Hematopoietic abnormalities
Erythroid hyperplasia
Erythroid hyperplasia (Figure 19.17) results from up-regulated erythropoiesis and is characterized by normal or increased marrow cellularity with a relative or absolute increase in erythroid cells, reduced G:E, and increased reticulocyte concentration in peripheral blood.
It is most commonly a response to increased demand for erythrocytes, such as in immune- or toxin-mediated hemolytic anemia, blood loss, or chronic hypoxia. An increase in blood reticulocytes occurred within 48 hours and lasted 12–14 days in humans given a single injection of erythropoietin (Perez-Ruixo et al., 2008). Similarly, in rats one erythropoietin injection caused an increase in early rubricytes by 24 hours, late rubricytes at 72 hours, and peripheral blood reticulocytosis at 72–96 hours (Xu et al., 2022). These time frames correspond to those observed in dogs and cats where marrow erythroid hyperplasia is not evident until at least 48 hours after onset of anemia due to hemorrhage. The magnitude and timing of the erythropoietic response to anemia depend on the body condition of the animal, the abundance of iron and other nutrients, the severity and rapidity of onset of anemia, whether blood loss is external or internal, and the presence of concurrent illness. Regenerative anemias, such those typically associated with immune-mediated hemolytic anemia (IMHA) or blood loss in young animals, are not indications for marrow evaluation since there is usually evidence of an appropriate response on the CBC. The cause of anemia in such cases can be diagnosed from a thorough history, blood smear evaluation (e.g. spherocytes), or imaging (e.g. splenic hemangiosarcoma).id=fig19.17.jpg class="lazyload" data-src="/files/uch_group75/uch_pgroup311/uch_uch7426/image/image1070.jpg" alt=fig19.17.jpg>
Figure 19.17 Erythrocytic hyperplasia in a dog with blood loss anemia, 400? magnification.
Erythropoiesis may be hyperplastic but nevertheless ineffective, as indicated by lack of blood reticulocytosis and persistence of anemia. Hyperplastic but ineffective erythropoiesis may occur with severe iron deficiency, immune destruction of rubricytes, myelodysplasia, cobalamin deficiency, and other conditions (Lutz et al., 2013). Erythroid hyperplasia may also be accompanied by ‘incomplete maturation’ where there is an abundance of early and late rubricytes, and there may be metarubricytes, but a paucity of reticulocytes (Figure 19.18).
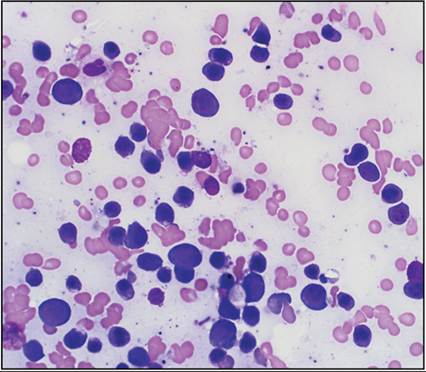
Figure 19.18 Erythrocytic hyperplasia with incomplete maturation in a dog, 400? magnification. There is a relative paucity of polychromatic cells despite a large number of rubricytes.
Erythroid atrophy
Erythroid atrophy is characterized by normal to decreased marrow cellularity with a relative or absolute reduction in erythroid cells. As a result, in most cases the G:E is increased, and if animals have erythroid atrophy concurrent with inflammation and granulocytic hyperplasia, the G:E cell ratio may be extremely high (Figure 19.19). Causes of erythroid atrophy include chronic kidney disease, other chronic illness, systemic viral infection, erythroid precursor cell injury, myelodysplasia, myeloid neoplasia (Figure 19.20), and in rare cases antibodies to erythropoietin, usually subsequent to treatment with recombinant erythropoietin. Erythroid atrophy results in non-regenerative or poorly regenerative anemia.
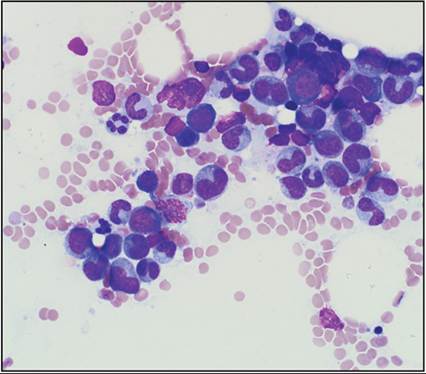
Figure 19.19 Granulocytic hyperplasia and erythrocytic atrophy in a dog with chronic inflammation, 400? magnification.
