15 Lymphocytic inflammatory bowel disease/al- imentary lymphoma in a cat
Initial presentation
2 months of intermittent vomiting, with recent increase in frequency
Signalment: 9-year-old neutered male domestic shorthaired cat; body weight
3.9 kg
Case history
The cat presented with a 2-month history of vomiting and an increasingly poor appetite.
The vomiting had been occurring initially two to three times per week, but during the 2 weeks prior to admission was occurring up to four times per day. The vomitus generally consisted of partially digested food, sometimes with bile present. There had been no diarrhoea, although the amount of faeces had decreased as the cat’s appetite decreased.His previous diet was a commercial dry food supplemented once a day with canned food. During the time his appetite was decreasing the owner had been tempting him with cooked chicken and ham.
His vaccinations were up to date and he had been treated for parasites 3 months prior to presentation. He had not travelled outside of the UK.
Physical examination
On physical examination the cat was bright and alert, but seemed to tire quickly. His body condition score was 3/9. His mucous membranes were pink but slightly dry and capillary refill time was infectious, e.g. bacteria, viral, fungal
• gastrointestinal (GI) parasites
• inflammatory bowel disease
• infiltrative neoplasia, e.g. lymphoma, mastocytosis
• high partial obstruction, e.g. intussusception, foreign body
• Systemic disease
• uraemia
• liver failure
• sepsis
• congestive heart failure
• acidosis
• hypoadrenocorticism
• ketoacidotic diabetes mellitus
• hyperparathyroidism
• gastrinoma
• Neurological diseases (no other signs consistent with these in this cat)
• dysautonomia
• vestibular disease
• CNS disease
• Drugs, toxins (no known history of drug or toxin exposure)
Case work-up
Minimum data base
Haematology, serum chemistry, urinalysis and faecal examination were preformed.
Haematology results were within the reference ranges. Serum chemistry showed a mild decrease in albumin to 24 g/l (reference range 28-39 g/l), and mild hyperglycaemia of 6.7 mmol/l (reference range 3.0-5.0 mmol/l), which was thought to be likely due to stress. Serum total thyroxin was within the reference range at 17.5 nmol/l (reference range 13-48 nmol/l).
The serum cobalamin concentration was decreased to 177 ng/l (reference range 251-908 ng/l) and folate was decreased to 6.4 μg∕ml (reference range 9.7-21.6 μg/^.
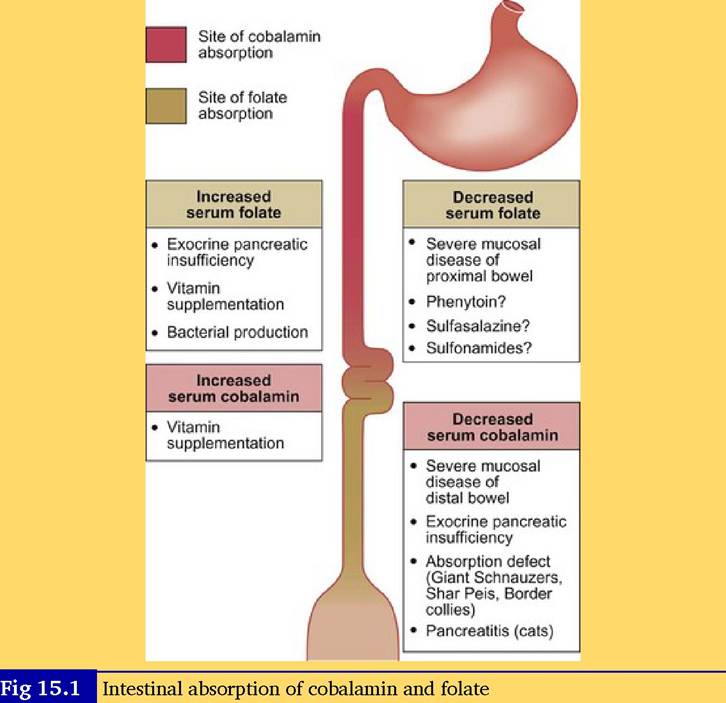
Clinical tip: folate and cobalamin (vitamin Bι2)
Cobalamin is absorbed in the ileal part of the small intestine. It requires prior binding with intrinsic factor, which comes from the pancreas in cats and the stomach and pancreas in dogs. Deficiency may be caused by poor absorption due to intestinal disease, exocrine pancreatic insufficiency, excessive bacteria in the upper small intestine utilizing the vitamin, or a deficiency in intrinsic factor. In humans who are vegetarians (especially elderly humans), a dietary deficiency is possible; however, this is unlikely in cats as they cannot successfully be vegetarians.
Unlike most other B vitamins, cobalamin is stored in the body. In healthy cats the half life is 11 to 14 days and in cats with GI disease it is only 4.5 to 5.5 days. Clinical signs of cobalamin deficiency in humans include anaemia, thrombocytopenia, neuropathies and digestion abnormalities. In cats (and dogs) the clinical signs are not as well described; however, it has been suggested that response to treatment of intestinal disorders is improved with cobalamin repletion. A high serum concentration of cobalamin does not appear to have clinical significance and may occur with supplementation. The recommended dose for supplementation in humans exceeds the amounts needed to reach serum reference ranges and there is a consideration that there may be positive pharmacological effects.
Folate is absorbed only in the proximal intestine.
A deficiency usually indicates small intestinal disease and if it is accompanied by a cobalamin deficiency it likely indicates widespread disease. A high serum folate can becaused by bacterial production, although serum concentrations of this vitamin are sensitive to food intake and a high dietary intake can also increase the serum concentration (Fig 15.1).
