16 Ingestion of glue by a dog
Initial presentation
Vomiting and decreased appetite
Signalment: 15-month-old neutered female Bassett Fauve de Bretagne (Fig
16.1), body weight 9.1 kg

Fig 16.1
Bassett Fauve de Bretagne dog at presentation
Case history
The dog had been healthy up until 2 days prior to examination when she was thought to have been playing with a tube of glue.
The owner reported that the dog had chewed off the cap and may have eaten some of the glue. Since then she had vomited twice, starting soon after access to the glue. She then had shown a decrease in appetite. The vomitus contained mostly a green fluid and foam. The owner reported that the dog had also passed a small amount of dark faeces.The dog was de-wormed regularly with fenbendazole and she had received her vaccinations as a puppy. Her regular diet was a commercial dry dog food supplemented with treats.
Physical examination
The dog was quiet but responsive. Her body condition score was 5/9. The mucous membranes were slightly tacky but the colour was pink and capillary refill time was less than 2 seconds. Peripheral lymph nodes were unremarkable.
Thoracic auscultation revealed normal heart and lung sounds, with a heart rate of 100 beats per minute. On abdominal palpation, a firm distended stomach was felt and the dog was uncomfortable during palpation. Respiratory rate was 24 breaths per minute. Rectal temperature was 38.4° C. She had been given no medications.
Problem list and discussion of problems
• Vomiting and poor appetite
The dog’s poor appetite was thought to be related to the vomiting and separate differential diagnoses were not considered.
Differential diagnosis
Differentials for acute vomiting in this dog included:
• Disorders of the stomach
• foreign body
• gastritis
• ulceration
• chronic partial dilatation-volvulus
• neoplasia
• Disorders of the small intestine
• foreign body
• inflammatory bowel disease
• neoplasia
• parasites
• intussusception (unlikely)
• Disorders of the large intestine
• colitis
• obstipation
• Systemic disorders
• pancreatopathy
• hypoadrenocorticism
• diabetes mellitus
• liver disorders
• peritonitis
• renal disease/uraemia (unlikely)
• Dietary causes
• adverse reaction to food (allergy or intolerance)
• dietary indiscretion
Because of the history of potentially having ingested glue and the fact that the dog appeared otherwise very healthy, glue ingestion was the top differential.
Case work-up
The dog was admitted to the hospital for diagnostic investigation.
Minimum data base
Haematology and serum chemistry were performed and the results were unremarkable. Albumin was 35 g/l, at the top of the reference range (26-35 g/l), which was likely due to haemoconcentration from mild dehydration.
Imaging
Abdominal radiographs showed a much distended rounded appearance to the stomach in both ventrodorsal and lateral views (Figs 16.2 and 16.3).
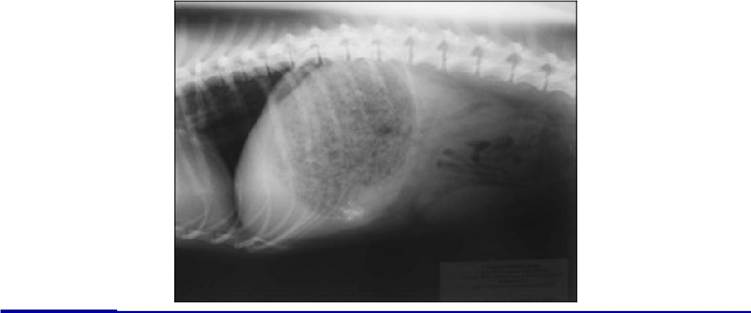
Figs 16.2

Figs 16.2 and 16.3
Lateral and ventrodorsal abdominal radiographs of patient showing stomach distended with a heterogeneous appearing mass
(courtesy of Dr Donald Yool)
Abdominal ultrasound showed the pyloric antrum and pylorus filled with hyperechoic material. The material was not moving despite the presence of peristalsis. The duodenum was empty and the mass appeared to be causing a pyloric obstruction.
Case assessment
Initial case management included administration of intravenous fluids to maintain hydration and provide venous access. As there was the presence of a foreign mass, surgical exploration was performed.
Surgical management
At surgery a large gastrotomy was performed and a dense mass filling the stomach was removed (Fig 16.4). An area of severe gastric ulceration was identified in the gastric mucosa, but the tissue appeared viable and resection was not needed. A prophylactic gastropexy was performed to prevent possible postoperative dilatation and volvulus from the mechanical stretching of the stomach by the mass.

