14 Hypoadrenocorticism in a dog
Initial presentation
Vomiting, weakness and lethargy
Signalment: 6-year-old neutered female cocker spaniel, body weight 17 kg
Case history
The dog had become lethargic during the past month and was vomiting digested food 3 to 4 times a week.
Her exercise tolerance had decreased over the last 1 to 2 months. Her stools varied between normal and soft. The owner was unsure if the dog’s drinking and urination patterns had changed.The dog was de-wormed regularly with fenbendazole and she was vaccinated yearly.
Her usual diet was a high quality dry food and she was also given snacks and treats regularly. She was on no medications or supplements.
Physical examination
The dog was very depressed at presentation. Her body condition score was 4/9 with evidence of recent weight loss. Her mucous membranes were tacky; capillary refill time was 3 seconds. Peripheral pulse quality was weak, but there was a pulse for every heart beat. There was a slight loss of skin elasticity. Based on these findings, she was estimated to be approximately 7% dehydrated.
Peripheral lymph nodes were unremarkable. Thoracic auscultation revealed normal heart and lung sounds, with a heart rate of 56 beats per minute (bpm). This heart rate was thought to be too slow for the degree of dehydration. She had a respiratory rate of 36 breaths per minute and her rectal temperature was 38.9° C.
Problem list and discussion of problems
• Vomiting
• Decreased exercise tolerance
• Slow heart rate, especially for hypovolaemia
Differential diagnosis
Differential diagnoses for vomiting in this dog include the following disorders:
• Disorders of the stomach
• foreign body
• gastritis
• ulceration
• chronic partial dilatation-volvulus
• neoplasia
• Disorders of the small intestine
• foreign body
• inflammatory bowel disease
• neoplasia
• parasites
• intussusception (unlikely)
• Disorders of the large intestine
• colitis
• obstipation
• Systemic disorders
• pancreatopathy
• hypoadrenocorticism
• diabetes mellitus
• liver disorders
• peritonitis
• renal disease/uraemia (unlikely)
• Dietary causes
• adverse reaction to food (allergy or intolerance)
• dietary indiscretion
Most dogs with intussusception are less than 1 year of age, although it is still a possible diagnosis in a dog of this age.
Differential diagnoses for decreased exercise tolerance in this dog include:
• Cardiovascular disease
• Neuromuscular disorders such as myasthenia gravis, peripheral neuropathies, brain or spinal cord disease, myopathies
• Respiratory disorders
• Electrolyte disorders, e.g. hypo- or hyperkalaemia, hypo- or hypernatraemia, hypocalcaemia
• Endocrine diseases such as diabetes mellitus, hypothyroidism, hypoglycaemia, hypoadrenocorticism
• Infectious disease
• Anaemia
• Nutritional deficiencies or malassimilation of nutrients
• Neoplasia
• Medications or toxins; however, the dog had no history of ingestion of these
• Pain - although there was no evidence of pain on physical examination, this can be subtle
A heart rate of 56 bpm is considered bradycardic for a medium sized dog and the degree of hypovolaemia would be expected to have increased the rate. Possible causes for the bradycardia include:
• increased vagal tone
• hypothyroidism
• sinus node disease (sick sinus syndrome)
• sinus block due to atrial disease
• atrial standstill (e.g. due to hyperkalaemia) or an atrioventricular heart block
Very fit dogs sometimes have a slow heart rate, but this dog did not appear fit and also had not been exercising normally for the past month or longer.
Case work-up
The dog was admitted to the hospital for diagnostic investigation and treatment of her dehydration. Intravenous balanced electrolyte crystalloid fluids were initially started at 85 ml/hour, calculated to correct her dehydration over 24 hours.
Nursing tip on intravenous fluid therapy
Fluid therapy needs to take into account the amount needed for maintaining normal hydration and replenishing the amount lost. Maintenance fluids are usually calculated at 40 to 60 ml/kg per 24 hours or 1.6 to 2.5 ml/kg/ hour. In this 17 kg dog, that was approximately 34 ml/hour. To replete the amount of fluid deficit, the dog’s body weight is multiplied times the estimated amount of dehydration, e.g.
17 ? 0.07 = 1.19 kg or 1.19 l in 24 hours. This is 1190 ml in 24 hours or about 50 ml/hour. Adding the 34 ml plus 50 ml is 84 ml/hour. The pet’s hydration should be assessed several times during fluid administration as sometimes hydration improves before this total amount is given. If the pet is vomiting or has diarrhoea, sometimes additional fluid needs to be given to make up these ongoing losses.Minimum data base
Haematology, serum chemistry and routine urinalysis were performed. Haematology results showed an increased packed cell volume (PCV) of 0.56 l/l (reference range 0.37-0.55 l/l).