Serum titres for Toxoplasma gondii were zero for IgM and 100 for IgG, inconsistent with the presence of this organism. Blood test results for feline leukaemia virus (FeLV) and feline immunodeficiency virus (FIV) were also negative.
Urinalysis showed a urine specific gravity of 1.026. The chemical strip analysis results were within reference ranges and the urine sediment was inactive. Urine protein to creatinine ratio was within the reference range (as the intestine is nourished by the luminal presence of nutrients, especially glutamate in the small intestine.
The estimation of caloric requirements for hospitalized patients is based upon the resting energy requirement, which is in kcal 70 ? body weight in kilograms0-75. The presenting weight is used initially, rather than the optimal weight. In this cat, this value was:

The estimated amount to initiate feeding was decreased to one-third of this amount, or 65 kcal to decrease the risk of the re-feeding syndrome. The key tips for nutritional supplementation of sick animals are to feed early and to try to not feed too much.
As this cat was vomiting, the provision of oral or gastric nutrition could have been difficult. Constant rate intravenous metoclopramide was administered with his intravenous fluids at a rate of 1 mg/kg/24 hours.
The initial feeding attempted was the use of a complete and balanced liquid food containing 1 kcal/ml.
This was administered by gentle oral administration at 8 ml given eight times per day. This was not completely successful, as the cat would often only tolerate about 5 ml, which provided 40 kcal per day. While not ideal, this is still satisfactory for initial feeding. The cat was also offered chicken and white fish and on the second day began to eat several grams per day, adding about 30 to 50 kcal to his intake.A naso-oesophageal tube could have been placed to feed the cat; however, there was a risk of vomiting the tube and having it displaced into the trachea. If the cat had not started eating, placement of a jejunostomy tube and/or intravenous parenteral nutrition would have been indicated.
By the end of the first week, the cat was eating a complete canned food in adequate amounts and had only vomited on days 4 and 6. He was discharged on oral medications, with repeat visits for evaluation and cobalamin administration.
He gained 0.6 kg over the 2 months following diagnosis and the owner reported that he vomited only once or twice a week and was much brighter and more active. His urine specific gravity did not increase above 1.030; however, he did not become azotaemic and his kidney disease appeared stable. He was lost to follow-up 1 year after the tentative diagnosis of intestinal lymphoma.
Discussion and epidemiology
As more cats are vaccinated for FeLV, the more common site of feline lymphoma has shifted from the mediastinal form to the GI form, which most often affects the small intestine. Cats with GI lymphoma have a lower incidence of FeLV (15%) infection than do cats with other forms of lymphoma (20-85% depending upon the site), although the true incidence might be higher if more sensitive tests were used (e.g. PCR testing).
The most common age range of cats with GI lymphoma is 9 to 13 years. There is no evidence of a breed predilection, but male cats are slightly more likely to develop the disease. As in this cat, the signs are chronic and often include a poor appetite and weight loss.
Vomiting is reported in fewer than 50% of cases and diarrhoea is present in about 30%, so absence of GI signs does not rule out the disease. Cats with low- grade lymphoma are likely to have palpably thickened loops of bowel.Some cases show a non-regenerative anaemia consistent with anaemia of chronic disease or bone marrow infiltration of the tumour in cases with FeLV. Mild to moderate hypoalbuminaemia is often present; however, this is common with many diseases of the small intestine. In some cases liver involvement in the neoplasia results in increased liver enzymes.
Low serum cobalamin and folate are present in many cases, but again, this is true of many small intestinal diseases where absorption is decreased.
The increased intestinal wall thickness is characteristic, but does not differentiate GI lymphoma from inflammatory bowel disease. The disruption of normal intestinal wall layering is usually more pronounced with lymphoma than other inflammatory bowel disease. The increase in mediastinal lymph node size is a non-specific finding common in many abdominal disorders.
Histology of GI biopsies is needed for a definitive diagnosis, but even then the diagnosis can be difficult. There are three grades of GI lymphoma: • Low - lymphocytic or small cell
• Intermediate • High - lymphoblastic, immunoblastic or large cell.
It can be extremely difficult, even with histopathology, to differentiate low grade small cell lymphoma from lymphocytic inflammatory bowel disease. Many clinicians believe that inflammatory bowel disease may lead to lymphoma in some cases. CD79a (B-cell) and CD3 (T-cell phenotype) antibody stains can be used to assess B- and T-cell immunoreactivity to help differentiate between the disorders. A predominance of one type of cell is more likely to be tumour and a mixed population more likely to be IBD. While an aid in diagnosing, the type of tumour cell (B versus C) does not correlate to response to therapy or survival time in cats.
Treatment discussion
Various chemotherapy protocols have been used for GI lymphoma; these include various combinations of cyclophosphamide, vincristine, prednisolone, L-asparaginase, doxorubicin and methotrexate. Remission rates with these protocols are difficult to interpret as many studies do no include the histological grade of the disease and remission rates are better for low grade small cell lymphoma.
Cats with low grade lymphoma, such as this cat, can often have a good response to the less aggressive chemotherapy protocol of chlorambucil and prednisolone with less risk of serious side effects. A remission rate of 69% has been reported with this treatment in these cases, with a median survival time of 17 months. Cats which achieve complete remission have better survival times. It may be that some of the cats treated for small cell lymphoma have a form of inflammatory bowel disease; however, the treatment appears to be appropriate for either disorder.