13 Pancreatitis and alimentary lymphoma in a dog
Initial presentation
Vomiting
Signalment: 5-year-old male entire Beagle, body weight 12 kg
Case history
The dog presented with a week long history of vomiting and decreased appetite.
The vomitus contained food and bile and occurred at least once a day. The frequency of vomiting had increased over the past month. He had had a similar episode 5 months earlier which had responded to treatment with oral electrolyte solutions and antibiotics.The owners thought that he had lost weight, but were unsure of how much. He was lethargic, although the owners reported that he was usually a quiet dog. His stools had been soft and somewhat dark in colour during the last couple of weeks, although also scant as he had not been eating well.
The dog had last been de-wormed 3 months previously, but had not been vaccinated for about 3 years. His previous diet was a dry food bought at the grocery store, plus snacks and treats of human food. He was being tempted to eat small amounts of chicken and ham at presentation. He was on no current medication.
Physical examination
The dog’s demeanour was dull but responsive. He was estimated to be about 6% dehydrated. His body condition score was good at 5/9, although there was evidence of muscle loss over his epaxial, lumbar and temporal muscles. Mucous membrane colour was pink and capillary refill time was less than 2 seconds. Peripheral lymph nodes were unremarkable.
Thoracic auscultation revealed normal heart and lung sounds, with a heart rate of 96 beats per minute and respiratory rate of 16 breaths per minute. There was evidence of mild to moderate pain on palpation of the cranial abdomen. Rectal temperature was decreased at 36.7° C.
Problem list and discussion of problems
• Vomiting
• Abdominal discomfort
• Low rectal temperature
Differential diagnosis
Vomiting was the dog’s main problem and it was the one initially addressed.
Differential diagnoses for vomiting in this dog include the following disorders:• Disorders of the stomach
• foreign body
• gastritis
• ulceration
• chronic partial dilatation-volvulus
• neoplasia
• Disorders of the small intestine
• foreign body
• inflammatory bowel disease (IBD)
• neoplasia
• parasites
• intussusception (unlikely)
• Disorders of the large intestine
• colitis
• Systemic disorders
• pancreatopathy
• hypoadrenocorticism
• diabetes mellitus
• liver disorders
• peritonitis
• renal disease/uraemia (unlikely)
• Dietary causes
• adverse reaction to food (allergy or intolerance)
• dietary indiscretion
Most dogs with intussusception are less than 1 year of age, although it was still a possibility in a dog of this age. He did not have any other signs of renal disease, so uraemia was an unlikely cause of the vomiting.
Differential diagnoses for cranial abdominal pain in this dog included:
• Pancreatitis
• Gastritis • Hepatopathy
• Peritonitis
• Pyelonephritis was unlikely as the pain was cranial and not over the area of the kidneys
• Occasionally back pain and abdominal pain may be difficult to differentiate, but this dog showed very localized pain which appeared unlikely to be coming from the spine or epaxial muscles
Low rectal temperature may be due to decreased ambient temperature, (which was not the case here) shock or other disorders of peripheral circulation, hypothyroidism, or to placement of the thermometer within a faecal ball in the rectum. One of the latter two differential diagnoses was thought to be most likely in this case.
Case work-up
The dog was admitted to the hospital for diagnostic investigation and fluid therapy to correct the dehydration.
Minimum data base
Haematology, serum chemistry and routine urinalysis were performed. Haematology results showed an elevation in white blood cell with a neutrophil count of 23.5 ? 109∕l (reference range 3.6-12.0 ? 109∕l), band or meta neutrophils of 1.4 ? 109∕l (reference range 0 for this laboratory) and monocytes of 2.24 ? 109∕l 9 (reference range 0-1.5 ? 109∕l).
His packed cell volume (PCV) was 0.54 l/l, within the reference range of 0.39 to 0.55 l∕l, but high for a dog not of the sighthound breeds.While the upper end of the range of PCV for most laboratories is above 0.50 l/l, the upper end of the reference range is more typically seen in greyhounds and other sighthounds. When values above 0.50 l/l are seen in other breeds, haemoconcentration should be considered, which is often due to dehydration. Values above 0.60 l/l may even be due to secondary poly- cythaemia or polycythaemia vera.
