38 Colorectal neoplasia in a dog
Initial presentation
Haematochezia, diarrhoea and faecal tenesmus
Signalment: 2-year-old entire male German shepherd dog, body weight
29 kg
Case history
The dog had initially begun to have diarrhoea 4 months prior to presentation.
The diarrhoea had become progressively more haemorrhagic and increased in frequency and urgency to defecate. At presentation the dog strained to defecate almost continuously when taken on walks. He produced small amounts of soft to liquid faeces and large amounts of blood when defecating. The dog only rarely vomited. The owner said the dog had lost about 7 kg during the last 4 months.His current diet was a restricted protein dry diet, with no snacks or treats. The dog’s vaccinations were current and he had recently been treated with 50 mg/kg fenbendazole for 5 days.
He was on meloxicam for discomfort due to hip dysplasia. This had been stopped for a month 2 months earlier and there had been no resolution of clinical signs of diarrhoea or haematochezia. Other than the hip dysplasia, he had been a healthy dog until the onset of the diarrhoea.
Physical examination
The dog was bright, alert and responsive (Fig 38.1) although he was quite thin (body condition score 3/9) with muscle loss over the lumbar area (Fig 38.2). His mucous membranes were pink and moist with a capillary refill time of resolved within a week of initiation of this treatment and the haematochezia decreased with the chemotherapy.
At 1 month after diagnosis the dog was reported to have gained 1 kg in weight. There was no organomegaly present, although there was a persistent caudal abdominal lymphadenopathy. On digital rectal examination the previous mass could not be felt. The dog’s faeces were soft but formed and no blood was present. His status was described as partial remission. At 4 months after diagnosis the dog was doing very well and had gained another 3 kg in weight.
Discussion and epidemiology
Colorectal tumours are uncommon in dogs. The most common tumours in this location are adenomas or adenocarcinomas, which often have a more rounded appearance than this tumour (Fig 38.6) and are often found as a focal growth which does not metastasize. Adenomas and adenocarcinomas are most often tumours of older dogs. If not surgically
resectable, the clinical signs from adenomas and adenocarcinomas often improve with the use of NSAIDs, such as piroxicam given as rectal suppositories or per os.
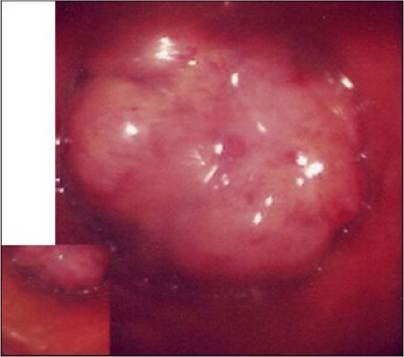
Fig 38.6
Endoscopic picture of a colonic adenoma
Alimentary lymphoma accounts for about 5% of cases of lymphoma and is often more difficult to diagnose than the more common multicentric form. In this dog, the presence of a colorectal lymphoma was not definitively proven, although he had lymph node involvement. This could either be a spread of the colorectal tumour or the dog may have had two diseases. In one study, the median age for GI lymphoma was about 8 years, with a spread of about 3 to 13 years, so this dog was a fairly young victim of the disease. Six of 30 dogs in that study had enlarged lymph nodes.
There appears to be no clear sex predilection for lymphoma, although some studies have shown more male than female dogs affected.
Prednisolone was used in this dog prior to the initiation of a chemotherapy protocol. Most oncologists have recommended against using glucocorticoids for treating dogs suspected of having lymphoma. If the lymphoma has not been diagnosed, the rapid Iymphocytolytic effects of glucocorticoids may have masked the diagnosis. Another reason for avoiding corticosteroid USC is the potential of multidrug resistance (MDR). MDR is a common cause for chemotherapeutic failure in canine lymphoma. It involves P-glycoprotein, a transmembrane protein which acts as an efflux pump for some chemotherapeutic agents, causing the drugs to be extruded from the tumour cells.
Other mechanisms of resistance to multiple agents have been discovered and MDR now refers to a phenotype of simultaneous resistance to chemotherapeutic agents which differ in structure and also includes the aptly named MDR associated protein (MRP). Many chemotherapeutic drugs are able to induce P- glycoprotein or MRP expression; however, the ability of dexamethasone to upregulate P-glycoprotein expression may be tissue and species dependent. There is still some suggestion that pre-treatment with glucocorticoids may adversely affect the success of treatment with a multidrug chemotherapy protocol; the answer is not definitive. In one study dogs pretreated with glucocorticoids had a significantly shorter remission (134 days) compared to those that did not receive glucocorticoids (267 days). However, in the present case, initial treatment with a more rigorous protocol may have resulted in excessive cytolysis and intestinal breakdown, so a more gradual approach was used.Prognosis
In one study the overall median survival time of dogs with GI lymphoma was 13 days; however, two dogs were alive at 31 and 84 months and both of these dogs had colonic or rectal neoplasia. Overall, alimentary lymphoma provides a fair prognosis for short to medium term remission, but a guarded prognosis for a long remission.
More on the topic 38 Colorectal neoplasia in a dog:
- Colorectal Cancer
- Neoplasia of the Ear Canals
- Mammary Neoplasia
- Pulmonary Neoplasia
- Hepatocellular Neoplasia
- Neoplasia of the Pinna
- Harderian Gland Neoplasia
- Neoplasia of the Reproductive System
- 14 Hypoadrenocorticism in a dog
- 16 Ingestion of glue by a dog
- 33 Intestinal leiomyoma in a dog
- 11 A foreign body in the small intestine of a dog
- Signature GEM Phenotypes: Molecular Pathology of Neoplasia
- 12 Chronic partial gastric dilatation in a dog
- 13 Pancreatitis and alimentary lymphoma in a dog
- 2 Idiopathic megaoesophagus in a dog
- 3 Myasthenia gravis in a dog
- Haemorrhagic gastroenteritis in a dog
- 25 Protein losing enteropathy in a dog
- 32 Colonic vascular ectasia in a dog