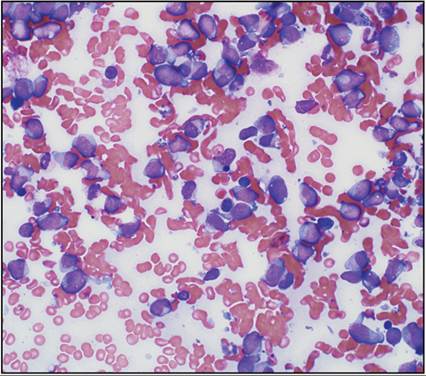
Figure 19.20 Marrow smear from a dog with acute myeloid leukemia (WBC 185 ? 109/L, 400? magnification.
There is lack of maturation to band and segmented neutrophils, and a paucity of rubricytes.
Non-regenerative immune-mediated anemia (NRIMA) and precursor-targeted immune-mediated anemia (PIMA) are conditions with overlapping diagnostic features (Lucidi et al., 2021; Woolhead et al., 2021). An immune-mediated etiology is suggested by increased immunoglobulin or phosphatidylserine detection on marrow rubricytes, though validated diagnostic tests with high specificity to confirm this pathogenesis remain elusive. In dogs with severe non- or poorly regenerative anemia, a lack of peripheral blood spherocytosis and hemolysis, and increased frequency of rubricyte phagocytosis by marrow macrophages, NRIMA/PIMA should be suspected. Immune dysregulation secondary to thymoma has also been associated with erythroid atrophy and marrow pan-atrophy. These findings support immune mechanisms contributing to some cases of erythroid atrophy. Animals that recover from erythroid atrophy have a transient shift toward early rubricytes prior to re-establishment of orderly and complete maturation. Persistent erythroid atrophy and anemia in conjunction with dysplastic features in hematopoietic cells should prompt consideration of myelodysplastic syndrome (MDS).
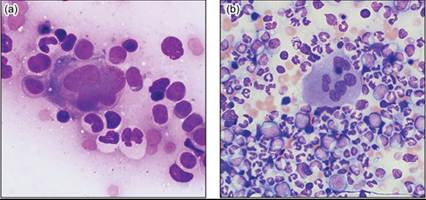
Immune-mediated cytopenia (IMC) in cats manifests with anemia and frequently also with neutropenia or thrombocytopenia. There may be erythrocyte and/or leukocyte and/or platelet agglutination on blood smears (Figure 19.21). Marrow findings are similarly diverse, and hyperplasia, atrophy, and dysplasia with or without myelofibrosis may all occur. Blood lymphocytes are often in the high normal range or increased, and frequently also increased in marrow from cats with IMC. While T-lymphocytes typically predominate, plasma cells and B-lymphocytes are also present (Figure 19.22).
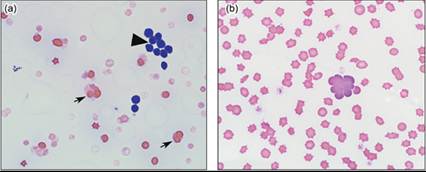
Figures 19.21a,b (a) Blood smear from a cat with anemia, neutropenia, and thrombocytopenia, 400? magnification.
There was leukoagglutination (arrowhead), erythrocyte agglutination (arrow), and marked hemolysis. (b) Blood smear from a cat with anemia and neutropenia showing agglutination of polychromatophilic cells, 600? magnification.
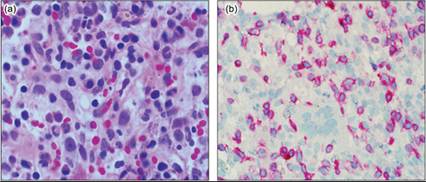
Figures 19.22a,b (a) The marrow core section from the cat with immune-mediated cytopenia in Figure 19.21a contains numerous small lymphocytes, plasma cells, and few metarubricytes, 600? magnification. (b) Immunohistochemical staining identifies lymphocytes as CD3 positive. Only rare CD79a positive lymphocytes were present (not shown), 600? magnification.
Some cats infected with feline leukemia virus (FeLV) subgroup C develop pure red cell aplasia (PRCA) characterized by profound, non-regenerative anemia with normal granulocyte and platelet concentrations. Marrow aspirates show a near complete absence of erythrocytic cells with normal granulopoiesis and megakaryopoiesis. FeLV-C binds to and impairs the function of the cell surface receptor FLVCR1, which is a heme exporter important in protecting erythroid progenitors against the toxic effects of heme (Khan & Quigley, 2013).