Clinical tip on PCVs
While the upper end of the range of PCV for most laboratories is above 0.50 l/l, the upper end of the reference range is more typically seen in greyhounds and other sighthounds. When values above 0.50 l/l are seen in other breeds, haemoconcentration should be considered, which is often due to dehydration. Values above 0.60 l/l may even be due to polycythaemia.
Serum chemistry results including basal cortisol were performed and showed a marked hyperkalaemia of 6.1 mmol/l (reference range 3.6-5.6 mmol/l), a hyponatraemia of 131 mmol/l (reference range 135-154 mmol/l), an increased albumin of 38 g/l (reference range 26-35 g/l), increased calcium of 3.2 mmol/l (reference range 2.3-3.0), increased urea of 8.1 mmol/l (reference range 1.7-7.4 mmol/l) with a creatinine at the high end of the reference range at 131 μmol∕l (40-132 μmol∕l) and a decreased glucose of 2.7 mmol/l (reference range 3.0-5.0 mmol/l). Basal serum cortisol was decreased at less than 13.5 nmol/l (reference range 20-230 nmol/l; lowest detectable amount at 13.5 nmol/l).
Clinical tip on use of basal cortisol
While an adrenocorticotrophin hormone (ACTH) stimulation test is the definitive diagnostic test for hypoadrenocorticism, a serum basal cortisol concentration of greater than 70 ng/l effectively rules out hypoadrenocorticism. This test should probably be run in any dog with unexplained gastrointestinal signs or weakness, regardless of the electrolyte concentrations.
Clinical tip on sodium: potassium ratios
Sodium to potassium ratios of less than 27 have been used to diagnose hypoadrenocorticism, but other differential diagnoses for hyponatraemia with concurrent hyperkalaemia should include (as well as hypoadrenocorticism): renal failure, chylothorax and gastrointestinal tract disorders. The ACTH stimulation test is the gold standard for definitive diagnosis of hypoadrenocorticism.
Only a very small amount of urine was obtained by cystocentesis. The urine specific gravity was 1.019, which was inappropriately low for the degree of dehydration. The chemical strip showed a pH of 5.5 with no blood, bilirubin or glucose.
As these results are consistent with, but not diagnostic for hypoadrenocorticism and there was evidence of hypoglycaemia, the fluids were changed to 0.9% saline with 5% glucose and the rate was increased to 100 ml/hour.
Imaging
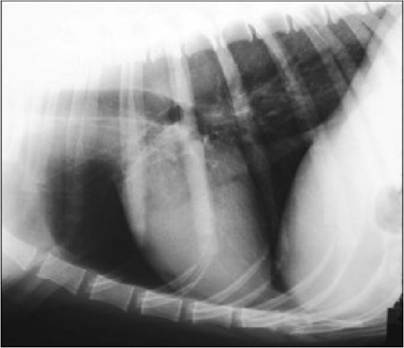
Thoracic radiographs showed microcardia and a small vena cava, consistent with dehydration (Figs 14.1 and 14.2). Abdominal ultrasound showed very small adrenal glands bilaterally (Figs 14.3 and 14.4).
Figs 14.1

Figs 14.1 and 14.2
Lateral and ventrodorsal thoracic radiographs showing
the decreased heart and vessel size consistent with dehydration
(courtesy of Dr Tobias Schwarz)

Figs 14.3

Figs 14.3 and 14.4
Ultrasound pictures of the left and right adrenal glands,
both of which are decreased in size
(courtesy of Carolina Urraca del Junco)
Electrocardiogram
The dog started to deteriorate with to the results being available. An formed which showed a heart rate absence of P waves, consistent with
a slower heart rate of 46 bpm prior electrocardiogram (ECG) was per- of 48 bpm, spiked T waves and an the hyperkalaemia (Fig 14.5).
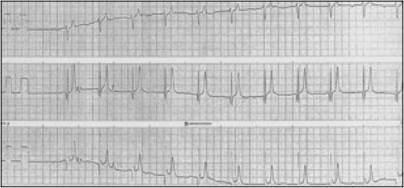
Fig 14.5
ECG showing bradycardia (heart rate 48 bpm), flattened P waves and spiked T waves typical of atrial standstill with hyperkalaemia
(courtesy of Geoff Culshaw)
ACTH stimulation test
An ACTH stimulation test was performed. Serum results of the post- ACTH stimulation test were less than 13.5 ng/l, confirming the diagnosis of hypoadrenocorticism.
Initial treatment
The fluid rate was increased to 850 ml/hour for an hour (50 ml/kg/ hour) using normal (0.9%) saline, and intravenous hydrocortisone sodium succinate was administered at 10 mg/kg every 6 hours.
Follow-up
The dog responded very well to treatment and the following day was brighter and interested in eating. She was started on oral fludrocortisone at 0.2 mg (total dose) po q 24 hours and an initial dose of prednisolone at a physiological dose of 0.15 mg/kg po q 24 hours.
