36 Feline constipation and megacolon
Case contributed by Nicki Reed
Initial presentation
Tenesmus, haematochezia and abdominal distension
Signalment: 8-year-old, female neutered Devon Rex cat, body weight 2.5 kg
Case history
The cat was presented for tenesmus, haematochezia and abdominal distension, accompanied by anorexia and lethargy.
Since being acquired 4 years earlier she had had intermittent episodes of constipation, manifested as straining to pass hard faeces which were occasionally coated with fresh blood or mucus. The episodes had initially occurred two or three times per year, but for the past 6 months had been occurring monthly. During these episodes the cat would defecate outside the litter tray and she appeared to have abdominal bloating. Symptomatic treatment with laxatives generally improved the condition within 1 to 2 days.Occasional episodes of small volume diarrhoea were reported (once to twice a year). At the time of presentation, she had passed no faeces for 4 days and had had a poor appetite for 2 days.
The cat was acquired from a rescue centre 4 years previously and lived indoors with one other unrelated Devon Rex cat. She was vaccinated against feline herpesvirus-1, calicivirus and feline parvovirus and de-wormed every 6 months with praziquantel and pyrantel. The cat was fed a proprietary canned cat food.
She was thought to have previously been used for breeding and was reported to have had surgery for an intussusception at 2 years of age.
Physical examination
The cat appeared slightly thin (body condition score 3/9) and had a distended abdomen (Fig 36.1). Her hydration appeared adequate and mucous membrane colour was pink with a capillary refill time of 2 seconds. Thoracic auscultation revealed a Grade I to II/VI systolic murmur, with point of maximal intensity at the left sternal border. No pulse deficits or arrhythmias were detected.
Respiratory rate was mildly increased at 30 breaths per minute, attributed to stress, as no abnormal lung sounds were detected. Abdominal palpation revealed a large colon, filled with hard faeces and a moderately distended bladder.Fig 36.1

Dorsal view of the cat showing distended abdomen.
Problem list and discussion of problems
The cat’s primary problem was thought to be constipation, based on the history and physical examination findings.
Differential diagnosis
Differential diagnoses for constipation include:
•Dietary causes, e.g. ingestion of bones or foreign material.
• Environmental causes, e.g. decreased exercise, litter box problems (dirty, change in type of litter or location of box; competition from other cats; inability to use the box due to arthritis or other locomotor disorders), stress
• Traumatic disorders, e.g. fractured pelvis; fractured or dislocated hip; bite wound; abscess; abdominal bruising; saccro-coccygeal luxation (tail-pull - unlikely as there was no history of trauma in this cat and the problem was chronic)
• Obstructive disorders, e.g. anal stricture; anal sac infection; rectal foreign body; rectal or colonic tumour; pelvic fracture malunion; perineal hernia; rectal diverticulum; pseudocoprostasis
• Neuromuscular disorders, e.g. spinal cord disease; congenital spinal cord anomaly (Manx cats); paraplegia/paralysis; central nervous system dysfunction; dysautonomia (Key-Gaskell syndrome); idiopathic megacolon
• Pharmacological causes, e.g. opioids; diuretics; anticholinergics; antihistamines; barium sulphate
With the chronic history and the lack of clinical signs consistent with most of the other possible differential diagnoses for constipation, the most likely cause in this cat was thought to be idiopathic megacolon, although other neurological causes and neoplasia could not be ruled out
Case work-up
A neurological examination was performed with no abnormalities detected.
A rectal examination showed no evidence of herniation, anal sac disease, strictures or foreign bodies. A few small pieces of hard dry faeces were present in the rectum.Minimum database
Routine haematology showed a moderate neutrophilia (26.2 ? 109∕l; reference range 2.5-12.8 ? 109∕l). This most likely represented a nonspecific inflammatory response. Serum chemistry parameters were within the reference ranges.