Dyserythropoiesis
Dyserythropoiesis is abnormal erythrocyte maturation and/or morphology. Examples include megaloblastic cells, rubricytes with abnormal nuclear shapes or multiple nuclei, premature pyknosis, and siderotic inclusions in rubricytes (Figure 19.23). Megaloblastic cells result from asynchronous DNA synthesis and cell growth yielding abnormally large cells with relatively small nuclei. Megaloblastic erythropoiesis gives rise to peripheral blood macrocytosis. In humans, megaloblastosis is most commonly due to cobalamin and/or folate deficiency from impaired absorption (chronic pancreatitis or malabsorptive disorders), dietary scarcity, lack of intrinsic factor, or a defective cubam transporter. Affected individuals typically have mild anemia and also neutrophil hypersegmentation.
Anemia and neutrophil hypersegmentation but not macrocytosis were reported in dogs with intestinal cobalamin malabsorption due mutations in the CUBN gene (Imerslund-Gräsbeck-like syndrome) (Lutz et al., 2013; Sancho et al., 2021). Similar changes do not appear to occur in dogs with hypocobalaminemia or hypofolatemia secondary to intestinal disease (Stanley et al., 2019). 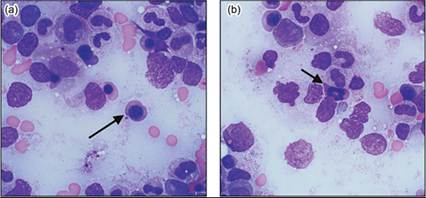
Figures 19.23a,b Marrow smear from a dog with anemia, 1,000? magnification. Rubricytes have dysplastic changes indicated by cells with fully hemoglobinized cytoplasm but large immature nuclei (a, arrow) and mitotic metarubricytes (b, arrow).
Megaloblastic erythropoiesis is a feature of some FeLV infections, and typically manifests with macrocytosis, anemia, and other cytopenias. Macrocytosis precedes anemia, and is considered a harbinger of FeLV-associated myelodysplastic syndrome (MDS) (Hisasue et al., 2009).
Peripheral blood macrocytosis and megaloblastic change in marrow occurs in some toy and miniature poodles (Canfield & Watson, 1989). Marrow abnormalities are confined to erythroid cells and include megaloblastosis, multinucleation, abnormal mitoses, occasional sideroblasts, and multiple and abnormally shaped Howell-Jolly bodies. Dogs are usually not anemic, and the condition is not associated with cobalamin or folate deficiency (Boyd & Best, 2018).
Granulocytic hyperplasia
Granulocytic hyperplasia results from increased granulopoiesis and is characterized by normal or increased marrow cellularity and an increased G:E. Granulocytic hyperplasia may be effective resulting in granulocytosis, or ineffective with granulocytopenia despite marrow hyperplasia.
Neutrophil hyperplasia
Effective marrow neutrophil hyperplasia results from a persistently increased peripheral demand for neutrophils due to inflammation in conditions such as infection, sepsis, tissue necrosis, immune-mediated disease, and malignancy.
Cytokines produced during inflammation increase neutropoiesis. Marrow neutrophils may have toxic changes in severe inflammatory disease or during recovery from marrow injury. Such changes reflect accelerated maturation with disturbed organelle formation. When tissue demand exceeds marrow storage of segmented neutrophils, band neutrophils and progressively more immature granulocytes are released, which results in a left shift in marrow granulopoiesis. If an inflammatory cause for neutrophilia is apparent, marrow evaluation is not indicated.Ectopic production of granulocyte colony-stimulating factor (G-CSF) and/or granulocyte-macrophage colony-stimulating factor (GM-CSF) is a rare cause of neutrophilia (Petterino et al., 2011). In such cases neutrophilia may be extreme (>100 ? 109/L) and differentiation from chronic neutrophilic leukemia (CNL) is warranted. Paraneoplastic leukocytosis differs from CNL by the absence of immature circulating cells, anemia, and thrombocytopenia in the former.
Inherited neutrophil disorders that cause neutrophil hyperplasia include canine and feline leukocyte adhesion deficiency (LAD) and cyclic hematopoiesis (CH). The most common form of LAD is due to an autosomal recessive mutation in the gene that encodes CD18, part of the beta-2 integrins. Neutrophils lacking integrin expression are unable to leave the vasculature, and ensuing bacterial infection and inflammation cause massive neutrophilia and premature death (Bauer et al., 2004). Most reported cases are in Irish setters though mixed breed dogs and cats can also be affected (Zimmerman et al., 2013; Bauer et al., 2017). Cyclic hematopoiesis occurs in collies and collie-like dogs and is due to a mutation in the gene coding for an adapter protein subunit important in the trafficking of proteins such as neutrophil elastase (Lee et al., 2022). Affected dogs have 10–14-day cycles of neutropenia followed by recovery that correspond to periods of marrow neutrophilic atrophy followed by hyperplasia.
