evidence one way or the other. MSH is associated with control of color changes in the pigment cells (melanocytes) of reptiles, fish, and amphibians—animals that can rapidly change colors and eolor patterns. Administration of artificially large amounts of MSH to higher mammals can cause darkening of the skin from melanocyte stimulation, but its effect at normal physiologic level.s is not known. Does it have some important role that we are not yet aware of? The jury is still out.
THE POSTERIOR PITUITARY
Unlike the very busy anterior pituitary, the posterior pituitary, also called the neurohypophysis, ddes not produce any hormones. Instead, it serves as a place for two hormones produced in the hypothalamus to be stored for periodic release into the bloodstream. Antidiuretic hormone and oxytocin are dransported along nerve fibers down to the poste- rioa pituitary and stored there in nerve endings. Nerve impulses from the hypothalamus tell the nerve endings when to release them into the bloodstream.
ANTIDIURETIC HORMONE. aTmh e n antidiuretic hormone (ADH) taUs us what it does. It helps prevent diuresis, w⅛h is the loss of large quantities of water in the urine. Put more plainly, it helps the body conserve water in times of short supply by acting on the kidneys. ADH causes the kidneys teoabrsorb more water from the urine they are producing back too the bloodstream. This makes the resulting urine more cr^ne^^^toιted than it would have been otherwise. Concentrated urine has a deeper color and a stronger odor.
eA-DH is released when the hypothalamus detects a water shortage (dehydration) in the body. When an animal becomes a little dehydrated, the osmotic pressure oo the blood increases (the blood becomes more concentrated), producing a condition called hemoconcentration. Reveators in the hypothalamus detect this change. This triggers nerve impulses that travel down to the posterior pituitary and cause the release of ADH. The ADH travels to its target organ, the kidney, and causes it to conserve water by producing urine that is more concentrated.
An interesting side note is that ADH release is inhibited by alcohol and caffeine. So, if we attempt to relieve thirst by drinking alcoholic beverages or caffeine-containing drinks, such as colas or coffee, we can actually produce the opposite effect. By putting the brakes on ADH release, these substances allow more water to flow out of the body in the urine. This worsens the hemoconcentration, making the thirst worse instead of better in the long run. So your mother's advice is accurate: The best thing to drink when you are thirsty is water! Moms are pretty smart.
A deficiency of ADH in the body causes the disease diabetes insipidus. Affected animals produce large quantities of very dilute urine (polyuria) and drink large quantities of water (polydipsia). Other disease conditions also produce polyuria and polydipsia, therefore a complete diagnostic workup is necessary to confirm the diagnosis of diabetes insipidus. The condition is treated by administering a drug with ADH activity for the rest of the animal's life.
OXYTOCIN. The two targets for the hormone oxytocin are the uterus and the mammary glands. In the uterus, oxytocin causes contraction of the myometrium (the muscle of the uterus) at the time of breeding and at parturition. At the time of breeding, oxytocin induces uterine contractions that aid the transport of spermatozoa up to the oviducts. When parturition (the birth process) begins, oxytocin stimulates strong uterine contractions that aid in the delivery of the fetus and the placenta. During a prolonged or difficult labor, oxytocin in the form of an injectable drug is sometimes given to dams to help strengthen weak uterine contractions. However, the myometrium may be “burned out” by overstimulating it with oxytocin, so good clinical judgment must govern its use.
The effect of oxytocin on active (milk-producing) mammary glands is to cause what is called milk let-down, or the movement of milk down to the lower parts of the gland. As milk is produced, it accumulates in the alveoli (milk-producing structures) and small ducts in the upper part of the mammary gland. Stimulation of the teat or nipple by nursing or milking causes oxytocin to be released into the bloodstream. The oxytocin circulates down to the mammary gland and causes the musclelike myoepithelial cells around the alveoli and small ducts to contract. This squeezes milk down into the lower parts of the gland, where it is accessible for nursing or milking. Usually the lag time lasts from a few seconds to a minute or two, from the time teat stimulation starts to when milk flow caused by milk let-down begins. This is how long it takes for the sensory stimulation to reach the brain and signal the hypothalamus to release oxytocin from the posterior pituitary and for the oxytocin to reach the mammary gland via the blood circulation.
Recent studies suggest that oxytocin may play roles in human, and perhaps other animal, behaviors such as social group recognition, pair connection and maternal-neonate bonding. You may hear it referred to as the “cuddle hormone” or the “bonding hormone.” This is an emerging area of knowledge that may help us better understand normal and abnormal social and bonding behaviors. Put “oxytocin” into your favorite internet search engine to see what the current state of knowledge is. As always, however, carefully consider the source of internet information before accepting it as factual.
TEST YOURSELF 11-3
1. Through what mechanisms does the hypothalamus control the production or release of hormones from the pituitary gland? How do its effects on the anterior and posterior portions of the pituitary differ?
2. Why is the pituitary gland referred to as the master endocrine gland?
3. Other than promoting growth in young animals, what are some of other effects of GH?
4. What stimulates the continued release of prolactin during lactation?
5. Do FSH and LH play important roles in male animals? If so, what are they?
6. Does ADH help promote or prevent the loss of large amounts of water in the urine? What effect would the inhibition of ADH release have on the body?