Imaging
Abdominal radiography showed impaction of the transverse and descending colon with faeces (Fig 36.2). In addition, ventral spondylopathy was present at the lumbosacral junction. Two views were taken to fully evaluate narrowing of the pelvic canal.
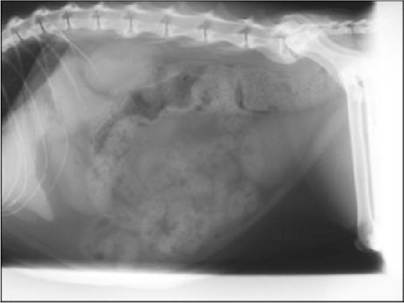
Fig 36.2
Lateral abdominal radiograph showing impaction of the transverse and descending colon with faeces at initial presentation.
Further investigations that could have been beneficial include urinalysis for assessment of hydration, ultrasonography if intraluminal or extraluminal masses were suspected, colonoscopy if intraluminal disease is suspected and barium enema if a stenotic lesion was suspected. If the neurological examination had been abnormal, further evaluation with MRI may have been useful.
Diagnosis
A diagnosis of colonic impaction was made. A diagnosis of obstipation could not initially be made, as it was not known whether the condition was refractory to therapy. Initial management was commenced with manual evacuation of faeces with the cat anaesthetized and a warm water enema was given.
Oral therapy with lactulose (initial dose 0.5 ml po q 8 hours) and cisapride (1.5 mg/kg po q 12 hours) was then started and the owner advised to feed a low residue diet. The clinical signs improved initially, although the frequency of defecation remained decreased, occurring only every second day.
Follow-up
Over the following 18 months the cat required increasing doses of lactulose and cisapride and micro-enemas with sodium alkylsulphoacetate on three occasions.
The cat subsequently presented after having not defecated for 4 days. She also again had a poor appetite and was lethargic. Further radiographs were obtained which showed a grossly dilated impacted colon (Fig 36.3) and as the condition was no longer responding to management a diagnosis of idiopathic megacolon was made.
Fig 36.3
Lateral abdominal radiograph showing a grossly dilated impacted colon at revisit.
Treatment options
The most appropriate treatment depended on the underlying cause of constipation and the severity of the problem. Potential therapy includes: • Ensure adequate hydration and correct electrolyte imbalance if present
• Evacuation of faeces (enemas)
• Dietary alteration and bulking agents
• Laxatives
• Prokinetics
• Surgery
Evacuation of faeces
When the cat was anaesthetized, an endotracheal tube was in position in case colonic manipulation induced vomiting. A combination of digital evacuation and enemas was typically used. Digital evacuation was performed gently, with copious lubrication. A warm water enema was used in this cat, although a variety of enema agents are available:
• Warm water or saline (5-10 ml/kg)
• Mineral oil, e.g. liquid paraffin (5-10 ml/cat)
• Lactulose (5-10 ml/cat)
• Sodium citrate + sodium alkylsulphoacetate
• Dioctyl sodium sulphate
Clinical tip on enemas in cats
Enema should be given slowly as rapid administration can induce vomiting. In addition, rapid administration reduces the ability to soften the stool and can increase the risk of colonic perforation. Enemas containing sodium phosphate should not be given to cats; they can cause hyperphosphataemia and an associated hypocalcaemia that may be fatal. Dioctyl sodium sulphate can increase the absorption of mineral oil therefore these two products should not be used together.
Dietary changes
Alterations in diet consist primarily of feeding increased fibre or low residue diets.
Bulking agents consist primarily of poorly digested celluloses and polysaccharides (insoluble fibre). The insoluble fibre draws water into the colon and stimulates colonic motility and thus defecation. Either proprietary high-fibre diets can be used or bulking agents such as sterculia may be added to the diet. Cats should be adequately hydrated before using bulking agents and this approach is only appropriate for mild cases. In cats with megacolon, increasing dietary fibre may be contraindicated, as the fibre is incapable of inducing colonic motility and may contribute to obstipation. Highly digestible/low residue diets are more appropriate in these circumstances as the faecal volume is reduced.Laxatives
Emollient
Emollient laxatives are detergents that improve the mixing of lipids (oils) with water. This improves the absorption of lipids from the colon, but decreases the absorption of water, hence softening the stool.