Serum chemistry results showed a decreased albumin of 21.9 g/l (reference range 26-35 g/l) and a globulin in the low end of the reference range at 19 g/l (reference range 18-37 g/l). Serum urea was mildly increased at 7.6 mmol/l (reference range 1.7-7.4 mmol/l) and sodium was decreased at 135 mmol/l (reference range 139-154 mmol/l) with potassium within the reference range at 4.0 mmol/l. Cholesterol was decreased at 3.1 mmol/l (3.8-7.0 mmol/l) and triglycerides were within the reference range at 0.73 mmol/l (range 0.57-1.14 mmol/l). Lipase was extremely increased at 2330 IU/l (reference range 13-200 IU/l), although amylase was within the reference range at 22.1 pmol/l (reference range 15-26 pmol/l). A canine-specific lipase was run to confirm this and was also highly elevated at 998 mmol/l (reference range less than 200 mmol/l).
Basal serum cortisol ruled out hypoadrenocorticism with a value of 202 nmol/l.
A serum thyroxine (total T4) concentration was decreased at 8 nmol/l (reference range 15-48 nmol/l).
Urinalysis was unremarkable on chemical strip and sediment and the specific gravity of urine was 1.047.
Serum amylase and lipase may reflect pancreatitis in the dog, although specificity of these tests is only about 50%. Serum amylase is particularly undiagnostic, as noticed in this case where the value was within the reference range in a severe case of pancreatitis. Serum amylase and lipase should be used only as preliminary screening tests if the more reliable specific canine pancreatic lipase immunoreactivity (cPLI) test is not immediately available.
There is also an in-house qualitative kit form of the cPLI test. The sensitivity of the laboratory-based cPLI is above 80% and it is also highly specific.Imaging
Abdominal ultrasound showed an enlarged irregular pancreas with focal fluid accumulation and a corrugated appearance to the duodenum. The small intestine was considered to be otherwise normal in width and layering. There was no evidence of peristalsis in the proximal small intestine.
Diagnosis
From the history, clinicopathological parameters and ultrasound results, a diagnosis of pancreatitis was made.
Medical treatment
Initial treatment included intravenous balanced crystalloid fluid therapy at a rate calculated to correct dehydration within 24 hours, intravenous clavulanate-potentiated amoxicillin (20 mg/kg iv q 8 hours), buprenorphine (20 μg∕kg q 6 hours) for analgesia, ranitidine (2 mg/kg subcutaneous q 12 hours), metoclopramide in a constant rate infusion (1 mg∕ kg constant rate infusion in 24 hours in iv fluids) and sucralfate (1.5 ml per os (po) q 8 hours). The sucralfate had to be discontinued as the dog could not take anything po without vomiting.
The total T4 was decreased in this dog, which could have been due to hypothyroidism or to the euthyroid sick syndrome. It was planned to investigate this further after treatment of the more severe disorders. While the dog was lethargic and had a low rectal temperature, he did not have alopecia, high cholesterol, hypertriglyceridaemia or (even after rehydration) anaemia.
Clinical tip on anti-emetics
Oral or subcutaneously administered metoclopramide has a relatively short half life and it is more efficacious if given as a constant rate infusion. It may adversely affect pancreatic blood flow as it is a dopamine agonist and the blood flow to the pancreas is regulated via dopamine receptors. Maropitant, a neurokinin 1 antagonist with broad spectrum actions, may have been a better choice in this dog, although it was not yet available at the time this case presented.
It does not have the promotility effects of metoclopramide, which were desired in this case. Another anti-emetic that may be useful in pancreatitis is dolasetron which is a 5HT antagonist and a very potent anti-emetic (but which was also not available at the time of this case).Clinical tip on antibiotic use in pancreatitis
There is much debate about whether or not to use antibiotics in cases of
canine pancreatitis. In humans, infection is a common complication of pancreatitis, although there is limited evidence that human patients treated with prophylactic antibiotics have a better outcome. While most clinicians treat cats with pancreatitis with antibiotics, the decision is more difficult in dogs, as infection is thought to be less likely. In this case (rightly or wrongly) the decision was made to use an antibiotic, due to the presence of a left shift or increase in band neutrophils.