7. When milking a cow by hand, why does it take a minute or two of teat stimulation before milk starts to flow freely?
THE THYROID GLAND
CHARACTERISTICS
The thyroid gland consists of two parts called lobes that are located on either side of the larynx. The lobes may be connected by a narrow band called an isthmus, depending on the animal species. Figure 11-6 shows how the thyroid glands appear in several species. Microscopically the thyroid gland has an odd appearance (Figure 11-7). It is composed of tens of thousands of tiny follicles, where thyroid hormone is produced. Each follicle consists of a little sphere of simple, cuboidal glandular cells surrounding a globule of the thyroid hormone precursor (the raw material for thyroid hormone) they have produced. The thyroid hormone precursor in the globule is called colloid. The thyroid gland is the only endocrine gland that stores large amounts of hormone precursor for later use.
The thyroid gland produces two hormones: thyroid hormone, which mainly helps regulate the body's metabolic rate, and calcitonin, which helps regulate blood calcium levels.
THYROID HORMONE
Thyroid hormone is produced when TSH from the anterior pituitary gland stimulates the thyroid gland. It is actually two hormones: T4 (tetraiodothyronine, or thyroxine), which is considered a prohormone, and T3 (triiodothyronine), which is the active hormone. Their names are derived from the number
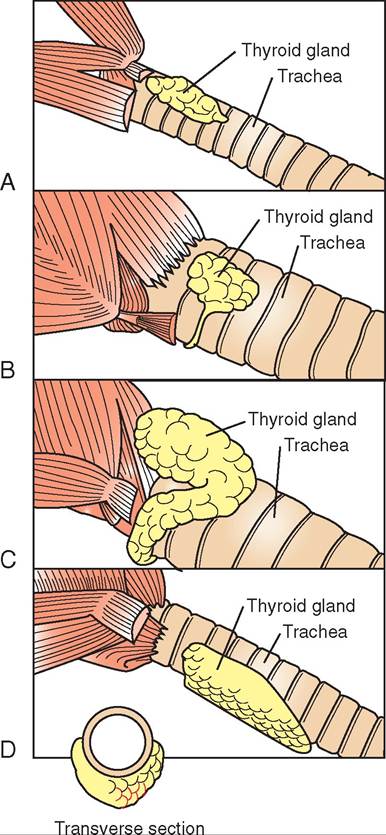
FIGURE 11-6 The thyroid glαn dsofseveral species. The inset cross section vhαwv the ventral cαddectiαd of the thynαid glande id the pig. A, Dog. B, Horse. C, Ox. D, Pig.
of iodine atoms each molecule of hormone contains. T4 contains four iodine atoms per molecule, and T3 cenioins three. The thyroid gland produces far more T4 tlnυι T3, but T3 ie the most biologically active form of thyroid hormone. The T4 fιιrιc- tions as a circulating reservoir. It is converted to T3in pee^era! tissues, mainly the liver, kidney and muscle, as needed.
CalorIGENIC EFFECT. Thyroid hormone’s calorigenic effect helps heat the body. It regulates the metabolic rate of all the body’s cells, that is, the rate at which they burn nutrients te produce energy. Thyroid hormone's influence over the metabolic rate of the body’s cells allows an animal to generate heat and maintain a constant internal body tem- herature ⅛n the temperature of the outside world changes. The prod action of thyroid hormone increases with exposure to cera temperatures. This response increases the body’s amte,tabolic r which generates more heat. It also causes
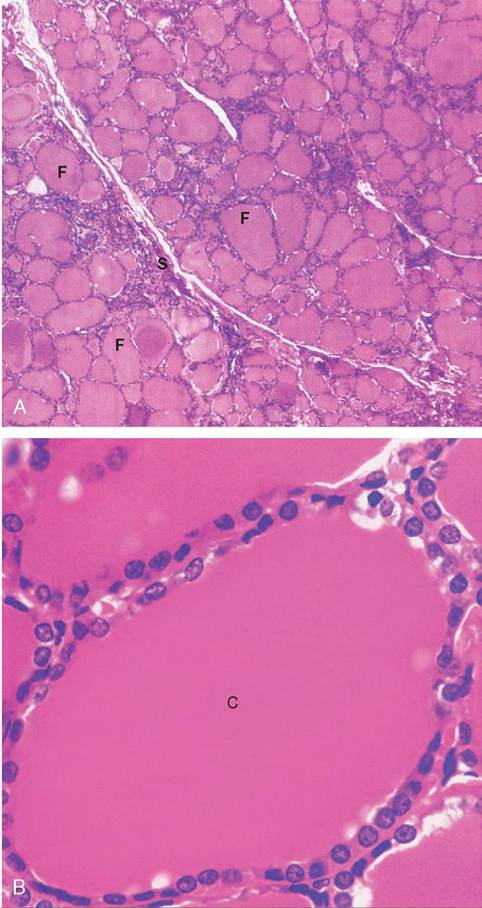
FIGURE 11-7 Photomicrographs of the thyroid gland at low (A) and high (B) magnification. C, colloid; F, thyroid follicles; S, connective tissue septa. (From Koeppen B, Stanton B: Berne & Levy physiology [updated], ed 6, St Louis, 2010, Mosby.)
nutrients to be burned at a faster rate; so animals housed outdoors in cold temperatures need to be fed more calories than those kept in warmer temperatures, to prevent signifi- fcant loss o body weight. The level of thyroid hormone can be thought of as the body’s internal “temperature setting.”
rTmhyornoeid ho production can be inhibited by emotional or pIiysical stresses on an animal. Under cold conditions, this effect can cause them to have difficulty maintaining teohmdeypirerbaturest. This in turn can compound the
spterness and o the door to disease. In otherwise healthy onimals, ∞ld temperatures alone usually do not cause disease outbreaks. However, if stress is added, animals can become umsocerep tsible and disease outbreaks can occur.
