Esophagus
Normal
The esophagus is designed for the passage of macerated food and liquid into the stomach for further digestion. The luminal surface is therefore lined with a layer of stratified squamous epithelial cells, which protect the esophagus from damage (Figures 7.5a,b).
Epithelial cells are not keratinized throughout the majority of the esophagus and are usually round in shape with a single nucleus and low nuclear to cytoplasmic (N:C) ratio (Figure 7.6). The esophageal submucosa contains mucous glands to aid lubrication. The muscularis layer is thick and contains skeletal muscle (except very near the stomach) (Bacha & Bacha, 2012). 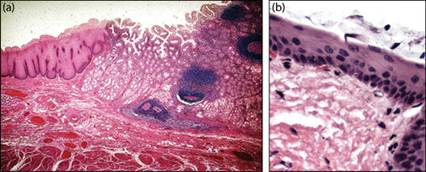
Figures 7.5a,b Histologic sections of the esophagus, canine. (a) Low-power (40x) magnification showing the gastroesophageal junction and the transition from stratified squamous epithelial mucosa to the glandular mucosa of the stomach. (b) Magnification of the esophageal mucosa showing the nonkeratinized squamous mucosal layer (H&E, 500? magnification).
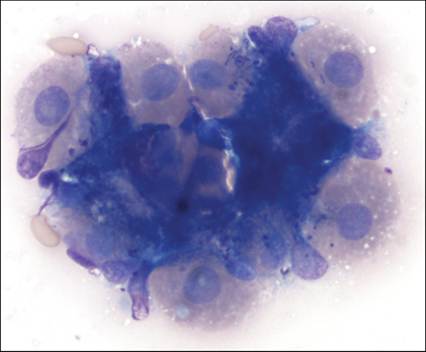
Figure 7.6 Cytology of normal esophageal squamous epithelial cells with overlying debris. These cells were obtained during endoscopic examination of the upper intestine and found adjacent to normal duodenal epithelium (see Figure 7.16a). The round shape with a single nucleus and eosinophilic cytoplasm gives these cells a ‘fried egg’ appearance typical for intermediate squamous epithelial cells (Wright–Giemsa, 500? magnification).
Hyperplastic lesions
In hyperplastic lesions of the GIT, diagnosis is usually presumptively based on diagnostic imaging and the identification of uniform populations of epithelial cells. In the esophagus, squamous hyperplasia has been described with disorders such as chronic regurgitation and reflux gastroesophagitis.
This may rarely result in a condition referred to as ‘Barrett’s esophagus’ where chronic inflammation induces intestinal metaplasia and development of columnar epithelium in the esophagus. Full characterization of this disorder is reliant on endoscopic imaging and biopsy (Sellon & Willard, 2003).Inflammatory lesions
As animals frequently ingest coarse materials, damage to the esophagus occasionally occurs and can result in signs of dysphagia, coughing, retching, hemoptysis, repeated swallowing, and occasionally ptyalism. In more chronic lesions, such as those caused by foreign bodies or esophageal parasites, anorexia and weight loss may be evident (Sellon & Willard, 2003). Inflammation is variable depending on the underlying disease. Esophageal infections may occur and are usually secondary to trauma. It is important to recognize the presence of normal oropharyngeal flora when interpreting the presence of bacteria in an upper GIT sample (Figure 7.7).
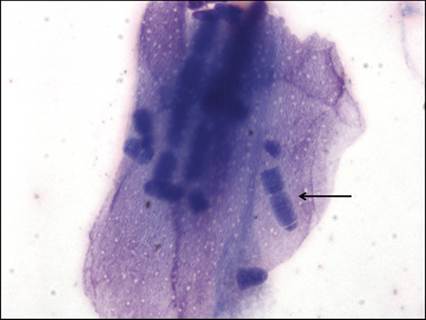
Figure 7.7 Mixed bacteria consistent with oral flora. Note the presence of large bacterial rods consistent with Conchiformibius (previously Simonsiella) spp. overlying a squamous epithelial cell (arrow) (Wright–Giemsa, 1,000? magnification).
There are few infectious organisms that localize to the esophagus. The esophageal worm Spirocerca lupi is a nematode found in tropical and subtropical regions including the southeastern region of the United States. Infection follows ingestion of an intermediate host (coprophagous beetle). Larvae follow a specific migratory route, penetrating the gastric mucosa of the host, migrating along arteries, maturing in the thoracic aorta before eventually moving to the caudal esophagus. In the esophagus, the worm develops in large nodules (Figures 7.8a, b) and passes larvated eggs in feces that can be detected using zinc sulfate fecal flotation. Chronic lesions have been associated with the development of sarcomas in up to 25% of infected dogs (Porras-Silesky et al., 2021).
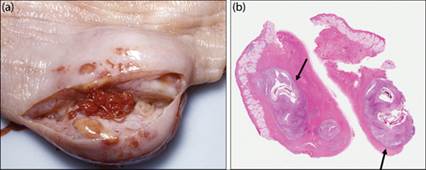
Figures 7.8a,b (a) Gross image of Spirocerca lupi infection in a dog. In the caudal esophagus, the worm develops in nodules and passes larvated eggs in feces, which can be detected via fecal flotation. (b) Histologic image of Spirocerca infection in the same dog. Note the marked inflammatory infiltrate surrounding the larva (cross-section) (arrows) (H&E, 20? magnification) (courtesy Roger J. Panciera).
Neoplastic lesions of the GIT are typically associated with clinical signs based on their localization. In the esophagus, masses may result in dysphagia, ptyalism, regurgitation, anorexia, and progressive weight loss.
Neoplasms of the esophagus
Epithelial tumors
Benign epithelial tumors of the alimentary tract are generally uncommon in small animals (Willard, 2012; Munday et al., 2017). Few cases of primary esophageal carcinomas, most commonly squamous cell carcinoma (SCC), have been described in dogs and cats (Munday et al., 2017). Prognosis in these lesions is guarded due to the difficulty in adequate removal and the metastatic tendency (Willard, 2012). Locally invasive tumors such as thyroid carcinomas or oral SCCs may invade into the esophagus. These are identified based on their similarity to cytologic appearance in other sites.
Stromal/spindle cell tumors
Stromal tumors of the esophagus are infrequently reported in dogs. Smooth muscle tumors, leiomyomas, and leiomyosarcomas have been reported in the esophagus (Frost et al., 2003). These are usually nodular masses situated at the gastroesophageal junction in older animals (Munday et al., 2017). Sarcomas, including fibrosarcomas and osteosarcomas, can develop secondary to infection with Spirocerca lupi (Porras-Silesky et al., 2021).