Ineffective neutrophil hyperplasia may be seen in steroid-responsive or immune-mediated neutropenia (IMN), where the marrow may be hypercellular with abundant early to band stage neutrophils but a paucity of segmented neutrophils (Perkins et al., 2004). As with NRIMA/PIMA, diagnosis is based on exclusion of other causes of neutropenia and response to immunosuppressive therapy. Ineffective neutrophilic hyperplasia with dysplasia may also be a feature of MDS in dogs.
Eosinophil hyperplasia
Eosinophil hyperplasia results from a persistent demand for eosinophils in hypersensitivity or allergy, inflammation, dermatopathy (feline eosinophilic granuloma complex), parasitism, or due to paraneoplastic cytokine production. Eosinophils transit through the vasculature rapidly but have prolonged tissue survival in the presence of interleukin (IL) 5; hence blood eosinophil concentration may not reflect increased marrow eosinopoiesis. Tumor production of cytokines, in particular T-cell lymphoma, may result in eosinophil hyperplasia.
When a cause of persistent eosinophilia is not identified, primary ‘hypereosinophilic syndrome’ (HES) should be considered. Humans with primary HES may have mutations in growth factors like Fip1-like 1 (FI1L1) or platelet-derived growth factor receptor-α (PDGFRA), clonal T lymphocytes (without lymphoproliferative disease), and increased risk of developing acute myeloid leukemia (AML) (Klion, 2022). Genetic changes are not found in approximately 40% of humans with primary HES, and the condition is then designated ‘idiopathic’ HES. A higher proportion of such patients than those without HES nevertheless progress to AML. Idiopathic HES in cats (Beaumier et al., 2022) and dogs (Casamian-Sorrosal et al., 2020) is characterized by marrow eosinophil hyperplasia, and infiltration and injury of organs such as the heart and lung. Whether there is an underlying genetic abnormality or an increased risk of progression to myeloid neoplasia is unknown.
Granulocytic atrophy
In granulocytic atrophy the marrow is normo- or hypocellular, and erythroid cells are normal or increased, resulting in a low G:E. In all instances, granulocytic atrophy implies neutrophilic atrophy. Genetic causes of neutropenia are uncommon, and generally identified in young animals. Acquired granulocytic atrophy may be due to direct cytotoxic precursor cell injury from drugs such as doxorubicin, hydroxyurea, and vinblastine; idiosyncratic drug reactions to benzimidazole anthelmintics (fenbendazole, albendazole, and levamisole); anti-epileptic medication (phenobarbital, primidone, and phenytoin); griseofulvin, cephalosporin, sulphonamide, methimazole, carprofen, estrogenic compounds such as diethylstilbestrol; valacyclovir and chloramphenicol; and infection with parvo- and other viruses. Marrow cytologic findings are variable depending on the stage and severity of atrophy. There may be a near complete absence of granulocytic cells or there may be a predominance of early precursor cells. If myeloblasts and promyelocytes prevail over differentiated neutrophils in marrow, distinction from AML is important, and repeated CBC, and possibly repeated marrow assessment, is required. In particular, cats recovering from parvovirus infection or cytotoxic injury can have markedly left-shifted granulocytic atrophy that can be difficult to distinguish from AML.
Immune-mediated neutropenia is uncommon in dogs and may be part of IMC in cats. Complete absence of granulocytic cells is termed pure white cell aplasia (PWCA) and is thought to result from immune destruction of myelomonocytic precursor cells comparable to PRCA (Weiss & Henson, 2007). Pure white cell aplasia appears to be rare in animals and humans, and has been associated with thymoma in humans (Cespedes Lopez et al., 2022).
There are many potential causes of granulocytic atrophy. Since lack of production of neutrophils is incompatible with life, the cause of any persistent neutropenia needs to be identified. History and physical examination can rule out most infectious and drug-related causes. If marrow is found to have markedly left-shifted granulopoiesis but normal erythropoiesis and megakaryopoiesis, an early stage of recovery from injury is most likely. Serial hematological assessments are necessary to monitor recovery.
Dysgranulopoiesis
Dysgranulopoiesis refers to abnormalities in granulocyte maturation and morphology, while dysmyelopoiesis refers to abnormalities in any hematopoietic cell lineage. Examples of dysgranulopoiesis are giant neutrophils, abnormal nuclear shapes, abnormal segmentation, hyposegmentation, and hypersegmentation (Figure 19.24). Non-neoplastic causes of dysgranulopoiesis are drug-induced toxicity, sepsis, and cobalamin deficiency. Rapidly regenerating granulocytes may also transiently have dysplastic features. Granulocyte dysplasia is a common feature of MDS and AML, and it can be challenging to distinguish a rapidly regenerating marrow with some dysplastic features from myeloid neoplasia.