• Docusate plus dantron
Clinical experience with oral emollient laxatives is limited and efficacy not yet proven. Hepatotoxicity and carcinogenicity have been reported in people resulting in one of these products only being licensed for use in the terminally ill. Long-term use should therefore be avoided.
Lubricant
Lubricant laxatives reduce water absorption and facilitate passage of the faeces. Effects are generally mild, but they may be useful in mild cases of constipation.
• White paraffin
• Liquid paraffin (5-10 ml/cat per os)
Care should be taken if giving liquid paraffin orally, as it can be aspirated into the lungs. Chronic use of mineral oil laxatives can result in decreased absorption of fat-soluble vitamins.
Hyperosmotic
This group comprises sugars, magnesium salts and polyethylene glycol that, due to their concentrated nature, draw fluid into the lumen of the colon. The most commonly used is lactulose (0.5 ml/kg po q 8-12 hours), which also undergoes fermentation in the colon to produce organic acids.
The organic acids stimulate fluid secretion in the colon. The magnesium salts are less well tolerated in cats than they are in humans and should NOT be used in cats with renal failure (due to impaired magnesium excretion). Polyethylene glycol is used commonly in the human field; however, the large volume required with some products makes them unfeasible to administer to cats. Further, polyethylene glycol is contraindicated in cases of mechanical or functional bowel obstruction (i.e. most cases of feline megacolon) and there are some concerns that polyethylene glycol can cause renal failure, therefore this author would caution against its use.Stimulant
Stimulant laxatives cause secretion of fluid from the cells lining the colon and also stimulate the nerves that cause contraction of the smooth muscle. This latter effect may damage the nerves if used long-term, therefore continuous daily use is not recommended.
• Senna
• Castor oil
• Bisacodyl 5 mg po q 24 hours
Prokinetics
Prokinetic drugs act to improve the contractions of the bowel, thereby propelling digesta from the stomach to the rectum. Different areas of the gut have different receptors, therefore some prokinetic drugs are more effective in the stomach than the colon. Cisapride belongs to the group of drugs known as benzamide prokinetics and is particularly effective in the colon of cats because of its action on the 5HT4 receptors that are present there. Although it is not readily available in the United Kingdom, it may be imported under a Special Treatment Authorization (see Appendix 7). New drugs in this group (renzapride, prucalopride, mosapride) are being developed, as well as non-benzamide prokinetics (tegaserod). The latter was licensed in the USA, but has been recently withdrawn due to concerns about cardiac side effects and is therefore unlikely to be available to the veterinary market.
The H2 antagonists ranitidine and nizatidine have some prokinetic effect, although they are not as potent as cisapride. Their mode of action is via inhibition of acetylcholinesterase, resulting in accumulation of acetylcholine at the neuromuscular junction and potentiation of the action potential. Efficacy has been demonstrated in vitro, but not in vivo and related H2 antagonists cimetidine and famotidine do not share this prokinetic effect.
• Cisapride 0.1-1.0 mg/kg po q 8-12 hours
• Ranitidine 1.0-2.0 mg/kg po q 8-12 hours • Nizatidine 2.5-5.0 mg/kg po q 24 hours
Surgery
Although mild cases of constipation will respond to medical management, cases of obstipation usually require correction by means of surgery to remove the distended and nonfunctional colon. This procedure is known as a sub-total colectomy and may be performed with or without preservation of the ileo-caeco-colic valve (Fig 36.4). The advantages and disadvantages of each procedure are given in Table 36.1.