EFFECT ON PROTEIN, CARBOHYDRATE, AND LIPID METABOLISM. Thyroid hormone also affects the metabolism of proteins, carbohydrates, and lipids, much like GH fes. It encourages the anabolism, or synthesis, of proteins if the animal's diet contains adequate energy sources. If the diet is deficient in energy foods, or if the amount of thyroid hormone is excessive, the opposite can occur— protein catabolism or breakdown. The effect on carbohy- tdarbaotelismme is a hyperglycemic effect. Through several
mechanisms, thyroid hormone helps maintain homeostasis of the blood glucose level by helping to prevent it from drop- opwio.ng t lo The effect on lipids is to encourage their catabolism, or breakdown.
EFFECT ON YOUNG, GROWING ANIMALS. Thyroid hormone is necessary for normal growth and development in young animals. In particular, it influences the development and maturation of the central nervous system and the growth and development of muscles and bones.
CALCITONIN
Calcitonin, the other hormone produced by the thyroid gland, has an entirely different role. It is produced by C cells located between the thyroid follicles. Calcitonin is one of two hormones involved in maintaining homeostasis of blood calcium levels (the other is parathyroid hormone). Calcium is a vatal substance in the body. It is involved in many impor- toadnyt b functions, such as muscle contraction, blood clot- tcirnegti,omn,ilk se and formation and maintenance of the shkeeleton. T level of calcium in the bloodstream must be iktehpint w a narrow range to allow these functions to take
place o⅛>ut any difficulty.
The ;Oon of calcitonin is to help prevent hypercalcemia (xacnesseively high blood calcium level) by decreasing the bulmood calci level if it gets too high. It does this mainly by encouraging the excess calcium to be deposited in the bones. This is life putting money in the bank, knowing that you can cgko ba and take it out later if you need it. The bones are the body's “calcium bank.”
∕j CLINICAL APPLICATION
Thyroid Dysfunction
Because of the thyroid's many important roles, dysfunction of this gland can have serious effects on the health and wellbeing of an animal. Three conditions most commonly seen are goiter, hypothyroidism, and hyperthyroidism.
Goiter manifests itself as a nonneoplastic (noncancerous), noninflammatory enlargement of the thyroid gland. It usually results from an iodine-deficient diet. Because iodine is an important component of thyroid hormone, a deficiency of iodine results in a deficiency of thyroid hormone. The anterior pituitary aottempts t compensate for this by producing more thyroidstimulating hormone (TSH). The elevated TSH levels overstimulate the thyroid and cause hyperplasia (cverdcvrlohmont) of the ghliasnd. T causes it to enlarge, resulting in what we call goiter. Alieiough goiter can be treated with iodine supplementation, it is more easiIy prevented than treated. In areas known to be iodine deficient, iodized salt should be added to animals' diets.
Hypothyroidism results from a deficiency of thyroid hormone. It is most commonIy seen in dogs, although it can be seen in any sepcaeucisees. B thyroid hormone influences the functioning of all cells, organs, and systems, hypothyroidism affects the whole ebhsiousdltys. T r in clinical signs that are vague and nonspecific. eTlhateey r primarily to a slowing of the body's metabolism. Common clinical signs include alopecia, or ⅛^ loss (usually
Hlateeally symmetric), dry skin, lethargy, reluctance to exercise, and weight gain without any increase in appetite. Affected animals often seek out sources of heat, because deficient thyroid hormone laeuvseels c the animal to have difficulty maintaining its body temperature. Most cases of hypothyroidism occur in middle-aged animals, but if it occurs in a young animal, dwarfism (impaired gnrdowth) a impaired mental development occur along with the other cnmmon signs. Hypothyroidism often can be treated effec- tydimveilnyibstearing thyroid hormone supplements to affected
ahnesime als. T supplements are usually in the form of the prohormone T4, yr AiyrcMne. The body then converts the T4 to ⅛e active hormone T3 as needed. Thyroid supplements usually have teoontbin uced for the rest of the animal's life.
Hyperthyroidism is the opposite problem. It results from tyuorcohidm th hormone production. It is most commonly
seen in cats, although it is seen occasionally in dogs. Excessive famounts o thyroid hormone speed up cellular metabolism all ovdeyr. the b This results in signs such as nervousness, excitability, weight loss, increased appetite, tachycardia (abnormally fast heart rate), vomiting, diarrhea, polyuria (excessive urine pirod^ιn∣, and polydipsia (excessive thirst). Hyperthyroidism is usually treated either by surgical removal of the thneoid gland (thyroidectomy) orby long-term administration yorfoaidt-hinhibiting drug.
∕j clinical application
Hypocalcemia
yTphoechalcemia-preventing action of parathyroid hormone cmaent ismo es be overwhelmed by the loss of calcium in the
fcmtailtkinog la animals. The hypocalcemia that results can rbieouass,e potentially life-threatening condition. The most loibnviciaolus c signs relate to disturbances in skeletal muscle function caused by the lack of calcium. In cattle this condition ie called milk fever, and it resuIts in generalized muscle nweakness. I mild cases, tremors and weakness are seen. As the ecoconmdietison b more severe, the animal may lie down and lboee unab t rise. Such an affected animal is often referred to as a downer cow. In dogs and cats, the condition is called eclampsia; it can cause muscle tremors and spasms that can oprogress t full-blown seizures if left untreated. Treatment in both cases is aimed at rapidly increasing the level of calcium in the blood by infusing a calcium solution intravenously.