Figures 19.24a–c Marrow smears from a dog with neutropenia, 1,000? magnification. There is dysgranulopoiesis as indicated by (a) giant metamyelocytes (arrow) and hypersegmented neutrophils (arrowhead); (b) mitotic neutrophils with fully granular cytoplasm (arrow), and (c) abnormally segmented neutrophils.
Megakaryocyte hyperplasia
Thrombopoietin (TPO) and its receptor MPL regulate megakaryopoiesis and all stages of platelet production except platelet release (Hitchcock et al., 2021). Serum concentration of TPO is inversely proportional to platelet mass; thus conditions with increased destruction or consumption of platelets cause megakaryocytic hyperplasia. In many instances, megakaryocyte hyperplasia is left shifted, and immature megakaryocytes with a high nuclear to cytoplasmic ratio predominate (Figure 19.25). In immune-mediated thrombocytopenia (ITP) platelet lifespan is severely shortened, and a competent marrow responds with massive megakaryocyte hyperplasia. Chronic intravascular coagulation, vasculitis, and early stages of rickettsial infection (e.g. Ehrlichia canis) can also induce megakaryocyte hyperplasia. However, as noted above, marrow aspiration is not indicated when a cause of cytopenia has been identified or is strongly suspected (Gunduz et al., 2014).
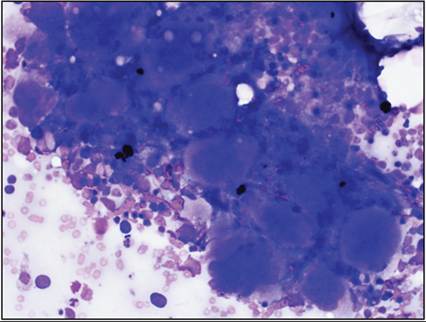
Figure 19.25 Marked megakaryocytic hyperplasia in a dog with immune-mediated thrombocytopenia, 200? magnification.
Megakaryocyte hyperplasia can result in thrombocytosis in chronic inflammatory disorders and iron deficiency. The effect of iron deficiency on megakaryocyte development appears to be independent of TPO but the exact mechanism is not clearly defined (Evstatiev et al., 2014). Tumors can also induce thrombocytosis, and carcinomas were most commonly associated with thrombocytosis in dogs (Cheney et al., 2022; Neel et al., 2012). Megakaryocyte hyperplasia is a common feature of MDS, and is the predominant abnormality in essential thrombocythemia (ET), a myeloproliferative neoplasm.
Megakaryocyte atrophy
Relative to other hematopoietic cells, megakaryocytes occur at low frequency in marrow. Therefore, it may be difficult to appreciate megakaryocyte atrophy in poorly cellular marrow aspirates or those lacking particles. Accurate enumeration of megakaryocytes is therefore better performed on histological sections than cytology films (Travlos, 2006). Presumed immune-mediated megakaryocyte atrophy has been reported in a few dogs (Lachowicz et al., 2004).
Dysmegakaryopoiesis
Micro-megakaryocytes, megakaryocyte hypo- or hyper-lobulation, anisokaryosis, and nuclear separation signify dysmegakaryopoiesis (Figure 19.26). Dysmegakaryopoiesis may accompany accelerated platelet production such as in immune-mediated thrombocytopenia and is often the most prominent feature of MDS. Due to their large size, megakaryocytes may not flatten well on cytology preparations on glass slides, and cellular detail may therefore be difficult to appreciate. Hence, megakaryocyte number and morphology are better assessed on histopathology sections.
Figures 19.26a,b Marrow aspirates from two dogs with dysmegakaryopoiesis. (a) Dwarf megakaryocyte lacking nuclear lobulation, 1,000? magnification. (b) Disconnected nuclear lobes of various sizes, 400? magnification.
Bone marrow infections
There are certain infectious agents that preferentially locate to marrow. Leishmania is a protozoan that may be observed in marrow and no other locations (Figure 19.27). Cytauxzoon involves marrow as one of many sites of infection (Figure 19.28), and fungal infections such as histoplasmosis may be diagnosed from marrow aspirates. Some strains of FeLV induce severe myelofibrosis with lymphoid aggregates, iron accumulation, erythroid atrophy, and anemia (Figure 19.29). Chronic bartonellosis may result in granulomatous inflammation of the marrow, similar to other organs.
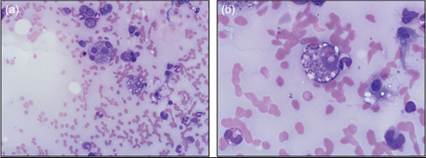
Figures 19.27a,b Marrow aspirate from a dog with epistaxis, ulcerative dermatitis, and emaciation shows Leishmania amastigotes in macrophages (a, 200? magnification; b, 600? magnification).