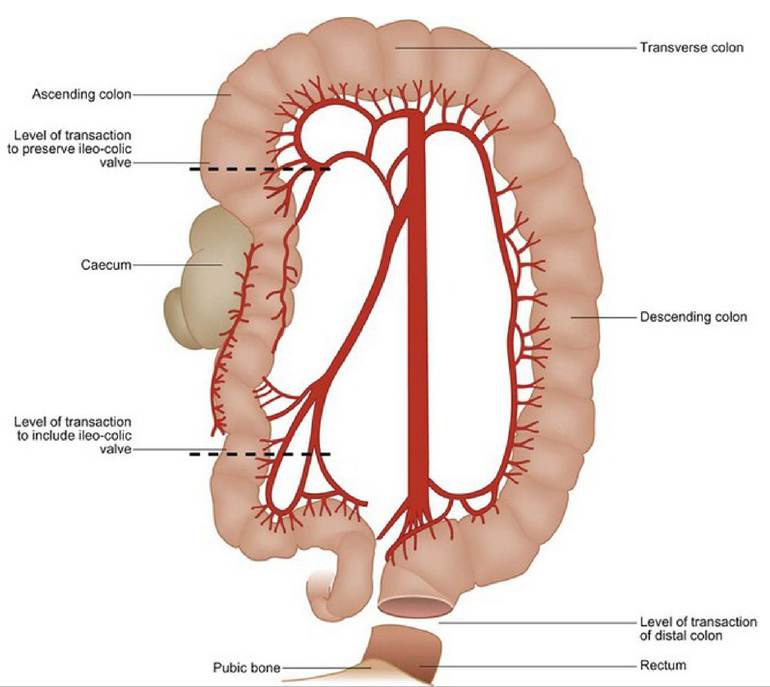
Fig 36.4
Illustration of the locations of the surgical options for colectomy.
Table 36.1 Advantages and disadvantages of sub-total colectomy
| Surgical procedure | bgcolor=white>AdvantagesDisadvantages | |
| Ileo-colic valve preserved | Reduced risk of colonic bacteria refluxing into small intestine and causing diarrhoea | May be recurrence of constipation in the segment of colon not removed. The bowel at the site of repair may be under greater tension |
| Ileo-colic valve removed | More colon is removed, therefore it is less likely to have recurrence of constipation Some surgeons feel it is an easier procedure to perform, as the area where the two ends of bowel are joined is under less tension | There may be a greater risk of small intestinal diarrhoea as a result of colonic bacteria migrating to the small intestine |
| Both procedures | The vast majority of cases have permanent resolution of constipation problems, thereby improving the cat’s quality of life and removing the necessity for permanent medication | Surgical: Anaesthetic risk Wound infections, breakdown Blood loss Peritonitis Postoperative: Recurrence of constipation Diarrhoea |
| Increased frequency of de- faecation |
Clinical TIP on constipation in cats
Owners of constipated cats may occasionally perceive the problem to be diarrhoea, rather than constipation. Faecal concretions within the colon are irritating to the mucosa causing secretion of fluid which can leak past the impacted faeces.
Nursing aspects
Standard enema pumps may be too wide bore to effectively introduce into a constipated cat. Use of a dog urinary catheter and syringe may facilitate introduction of enema solutions more proximally into the colon, enabling break-up of faecal material.
Many cats when hospitalized will become constipated. Reasons for this may include drugs (e.g. opioids), unfamiliar litter substrate (especially if normally outdoor cats), anxiety and lack of exercise. Trying a variety of litters, providing privacy and allowing the cats to exercise, particularly after feeding, may encourage defaecation.
Lack of water intake may be a feature in a number of cats that become constipated and cats are often reported to drink little at home. Reasons for this may be the water bowl is beside the food bowl, the bowl is an inappropriate size, the cat cannot see the water level or the cat prefers running water. Moving the water bowl away from the food bowl and trying larger bowls of a different substance may encourage drinking, as can use of a water fountain.
Follow-up
With a diagnosis of idiopathic megacolon no longer responsive to medical management the cat underwent surgery for a sub-total colectomy. Histopathological findings were consistent with idiopathic megacolon. Following surgery her demeanour and appetite improved, although she had a tendency to pass diarrhoeic faeces. The cat has remained well for 6 years post-surgery and has been maintained on a highly digestible diet.