Nursing aspects of feeding in cases of pancreatitis
It has previously been recommended to withhold food from patients with pancreatitis, which is sensible in patients that are vomiting. In humans there is no evidence that withholding nutritional supplementation is beneficial and even some that it may be detrimental. Current thinking is to withhold food only from dogs which are vomiting and then only for 2 to 4 days. If antiemetics do not control vomiting, then parenteral support (e.g. partial parenteral nutrition via a peripheral vein) or enteral support via a jejunostomy tube are recommended. Parenteral nutrition has the advantage of not requiring anaesthesia for placement as does a jejunostomy tube. In dogs that are not vomiting, small amounts of low fat and moderate carbohydrate foods may be offered in small frequent meals. There is no scientific evidence that a high fat meal causes pancreatitis, but there is anecdotal evidence that the dogs appear to do better if offered low-fat foods during recovery. Feeding low-fat food also appears to cause resolution of signs in some chronic low-grade cases of pancreatopathy.
After 2 days of treatment, the dog’s clinical signs had waxed and waned, but overall had failed to respond and he was still depressed and vomiting. Repeat haematology and serum chemistry was performed. This showed an improvement, in although still elevated, serum lipase to 875 IU∕l (reference range 13-200 IU∕l), but a fall in the albumin to
15.8 g/l (reference range 27-35 g/l) and also a decrease in globulin to
17.8 g/l (reference range 18-37 g/l). Serum urea was now within the reference range at 5.4 mol/l (reference range 1.7-7.4 mol∕l) and PCV had decreased to 0.48 l/l. Urine protein to creatinine ratio was 0.3, effectively ruling out a protein losing nephropathy. Liver function tests other than albumin (e.g. serum bile acids and bilirubin) as well as liver enzymes were within reference ranges, making a hepatopathy unlikely.
Clinical tip on the Clinicopathological effect of dehydration
Dehydration affects many Clinicopathological parameters, notably increasing PCV, haemoglobin, urea, creatinine (prerenal azotemia), albumin, globulins and sodium. This can increase some parameters above the reference range, such as urea and creatinine; however, it can also mask low values for others, such as proteins and PCV. These parameters, especially if in the lower end of the reference range, should be re-evaluated after rehydration.
A gastrointestinal disorder in addition to the pancreatitis was suspected and gastrointestinal endoscopy was performed.
Endoscopy
At endoscopy, the stomach had thickening of the rugal folds (Fig 13.1) and the small intestinal mucosa was very roughened and abnormal in appearance with some bleeding present (Fig 13.2). Mucosal biopsies were taken of the stomach and small intestine.
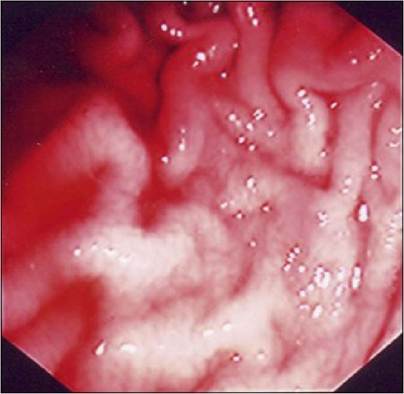
Fig 13.1
Endoscopic view of the stomach, showing lack of distension and a
roughened appearance of the rugal folds
Fig 13.2
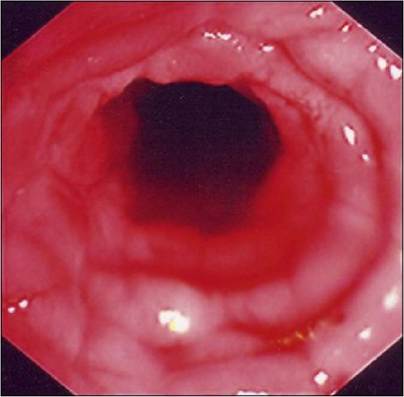
Endoscopic view of roughened small intestinal mucosa, with bleeding present
Histopathology
Histopathology of the stomach showed oedema and congestion of the lamina propria, some focal haemorrhage and areas of erosions with underlying inflammation. In the gastric cardia, biopsies showed extensive fibrosis and atrophy of the gastric glands. This was interpreted as moderate to severe inflammatory gastritis.