Outcome
The prednisolone was discontinued 1 week later; however, the owners kept a supply in case the dog suffered a stressful incident. Haematological and serum chemistry parameters returned to within the reference range other than a tendency to have potassium concentrations at the high end of the reference range and sodium just below the reference range.
She has continued to do well several months after diagnosis and her prognosis for a normal life is good, although she will need lifelong medication.
Case discussion
In typical hypoadrenocorticism there is a deficiency of aldosterone and glucocorticoids. Aldosterone normally promotes sodium retention and water reabsorption as well as potassium excretion, especially in the renal tubules. The aldosterone deficiency leads to the electrolyte imbalances of increased potassium and decreased sodium, causing the clinical signs of impaired cardiac conduction and bradycardia, lethargy and nausea. Glucocorticoid deficiency causes loss of appetite, vomiting, diarrhoea and lethargy.
An atypical form of hypoadrenocorticism also occurs in which there is only a glucocorticoid deficiency and no change in the serum electrolyte concentrations. These dogs may still show gastrointestinal signs and weakness.
Because hypoadrenocorticism can occur with or without electrolyte changes, this diagnosis should be considered in the differential diagnoses for any dog with any combination of weakness, gastrointestinal signs (vomiting or diarrhoea) or polyuria/polydipsia. The clinicopath- ological abnormalities of azotaemia, increased calcium and inappropriately low urine specific gravity may appear similar to kidney disease.
A basal cortisol is useful in ruling out hypoadrenocorticism as a value greater than 70 nmol/l will rule this out, while in a patient with a value less than that an ACTH stimulation test should be performed.
Concurrent hypovolaemia affects many of the parameters measured, in that albumin, urea, creatinine and the PCV appear higher than they will be after the dog is rehydrated. The inappropriately low urine specific gravity is caused by the impaired concentrating ability secondary to chronic sodium loss reducing the renal medullary concentration gradient.
The weakness may also be exacerbated by hypoglycaemia due to the lack of glucocorticoids, so the blood glucose should always be checked and treated if necessary. Mild to moderate hypercalcaemia is seen in about a third of dogs with hyperadrenocorticism; the cause of this is not yet known.
Medical management
Hyperkalaemia can be life-threatening and should be treated with aggressive fluid therapy with normal saline (0.9% sodium chloride). If hypoglycaemia occurs, either 5% glucose should be provided intravenously or a slow bolus of 50% glucose at 1 ml/kg should be given intravenously.
Glucocorticoid therapy should be administered early in the treatment. If there is a strong suspicion of hypoadrenocorticism, it should be given as soon as the ACTH stimulation test is completed rather than waiting for the results. If the dog is in a potentially fatal crisis, dexamethasone may be given prior to the test as it will not interfere with the assay, although it will affect the test results.
Mineralocorticoid treatment is not necessary in a crisis situation, although it will be needed for longer term management. Hydrocortisone does have some mineralocorticoid as well as glucocorticoid activities, although prednisolone sodium succinate or dexamethasone sodium succinate may also be used.
For longer term use, fludrocortisone acetate per os at an initial dose of 15 μg∕kg q 24 hours is usually used in the United Kingdom, although injectable desoxycorticosterone pivalate is available in some countries. The dose of fludrocortisone often needs to be increased during the first year of treatment in many dogs to maintain the serum potassium concentration within the reference range and some dogs may need twice daily dosing.
Glucocorticoid (e.g. prednisolone) therapy is usually not needed on a daily basis in dogs treated with fludrocortisone (although may be needed in those treated with desoxycorticosterone pivalate). Owners are usually provided with a supply of prednisolone tablets to be given at a dose of 0.1 to 0.2 mg/kg/day if the dog appears to show clinical signs.
Salt supplementation may help the initial hyponatraemia, especially early in the treatment period. Many affected dogs do have a serum sodium concentration slightly below the reference range regardless of salt supplementation and this does not appear to affect them clinically if the serum potassium concentrations are well managed.
Epidemiology
While hypoadrenocorticism can occur in any breed, there has been a greater incidence reported in Great Danes, Portuguese water dogs, Rottweilers, standard poodles, West Highland white terriers, soft coated wheaten terriers, Nova Scotia duck tolling retrievers and bearded collies. It occurs most often in young to middle aged dogs (e.g. 4-6 years of age) and more often (70%) in female dogs (except in bearded collies and standard poodles, where both genders are affected equally). Intact female dogs appear to have a higher risk than spayed female dogs.
Prognosis
Hyporadrenocorticism can be life-threatening if not rapidly recognized and treated. The disorder requires lifelong management. Nevertheless, with good client compliance, the prognosis is excellent. In one study, 100% of 98 treated dogs survived to discharge.