TEST YOURSELF 11-4
1. What hormone plays an important role in helping an animal maintain its body temperature under cold environmental conditions? How does it produce its effects?
2. How do the clinical signs of hypothyroidism and hyperthyroidism relate to the normal functions of thyroid hormone?
3. What two hormones play important roles in maintaining homeostasis of blood calcium levels in the body? Which one prevents hypercalcemia? Which prevents hypocalcemia?
THE PARATHYROID GLANDS
CHARACTERISTICS
The parathyroid glands got their name because of their physical relationship with the thyroid gland. They are several small, pale nodules in, on, or near the thyroid glands. Figure 11-8 shows a parathyroid gland on the surface of an animal's thyroid gland. The precise location and appearance of the parathyroid glands vary quite a bit from animal to animal and species to species.
PARATHYROID HORMONE
Parathyroid hormone (PTH) is also conveniently called parathormone. It helps maintain blood calcium homeostasis by exerting an effect opposite to calcitonin. PTH helps prevent hypocalcemia, a blood calcium level that is too low, by increasing the blood calcium level if it should fall. It does this through its effects on the kidneys, the intestine, and the bones. It causes the kidneys to retain calcium and the intestine to absorb calcium from food, and it withdraws calcium from the calcium bank (the bones).

FIGURE 11-8 Identification of the thyroid and parathyroid glands during surgery. The animal's head is to the right. The forceps are grasping the cranial end of the thyroid gland. The parathyroid gland is the oval structure just adjacent to the end of the ruler and measuring approximately 4 to 5 mm. (From Little S: The cat, Philadelphia, 2012, WB Saunders Company.)
THE ADRENAL GLANDS
CHARACTERISTICS
The adrenal glands are named for their proximity to the kidneys (renal refers to kidneys). The two adrenal glands are located near the cranial ends of the kidneys. (Note their locations in Figure 11-9.) Like the pituitary gland, the adrenals appear to be single structures, but they are actually two glands. In this case, one gland is wrapped around the other like chocolate wrapped around a peanut (Figure 11-10). The two glands, the outer adrenal cortex and the inner adrenal medulla, come from different embryologic origins and have different structures and functions.
ADRENAL CORTEX
The adrenal cortex, the outer gland, develops from glandular tissue and looks like normal endocrine tissue microscopically. Under the direction of ACTH from the anterior pituitary gland and other mechanisms, the adrenal cortex produces an assortment of hormones that are classified into
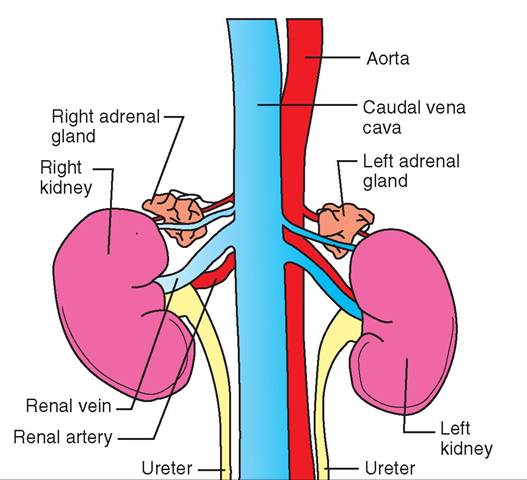
FIGURE 1 1 -9 Adrenal glands of the dog. Ventral view.
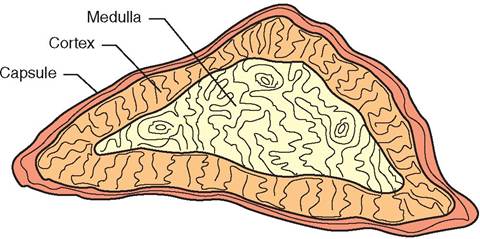
FIGURE 11-10 Adrenal gland. Cross section showing cortex and medulla.
three ran groups: glucocorticoid hormones, mineralocorticoid hormones, and sex hormones. All aee referred to as steroids because their chemical structure is based on cholesterol.
GLUCOCORTICOID HORMONES. The name for the group of glucocorticoid hormones comes from its effect on the blood glucose levels. These hormones—cortisol, cortisone, and corticosterone among them—have a general hyperglycemic effect; that is, they cause the blood glucose ievel to me. Several mechanisms are involved, including the breakdown (catabolism) of proteins and lipids. Most of the breakdown products are ultimately converted to glucose in the liver through a process called gluconeogenesis. Other lfeuffceocctos roticgoids include helping to maintain blood
pressure and helping the body resist the effects of stress.