The duodenum had severe diffuse and nodular infiltration of the lamina propria with immature, noncleaved lymphocytes. There was widespread villus blunting and atrophy. This was interpreted as alimentary lymphoma.
Follow-up
As these owners did not want to pursue therapy, the dog underwent euthanasia. A necropsy confirmed extensive infiltration of small lymphocytes within the villi, lamina propria and extending below the villi and into the submucosa in some areas. The mesenteric lymph nodes also showed effacement in flat fields of small lymphocytes. The subcapsular sinus of the lymph nodes was also heavily infiltrated with small lymphocytes.
The thyroid glands had atrophied follicles with nearly complete absence of colloid, but no inflammatory cells present. It appeared that the dog was hypothyroid due to idiopathic follicular atrophy rather than active lymphoid thyroiditis; in this diagnosis it is unclear whether the follicular atrophy is a distinct syndrome or the final result of previous lymphoid thyroiditis.
Case discussion and epidemiology
This case demonstrates the pitfall of assuming that there is only one aetiology for a patient’s clinical signs, in that he had more than one cause for his vomiting. As neither pancreatitis nor hypothyroidism are known risk factors for intestinal lymphoma, it is likely these diseases occurred independently in this unlucky dog. His pancreatitis was resolving and the hypothyroidism was treatable, so the final diagnosis is the intestinal lymphoma.
Alimentary lymphoma constitutes 7% of canine lymphoma cases and can occur diffusely as in this dog or in a more localized form. Signs usually include anorexia, vomiting, diarrhoea, weight loss and pyrexia; several of which were present in this case. The main differential is IBD and often full thickness biopsies, sometimes using immunohistochemistry, are necessary to differentiate between the two.
Other possible techniques for distinguishing the two may include flow cytometry and assessment of T-cell clonality by PCR. Primary canine gastrointestinal lymphoma is usually of T-cell phenotype. Hypoprotein- aemia and hyperbilrubinaemia are more common in lymphoma than in IBD, but this is not consistent. It also appears that some cases of lymphocytic plasmacytic enteritis can eventually mutate into lymphoma.
There appears to be no age or sex predilection for the disorder. In one study, about half (23) of 44 dogs with gastrointestinal lymphoma were female, with 11 intact and 12 neutered: 21 of the dogs were male, with 12 intact and nine neutered. Sixteen breeds as well as individuals of mixed breeding were represented. The Boxer and the Chinese Shar-Pei were the most commonly represented breeds with six individuals each. The age range of the dogs was 1.5 to 14.6 years.
Treatment for focal lymphoma is usually by surgical resection, but this is not possible in the more generalized or diffuse form that this dog had. Dogs with this form respond poorly to chemotherapy and there is a risk of intestinal perforation. Chemotherapy with cyclophosphamide, vincristine and prednisolone (and sometimes doxorubricin) has been tried in dogs with diffuse alimentary lymphoma, but this form of lymphoma is more refractory to treatment than other forms in the dog. Response rates of 30% to 60% with a medium remission time of 4 to 8 months have been reported.
More on the topic 13 Pancreatitis and alimentary lymphoma in a dog:
- Chronic Pancreatitis
- Acute Pancreatitis
- 19 Pancreatitis in a cat
- LYMPHOMA
- Lymphoma
- Lymphoma and Lymphocytic Leukemia
- Primary CNS lymphoma (PCNSL)
- Lymphoma
- Hodgkin Lymphoma
- NON-HODGKIN'S LYMPHOMA
- Non-Hodgkin's Lymphoma
- Non-Hodgkin Lymphoma
- 38 Colorectal neoplasia in a dog
- 14 Hypoadrenocorticism in a dog
- 16 Ingestion of glue by a dog
- 33 Intestinal leiomyoma in a dog
- Hamster Polyoma Virus Infection: Transmissible Lymphoma