Fig 16.4
The mass of glue which was removed from stomach of the patient
(courtesy of Dr Donald Yool)
Gastric biopsies of the ulcerated area and of a non-ulcerated area of the stomach were submitted for histopathology. There was mucosal loss with severe focal gastric ulceration and submucosal oedema.
Moderate acute gastritis with large numbers of Helicobacter-like organisms were identified deep within the gastric glands in a non-ulcerated area of the stomach.Clinical tip: Helicobacter species
Many species of Helicobacter have been identified in dogs and cats: H. felis,
H. pylori and H. heilmannii (Gastrospirillum hominis), H. salomonis and H. bizzo- zeronii have been themost common. Experimentally, infection can be established in both dogs and cats and a lymphoid follicular gastritis can be produced. However, in these experimental studies, clinical signs are absent or very mild. Several surveys of laboratory and pet populations have shown a very high prevalence rate. Peptic ulceration appears to be very rare in dogs and cats. The role of Helicobacter species in clinical cases of chronic gastritis is unknown, as is the optimal treatment. In approximately 25% of cases in which Helicobacter is identified, it appears to be the cause of or related to the clinical signs and should be treated. When the organisms are deep in the gastric glands (as in this case), rather than located more superficially, it is more likely that they are involved in the pathophysiology of vomiting.
There are several treatment protocols for Helicobacter infection, including 2 weeks of omeprazole 0.7 mg/kg po q 24 hours (or an H2 blocker such as ranitidine), amoxicillin at 10 to 20 mg/kg po q 8 hours, metronidazole 10 mg/ kg po q 12 hours. Other suggestions include omeprazole with either azithromycin at 10 to 20 mg/kg po q 24 hours in dogs and 5 mg/kg po q 24 hours in cats or clarithromycin at 7.5 mg/kg po q 12 hours. Relapses have been seen. One study revealed that 70% of infected dogs can be cleared with triple antibiotic therapy with or without famotidine for 4 weeks. Vomiting decreased significantly in dogs in which the Helicobacter was cleared.
Follow-up and medical management
The dog recovered well after surgery, although she vomited once. Postoperative medical treatment included the anti-emetic maropitant at 1 mg/kg subcutaneously q 24 hours, omeprazole (1 mg/kg q 24 hours po), sucralfate (500 mg q 8 hours po) for their gastroprotectant effects and tramadol (2 mg/kg q 12 hours; initially intravenously, then po) for analgesia.
Treatment for the Helicobacter species found in the gastric biopsy samples was clavulanate-potentiated amoxicillin (15 mg/kg po q 12 hours) and clarithromycin (7.5 mg/kg q 12 hours po) for 2 weeks.Case discussion and epidemiology
Most cases of glue ingestion by dogs (and less commonly, cats) result in gastritis and enteritis; however, expanding glues are associated with gastric obstruction with a foreign body. Gorilla glue is a urethane polymer and polymeric isocyanate liquid which expands to three to four times its original mass when used. The material is activated from a liquid to a solid mass in the stomach when ingested, which probably takes about 20 minutes. It will incorporate food in the stomach into the mass.
Dogs ingesting as little as 2 oz of the glue have developed gastric obstruction. In one report, eight of 10 cases of polyurethane glue ingestion required surgical removal of the mass. Clinical signs usually develop within 12 hours of ingestion (within 30 minutes in one reported case) and include vomiting, possibly haematemesis, anorexia, lethargy, abdominal distension, abdominal pain and secondary tachypnoea. Gastric hyperaemia and ulceration have been reported, as was present in this case, and in one reported case, gastric perforation occurred.
The radiographic appearance (see Fig 16.2) is fairly distinct, with the presence of a distended, stomach filled with a mottled radiopaque substance. Radiographic evidence may be present 4 hours after ingestion, although is more obvious in radiographs taken at 24 hours.
Because of the solid nature of the mass, induction of emesis should not be considered; it is also ill advised as having the glue expand within the oesophagus would cause serious complications. Unlike in most toxin ingestion cases, administration of charcoal is also not advised as it would be incorporated in the mass rather than preventing absorption of the glue (which is unlikely anyway).
Prognosis
If the glue mass is removed without delay and if gastric perforation does not take place, the prognosis for recovery should be good.