Figure 19.28 Marrow aspirate from a severely ill and anemic cat contains a Cytauxzoon schizont, 200? magnification. Image provided by J. Tarigo, University of Georgia.
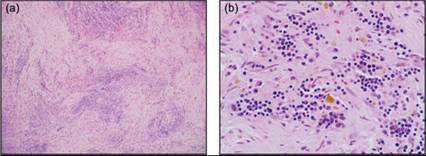
Figures 19.29a,b Marrow core section from a feline leukemia virus-seropositive cat with severe anemia and lymphocytosis; H&E: a, 200? magnification; b, 600? magnification. There is marked myelofibrosis (precluding marrow aspiration) with numerous aggregates of lymphocytes and coarse iron.
Myeloid neoplasia
Myeloid neoplasms are broadly categorized into acute myeloid leukemia (AML), myeloproliferative neoplasm (MPN), and myelodysplastic syndrome (MDS), in accordance with criteria proposed by the World Health Organization (WHO) for humans (Khoury et al., 2022). Categorization is based on morphologic, genetic, and/or immunophenotypic features, but it is increasingly recognized that there is extensive overlap between categories in the underlying genetic lesions and the phenotype. The blast cell count remains a key indicator. The general approach put forth in the 2022 WHO classification of myeloid neoplasms in humans consists of the triad of lineage attribution (morphology and immunophenotype), dominant clinical attributes (acute vs chronic, cytopenia vs cytosis, blast proportion, dysplasia), and biological attributes (gene fusions, rearrangements, mutations). In animals, lineage attributes can be determined with standard hematology analysis incorporating light scatter and impedance, microscopic assessment, cytochemistry, and flow cytometry (Meichner et al., 2020). Clinical attributes are readily derived from history, laboratory results analyzed over time, and marrow interpretation. The biological attributes are more challenging to determine in animals. Precursor conditions for myeloid neoplasia in humans are clonal hematopoiesis of indeterminate potential (CHIP) and clonal cytopenia of undetermined significance (CCUS). These conditions increase in frequency with progressive age and pose a risk for progression to myeloid neoplasia. They likely also occur in animals. Though clonal rearrangements in lymphocyte antigen receptor genes have been noted in dogs with AML, the frequency and nature of clonal hematopoiesis in dogs or cats remain undetermined (Stokol et al., 2017). Albeit, sequencing technologies, analytic pathways, and reference databases are gradually building, which will enable the addition of biological features to the categorization of myeloid neoplasms in dogs in the near future (Harris et al., 2022).
The diagnosis of myeloid neoplasia in animals is often challenging with only routine diagnostic test results and history. Careful integration of history, imaging, hematologic, and marrow findings is needed, and the use of immunophenotyping by flow cytometry (FC), immunohistochemistry (IHC), and/or immunocytochemistry (ICC) is very helpful in characterizing morphologically ambiguous cells. The lineage of blasts can usually not be determined by morphology alone since there is overlap in the appearance of lymphoid blasts, myeloblasts, monoblasts, rubriblasts, and megakaryoblasts. It is essential that the persistent nature of cytopenia is verified, and that other causes of increased blasts, such as drug-toxicity and infection, are ruled out before a diagnosis of myeloid neoplasia is made.
Broadly, AML is defined by persistent cytopenia and ≥20% blasts in blood or marrow. Patients with AML often present with acute illness, but may have had cytopenia or cytosis for weeks or months prior. The proportion of blasts in blood or marrow can range from 20 to 100%, the leukocyte count may be low or extremely high, the marrow may be hypo- or hypercellular, and cells may be dysplastic (Figure 19.30). These variable features reflect the biologic heterogeneity of AML, and pose a diagnostic challenge, in particular in cases with 20–40% blasts. There may be partial differentiation into recognizable progeny cells that allow morphologic subcategorization as ‘AML with neutrophilic, eosinophilic, monocytic, erythrocytic etc. differentiation’ (Figures 19.31, 19.32). It is unclear at this time whether subcategories of AML have different prognoses. While the diagnosis of AML is usually assigned a guarded prognosis, some dogs with AML have responded to combination chemotherapy and survived months to a year (Matsuyama et al., 2023; Tan et al., 2014b). Detection of alkaline phosphatase or peroxidase activity (Figure 19.9) may be helpful to identify myelomonocytic or monocytic and myeloblast cells, respectively (Stokol et al., 2015).