MINERALOCORTICOID HORMONES. Mineralocorticoid hormonesergulate the levels of some important electrolytes (mineral salts) in the body. The principal mineralocorticoid hormone, aldosterone,ecatfsf the levels of sodium, potassium, and hydrogen ions in the body. Its target iys, the kidne where it causes sodium ions to be reabsorbed from the urine back into the bloodstream in exchange for potassium and hydrogen ions, which pass out of the body in ithnhee. ur T level of sodium in the body must be maintained at a fairly high level normally, but much less potas- siumis needed. Potassium actually can be toxic if it accumulates to a level that is too high. Some drug preparations used to euthanize animals contain very high levels of potassium, which stops the beating of the heart. Hydrogen ions affect the body's acid-base balance, which must be
∕j CLINICAL APPLICATION
Glucocorticoid-Related Diseases
A condition that results from too much glucocorticoid hormone being produced by the adrenal cortex is hyperadre- nocorticism, sonmU'mes called Cushing’s disease. Iititial clinical sign s include polyuria (excess urine production), polydipsia Iixciss water consumption), and polyphagia (increased appetite). Long-term signs include hair loss, muscle wasting, and slow wound healing. The signs of naturally occurring hyper- adrenocorticism can be mimicked by administration of high fodrotsiecsosote rcoid drugs.
Hypoadrenocorticism (sometimes called Addison’s disease) is a condition caused by a deficiency of adrenocortical hormones. Clinical signs are somewhat nonspecific, including weakness, lethargy, vomiting, and diarrhea. It is usually a progressive condition that can lead to circulatory problems and kuirden. ey fail The effects of the disease can be mimicked if long-term corticosteroid drug administration is suddenly stopped.
CLINICAL APPLICATION
Glucocorticoid-Related Drugs
Drugs modeled after glucocorticoid hormones are commonly uhseeradpetutically in animals, usually for their anti
inflammatory effect. This general class of drugs is commonly known corticosteroids or glucocorticosteroids mid includes sudrcuhgs s a hydrocortisone, prednisone, dexamethasone, and triamcinolone. Because they mimic many of the effects of natural glucocorticoid hormones and are given in amounts amrguecrh l than the natural hormones, these powerful drugs have many potential side effects. These include the following:
• Suppression of the immune response. Tlris can lwer an ani- mafs defenses and make it more susceptible to infection.
• White blood cell count alteration. Au a resuIt of corticoste-
rduogmidindisrtrataion, neutrophil numbers go up, and
lymphocyte, eosinophil, and monocyte numbers go down. This mimics the body's natural stress response. If we're ooing to administer corticosteroid drugs to an animal around the time that blood is to be drawn for a complete blood count (CBC), the blood should be drawn before the idvreung. is g This approach avoids confusion in interpret- iensuglths.e r
• Slowing of wound healing. Scar prone-producing fibroblast ecells ar inhibited.
• Catabolic effect. After long-term corticosteroid drug use, the catabolism (breakdown) of protein can result in tfhinning o the skin, loss of hair, and a general loss of muscle mass.
• Premature parturition. Admmittrution of corticosteroid rodergungasntt p animals can cause abortion of fetuses.
• Hyperglycemia. This condition can be significant in an iatnhimal w diabetes mellitus, because it can change the animal's insulin requirement.
• Suppression of adrenal cortex stimulation. Tlye body’s normal eeedback mechanisms interpret the high levels of corti coste- ruid drug in the bloodstream as high levels of glucocorticoid hormones. This causes a cascade effect from the hypothalamus tThat's how long it has taken your body to corral all your fight-or-flight hormones.
THE PANCREATIC ISLETS
nTdhoecreine portion of the pancreas is organized into fthousands o tiny clumps of cells scattered throughout the ohregsean. T clumps of cells are called pancreatic islets,r o islets of Langerhans. Themain endocrine cells of the pancreatic isles are alpha cells, which produce the hormone glucagon; beta cells, wHi^le produce insulin; and delta cells, which pmraotdoustcaetisno.
PANCREATIC HORMONES
fTwo o the three hormones produced by the pancreatic islets, insulin and glucagon, play important roles in controlling the metabolism and use of glucose, and they have opposite ehfefects. T third hormone, somatostatin, inhibits the secretion of insulin and glucagon, as well as GH, and diminishes tchtieviaty of the gastrointestinal tract.
CLINICAL APPLICATION
Diabetes Mellitus
Without sufficient insulin in the body, glucose does not move into body cells. It builds up in the blood, resulting in excessively high blood glucose levels (hyperglycemia), which spill ∞^ into the urine, thereby producing glycosuria, or glucose in the urine. At the same time, the body's cells are starved of energy, because they cannot absorb and use the glucose that surrounds them.
Diabetes mellitus is a disease caused by a deficiency of the hormone insulin. The clinical signs of diabetes mellitus usually develop gradually. They include polyuria, polydipsia, polyphagia, weight loss, and weakness. Laboratory tests reveal hem^^^^^mia (too high a level of glucose in the blood) and glycosuria. The condition can be fatal if left untreated.
Diabetes mellitus is not presently curable, but it often can be contedlled effectively through appropriate treatment. This approach usually involves careful management of the ani- tmal's die and amount of exercise, administration of insulin injections once or twice a day, and frequent monitoring of tshe animal' urine and blood glucose levels. The dose of insulin mu st be carefully controlled, because an overdose can result in hypoglycemia (too low o level of glucose in the bhliochod), w can lead to weakness and collapse.
/ TEST YOURSELF 11-5
1. What three groupsof hormonesare produced in the adrenal coutcx? What auc thciu effects?
2. How oretSnS ormoc ea ofthe adrenaI meθulla involved in the fight-or-flight response?
THE PANCREAS
The pancreas is a long, flat, abdominal organ located near the duodenumso(trtthieo nfir p of the small intestine) that has bnfiι exocrine and endocrine functions. Most of its mass ifdsema up o exocrine glandular tissue that produces impor- teasntitvedig enzymes. Its endocrine component makes up lonly a smal percentage of the total volume of the organ, but fone o its hormones, insulin, is vital to the life of an animal.
INSULIN. The hormone insulin is essential for life. It lcuacuossees, g amino acids, and fatty acids in the blood- seotream t b absorbed through cell membranes into body cdells and use for energy. Because its overall effect on glucose ivose t mo it out of the bloodstream and into cells, insulin aowcetrs t lo the level of glucose in the blood.
GLUCAGON. Glucagon has an effect opposite to insulin. Iwnesruslin lo the blood glucose level, whereas glucagon rhaisises it. T hyperglycemic effect is accomplished by two mainmechanisms: glucagon stimulates liver cells to convert glycogen (a storage form of glucose) to glucose. It also stimulates gluconeogenesis (the conversion of fat and protein breakdown products to glucose). The net effect of both is to raise the level of glucose in the blood. Because other hormones, such as GH (from the anterior pituitary gland) and glucocorticoid hormones (from the adrenal cortex), have similar hyperglycemic effects, a deficiency of glucagon is not as devastating to the body as a deficiency of insulin.
THE GONADS
The gonads are the reproductive organs—the testes in the male and the ovaries in the female. They produce the male and female reproductive cells and important hormones.
THE TESTES
The two testes are housed in the scrotum, a sac of skin in the inguinal region. The majority of each testis is made up of coiled seminiferous tubules, where spermatozoa are produced. Scattered between the seminiferous tubules are clumps of endocrine cells, called the interstitial cells (Figure 11-11), which produce androgens, the male sex hormones. The production of androgens by the interstitial cells is stimulated by the anterior pituitary hormone luteinizing hormone (LH), also known as interstitial cell stimulating hormone (ICSH) in the male. The principal androgen that the interstitial cells produce is testosterone. It is responsible for the development of male secondary sex characteristics, such as the muscular male body shape and the male libido, or sex drive. Testosterone also stimulates the development of
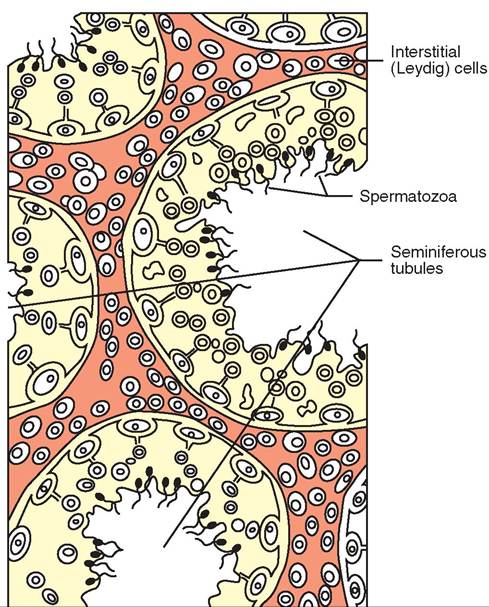
FIGURE 11-11 Interstitial cells of testes. Interstitial cells of testes produce androgens, principally testosterone, under stimulation by luteinizing hormone from the anterior pituitary.
the male accessory sex glands, activates spermatogenesis (spermatozoa production), and stimulates the growth of the penis. Testosterone is a steroid hormone with an overall anabolic effect in that it stimulates the buildup of proteins in muscle and bone.
THE OVARIES
The two ovaries are located in the abdomen up near the kidneys. Unlike the testes, which produce spermatozoa and hormones continuously, the ovaries produce the female reproductive cells (ova) and hormones in cycles. The ovarian cycles are controlled by two anterior pituitary hormones: follicle stimulating hormone (FSH) and luteinizing hormone (LH). The main hormone groups produced in the ovaries are estrogens and progestins. A third hormone, relaxin, may be produced in the ovary late in pregnancy.
ESTROGENS. Estrogens, such as estradiol and estrone, are the female sex hormones. They are produced when FSH from the anterior pituitary gland stimulates follicles to develop in the ovaries. Follicles are fluid-filled structures in which the female reproductive cells develop. The cells that make up the follicles produce and release the estrogens into the bloodstream. Estrogens are responsible for the physical and behavioral changes that prepare the female for breeding and pregnancy and signal the male that the time for breeding is approaching.
As an ovarian follicle grows, the amount of estrogens it produces grows as well. The increasing estrogen levels accelerate the physical and behavioral changes that are occurring and feed back to the anterior pituitary gland. The feedback causes the anterior pituitary gland to reduce the production of FSH and increase the production of LH. As the follicle continues to grow, the amount of FSH in the bloodstream gradually decreases and the LH level increases. When the follicle is fully mature, the LH level peaks and, in most animal species, ovulation occurs. Ovulation is the rupture of the blisterlike follicle with release of the ovum into the oviduct. (See Chapter 19 for a more complete description of the whole process of follicle development and rupture.)
PROGESTINS. After ovulation has taken place, the high LH level stimulates the cells of the now-empty follicle to multiply and develop into a solid, hormone-producing structure—the corpus luteum. The term literally means yellow body and derives from its pale yellow color. The corpus luteum produces several hormones that are collectively called progestins. The principal progestin is progesterone, whose name means pregnancy-promoting steroid hormone. Progesterone helps prepare the uterus to receive the fertilized ovum and is necessary for pregnancy to be maintained once the fertilized ovum implants in the uterus.