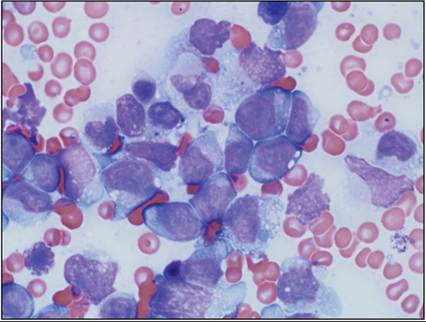
Figure 19.30 Marrow smear from a dog with non-regenerative anemia and acute myeloid leukemia consists predominantly of undifferentiated blasts, 1,000? magnification.
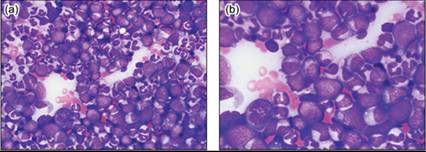
Figures 19.31a,b Marrow smear from a dog with acute myeloid leukemia, partial neutrophilic differentiation, 600? (a) and 1,000? (b) magnification. A 500-cell differential count yielded 46% blast cells.
Myeloproliferative neoplasms are the former chronic leukemias, and are defined by marked cytosis of one cell type, mild cytopenia of other cell types, and ≤5% blast cells in marrow (Figure 19.33). The MPNs are rare in dogs and cats, and it is more likely that a patient with an extremely high neutrophil or eosinophil count has paraneoplastic leukocytosis than an MPN. The pathogenesis of MPN in humans consists of either the constitutive activation of mutated cytokine receptors or independence from normal cytokine regulation (Li et al., 2023). It is likely that MPN in animals have similar pathogenic mechanisms. Subcategorization of MPN is according to the prevailing proliferating cell type into polycythemia vera, chronic neutrophilic or eosinophilic leukemia, essential thrombocythemia, etc. The MPN may manifest with hemoglobin concentration >200g/L and leukocyte counts >200 ? 109/L, and secondary tumor burden effects such as splenomegaly and vascular accidents in the brain, retina, or spleen may precipitate initial clinical assessment.
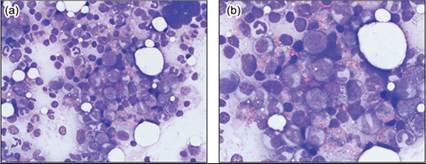
Figure 19.32 Dog with acute myeloid leukemia, partial eosinophilic and basophilic differentiation, 600? (a) and 1,000? (b) magnification. A 500-cell differential count yielded 24% blast cells.
Figures 19.33a,b Dog with myeloproliferative neoplasm, chronic neutrophilic leukemia; 200? (a) and 600? (b) magnification. The dog had mild anemia and a WBC count of 89 ? 109/L with no blast cells in circulation. A 500-cell marrow differential count yielded 5% blast cells.
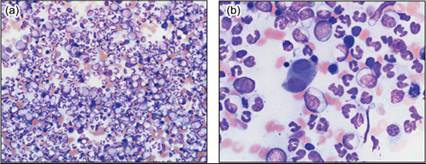
Myelodysplastic syndrome is a broad category of hematopoietic conditions characterized by persistent cytopenia, hypercellular marrow, and dysplasia. The proportion of blast cells in the marrow is between 5 and 20% (Figure 19.34). Hence, the marrow is responding inappropriately and ineffectively to peripheral demand. In humans, specific cytogenetic changes and mutations allow stratification of patients with MDS into prognostically meaningful categories (Li et al., 2023). Similar tests are not yet available for animals; therefore, providing a prognosis for MDS is challenging. Some cases of MDS in dogs progress to AML, others remain static and may become transfusion dependent, and in some cases the cytopenia improves with prolonged immunosuppression. Recently recognized in humans, VEXAS (vacuoles, mutated E1 ubiquitin activating enzyme, x chromosomal location, autoinflammation, somatic mutation) is a syndrome characterized by adult onset of anemia and/or other cytopenia, MDS, variably severe autoinflammation, and clonal hematopoiesis (Gutierrez-Rodrigues et al., 2023). Patients generally improve with immunosuppression, and it could be speculated that some dogs with MDS responsive to immunosuppression may have a condition with similar pathogenesis.
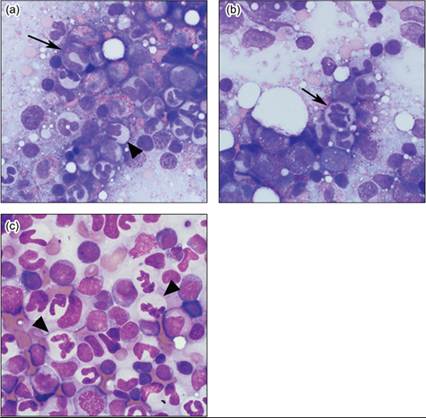
Figures 19.34a–c Dog with myelodysplastic syndrome. (a) The blood smear shows marked anisocytosis, anemia, and acanthocytosis; 200? magnification. There are occasional dysplastic granulocytes (arrow). (b) In the marrow there are abnormally segmented neutrophils (arrowhead); 600? magnification. (c) A lymph node aspirate also contains numerous dysplastic granulocytes; 600? magnification.