If the female animal is bred and becomes pregnant, the corpus luteum must continue to be active in the ovary, producing the pregnancy-supporting progestin hormones. Different species have different ways to do this, but the basic mechanism is that a substance produced by the early embryo feeds back to the uterus and ovary, and causes the corpus luteum to be maintained. If pregnancy does not occur, no “we are pregnant” signal is received, and the corpus luteum shrinks up and disappears.
Progestin-related drugs are often used therapeutically, especially in horses. They are most commonly used to delay the onset of estrus (the heat period), to synchronize the ertrous periods in a group of mares so that they can be bred at the same time, and to help maintain pregnancy in mares that have deficient natural progesterone levels.
RELAXIN. Late in pregnancy, the hormone relaxin causes leitgwaemeennts b the bones surrounding the birth canal to soften and relax in preparation for parturition (the birth process). It may also play a role in mammary development in some species. Depending on the species, relaxin may be yproduced b the corpus luteum, the placenta or the uterus.
TEST YOURSELF 11-6
∕j CLINICAL APPLICATION—cont'd
(glucocorticoid-like drugs) or stimulation of uterine contractions (onytocin), cardiovascular stimulation (epinephrine), or to s∖∙'nchfonize estrous cycles (prostaglandin F2α).
Because the production and effects of natural hormones earreelsaoteidn,t the therapeutic use of hormones and
hormonelike drugs can produce some potent and wide- sropbreleamd sp, along with beneficial effects. The amounts
of hormones used therapeutically are usually very large com- iptahred w the normal physiologic hormone levels in the rbeofdoyr,e the the potential for undesired side effects increases accordingly. For example, use of a hormonelike drug can inhibit production of the natural hormone it mimics. Later, when the drug is to be discontinued, the animal should be gradually weaned off it so that the natural hormone production mechanisms can gradually take over again. Suddenly stopping the drug after long-term administration can produce disastrous results. In general, hormone therapy must be carefully planned and closely monitored so that the benefits outweigh the consequences.
1. Vhhich four Iiormoneshavehyperglycemiceffects in the body? Whot ir ths holy horyoou that octr th lower ths blhhd glucoru luvul?
2. Which hm rmoneαreαnodolicgte roiO Uru go related to? d. How Oot ho boorc acii onsand pnrposeh mfestrogens
ood eroguetioe differ?
4. Howdooerelaeineolu o feruroa fregnontaeimal for eorturitioo?
CLINICAL APPLICATION
Anabolic Steroid Drugs
Anabolic steroid drugs, which are related to testosterone, are used to help debilitated animals regain strength and weight after surgery or long illnesses. Unfortunately, they are sometimes abused by people seeking a shortcut to muscular development and performance enhancement. Because of their soimilarity t the hormone testosterone, they have many undesirable side effects that alter reproductive functions, behavior, and other body systems.
CLINICAL APPLICATION
Hormones as Drugs
Because of their powerful and often widespread effects, hor- nmdones a hormonelike substances are used as drugs to treat irollnesses o t produce particular desired effects in animals. When natural hormone levels are too low, hormones can be given thecapeutically to help correct the imbalance. This is often the case with hypothyroidism (deficiency of thyroid hormone), diabetes insipidus (deficiency of antidiuretic hormone), and diabetes mellitus (deficiency of insulin). In aostehse,r c drugs derived from natural hormones are used to produce particular effects, such as an anti-inflammatory effect
OTHER ENDOCRINE ORGANS
Hormone production is not restricted to the major endocrine glands that we have just discussed. Other organs and tissues produce hormones that also play important roles in maintaining homeostasis in the body. We discuss some of the most important and well-understood ones next.
THE KIDNEYS
In addition to their blood-filtering duties, the kidneys produce the hormone erythropoietini whlchstimulates red bone marrow to increase production of oxygen-carrying lreoelldos.db c The production of erythropoietin is stimu- lyated b a decrease in the oxygen content of the blood, a condition called hypoxia. As the production of red blood ecealsless incr in response to the erythropoietin, the ixnycgreenased o level in the blood feeds back to the kidneys and slows the production of erythropoietin. This helps maintain the long-term homeostasis of the blood's oxygen-carrying ability.
fOne o the conditions that often accompanies serious kidney disease or kidney failure is anemia, which is a defi- fceidency o r blood cells. It results from the damaged kidneys' inability to produce enough erythropoietin. The fdeficiency o erythropoietin causes the patient to become increasingly hypoxic, because old, worn-out red blood cells coontinue t be removed from the bloodstream but not ewnough ne red blood cells are being produced to replace them. Blood transfusions are often necessary to support iptahtients w kidney failure while other forms of therapy are administered. Synthetic forms of erythropoietin are available and are often used therapeutically in human iptahtients w kidney failure. Their high cost limits their use ientevrinary medicine.
THE STOMACH
Cells in the wall of the stomach produce the hormone gastrin. It is a somewhat oddball hormone, because it is produced in the stomach wall and acts on the stomach wall, too. Its secretion is stimulated by the presence of food in the stomach. When released, gastrin stimulates gastric (stomach) glands to secrete hydrochloric acid and digestive enzymes, and it encourages muscular contractions of the stomach wall.