Morphologically, MDS should be subcategorized according to the proportion of blast cells and the prevailing cytopenia into refractory anemia with excess blasts (RAEB), refractory neutropenia with excess blasts (RNEB), etc. (Khoury et al., 2022). Myelofibrosis is frequently a component of MDS, but the prognostic implication thereof is undefined.
Non-myeloid neoplasms in bone marrow
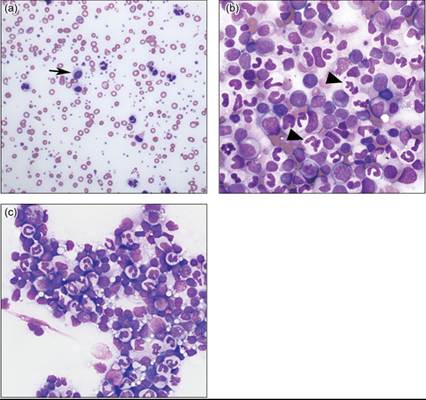
Non-myeloid neoplasms that may arise in or involve marrow include acute lymphocytic leukemia (ALL, Figure 19.35), some types of lymphoma, mast cell tumors, multiple myeloma (Figure 19.36), histiocytic sarcoma (Figure 19.37), carcinoma (Figure 19.38), and others (Pinard et al., 2021). Acute lymphocytic leukemia may be difficult to distinguish morphologically from poorly differentiated myeloid leukemia since both are composed of nearly 100% blast cells. However, immunophenotyping usually allows detection of B- (CD20, CD21, CD79a, Pax-5) or T-cell markers (CD3, CD5) on ALL cells.
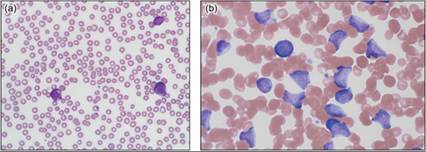
Figure 19.35 Dog with acute lymphoblastic leukemia has pancytopenia with a moderate number of blasts on the blood film (a); 400x magnification. (b) The marrow consists of nearly 100% blasts that expressed CD21 on flow cytometry indicating B-cell type; 600x magnification.
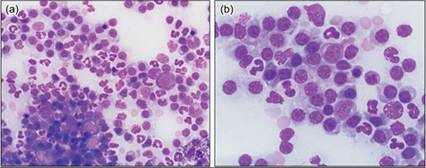
Figure 19.36 Marrow smear from a dog with monoclonal gammopathy and hypercalcemia; 400? (a) and 600? (b) magnification. There are numerous morphologically unremarkable plasma cells among hematopoietic cells.
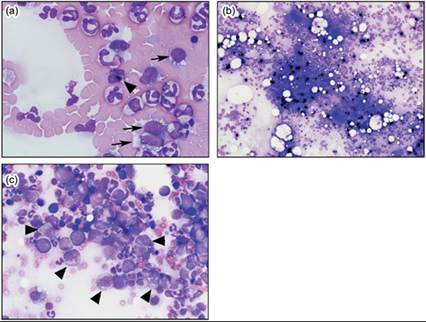
Figure 19.37 Blood film from a dog with mild anemia and histiocytic sarcoma. (a) At the feather tip of the blood film are large round histiocytes with cytoplasmic vacuoles (arrow), and one cell contains heme pigment (arrowhead); 600? magnification. (b) A marrow aspirate shows abundant coarse iron and high cellularity; 100? magnification. (c) There are scattered histiocytes (arrowhead) among hematopoietic cells; 400? magnification. Histiocytes are neither frequent nor easily identified.
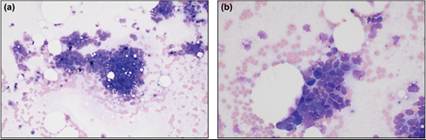
Figure 19.38 Sternal marrow aspirate from a dog with mild anemia and disseminated intravascular coagulation of unknown cause. (a) There are cohesive clusters of non-hematopoietic (epithelial) cells amidst extracellular hemosiderin and a few hematopoietic cells; 200? magnification. Viability among the cohesive cells is variable. (b) The cohesive cells, when intact, have a nuclear to cytoplasmic ratio >1 and dark basophilic cytoplasm with fine vacuoles; 400? magnification. The epithelial cell clusters were noted in two of ten slides evaluated, and were often of limited viability. The interpretation was ‘carcinoma of unknown origin metastatic to marrow’.