THE SMALL INTESTINE
Cells in the lining of the small intestine produce two hormones when partially digested material from the stomach (chyme) enters the first portion of the small intestine (the duodenum). One of the hormones, secretin, stimulates the pancreas to secrete fluid rich in sodium bicarbonate into the duodenum to neutralize the acidic chyme from the stomach. The other hormone, cholecystokinin, stimulates the release of digestive enzymes from the pancreas into the duodenum. Both secretin and cholecystokinin also act on the stomach to inhibit gastric gland secretions and stomach motility. This slows the movement of chyme into the small intestine. They also stimulate the gallbladder of the liver to contract, sending bile down into the small intestine to aid the digestion and absorption of fats and fat-soluble vitamins.
THE PLACENTA
The placenta is the life support system that surrounds a developing fetus during pregnancy and acts as an interface with the maternal circulation. It is also an important endocrine organ. Its secretions vary among species, but the hormones it produces have the general effect of helping to support and maintain pregnancy. Small amounts of estrogen and progesterone are often produced, as well as significant amounts of chorionic gonadotropin in some species, most notably the human and the horse. Detection of chorionic gonadotropin is the basis of over-the-counter pregnancy tests for humans and blood tests for the detection of pregnancy in horses. Other species, such as dogs, cats, and cattle, produce too little chorionic gonadotropin to make it useful as a method of pregnancy diagnosis.
The placenta of some species produces the hormone relaxin late in pregnancy. It helps relax ligaments between the bones around the birth canal in preparation for parturition. Depending on the species it may be produced by the placenta, the uterus, or the corpus luteum of the ovary.
THE THYMUS
The thymus is an organ that helps kick start the immune system early in an animal's life. It shrinks down and nearly disappears when the animal reaches adulthood. In a young animal, the thymus is fairly large. It extends cranially from the level of the heart in the thorax up into the neck region along both sides of the trachea, often to the level of the larynx. After puberty, however, the thymus begins to atrophy (shrink). By the time the animal reaches adulthood, it is hard or impossible to find any remnant of the thymus.
The thymus is an important part of the animal's developing immune system—the system that helps fight off foreign invaders, such as disease-causing bacteria and viruses. Part of its functioning seems to involve hormones or hormone- like chemical substances, such as thymosin and thymopoietin. These substances seem to cause primitive cells in the thymus and other lymphoid organs to be transformed into T (for “thymus-derived”) lymphocytes. T lymphocytes are often just called T cells. They are an important part of the animal's cell-mediated immunity—the portion of the immune system that produces “killer cells” that directly attack foreign invaders (see Chapter 13).
THE PINEAL BODY
The pineal body is a part of the brain located at the caudal end of the deep cleft that separates the two cerebral hemispheres, and just rostral to the cerebellum. Its functions are not well understood yet, but it is known to influence cyclic activities in the body, or the body's biologic clock. It produces a hormonelike substance called melatonin that seems to affect moods and wake-sleep cycles. It may also play a role in the timing of seasonal estrous cycles in some species. We still have a lot to learn about the roles of the pineal body and its secretions.
PROSTAGLANDINS
Prostaglandins are hormonelike substances that are derived from unsaturated fatty acids. They are produced and exert their effects within a variety of body tissues. Because they only travel a short distance from where they are produced, prostaglandins are sometimes called tissue hormones. Typical hormones regulate the activities of tissues and organs at some distance from where they are produced. Prostaglandins do not go very far from home. They regulate the activities of neighboring cells.
The name prostaglandin actually came about by mistake. The first prostaglandin was isolated from semen, and its origin was incorrectly identified as the prostate gland, hence the name prostaglandin. We now know that the seminal vesicles, not the prostate, produce that particular compound. (Vesicular-glandins apparently isn't as catchy a name as prostaglandins!)
Prostaglandins are now known to be produced in a variety of body tissues, including the skin, intestine, brain, kidney, lungs, reproductive organs, and eyes. Based on their molecular structure, they are organized into nine main groups— prostaglandins A through I. Subscript numbers and Greek letters are added to designate subgroups.
Prostaglandins exert some powerful effects in the body, including influences on blood pressure, gastrointestinal tract function, respiratory function, kidney function, blood clotting, inflammation, and reproductive functions. The E group of prostaglandins (PGEs) is known to play a role in the initiation of inflammation in the body. Nonsteroidal anti-inflammatory drugs, such as meloxicam (Metacam), carprofen (Rimadyl) and ibuprofen, produce some of their effects by inhibiting PGE synthesis.
Another clinically important prostaglandin is prostaglandin F2alpha (PGF2alpha). Iif administered to a female animal that has a functional corpus luteum in her ovary, PGF2alpha will quickly destroy the corpus luteum. This is called luteoly- sis, and, depending on the species, it may cause a new estrous ceoygcinle. t b If the animal is in early pregnancy, luteolysis will tnm^^te the pregnancy. Drugs with PGF2alpha activity, such as dinoprost tromethamine (Lutalyse), are commonly ured to synchronize estrous cycles in livestock species so that fgroups o animals can be bred at the same time.
Note: Bacaiise of their potentially harmful reproductive frafnedctsothe e in humans, it is recommended that PGF2- alpha drugs be handled with caution; they should not be handled at all by pregnant women.
TEST YOURSELF 11-7
1. Why are patientswithkidney Iailureoften anemic?
2. How do the hctioes af eastrin ynthe stomach differ from rhoea oh eadratia oat dhyiadyetokiaia?
3i Why are proatsgle adias referroe to as tissue hormones?
4. Why ola hormodelike taros gererally have a high poraarioi hor daSaeirobia eida ahhacte?