Pathophysiology
The colon has two main functions: absorption of water and electrolytes and storage of faeces. The wall of the colon is made up of two types of smooth muscle: the concentric circular muscle on the luminal aspect and the longitudinal muscle on the serosal aspect. The muscular layers receive stimulation from the intrinsic nerves whose cell bodies lie in the submucosal (Auerbach’s) and myenteric plexuses (Fig 36.5). These nerves cause ‘slow-wave’ contractions that occur at a rate of approximately five per minute. The contractions are initiated by a ‘pacemaker’ located at the junction of the transverse and descending colon. The slow wave contractions mix the digesta. When the colon becomes distended with digesta more coordinated contractions (segmentation and peristalsis) are initiated, which pushes the digesta aborally towards the rectum. Here, defecation is controlled by the extrinsic nerve supply from the pelvic and pudendal nerves (Fig 36.6). The extrinsic nerve supply can also have an effect on segmentation, either stimulating it (parasympathetic) or inhibiting it (sympathetic - adrenergic).
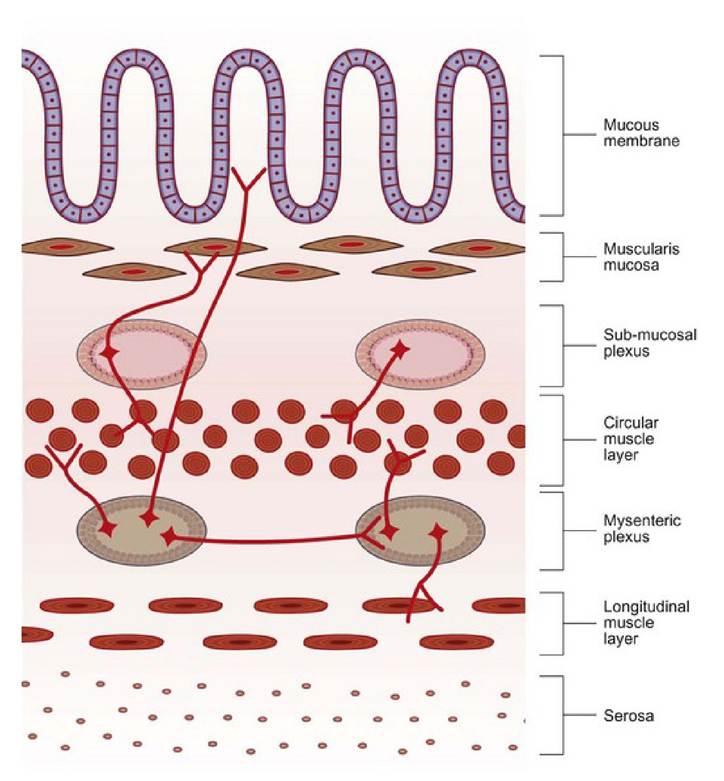
Illustration of the muscular layers of the colonic
Fig 36.5
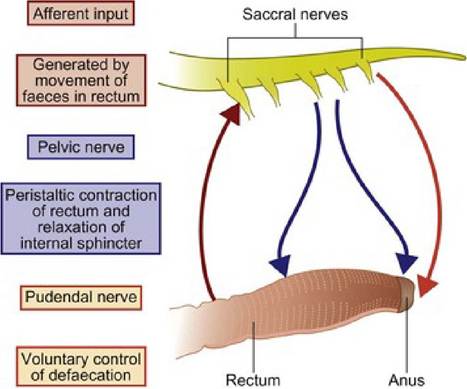
Fig 36.6
Illustration of the nerve supply to the colon.
The cause of megacolon is not well understood. It is typically recognized in middle-aged to older cats, with a history of progressively worsening constipation. Proposed mechanisms have included abnormalities with the nervous supply to the lower colon (intrinsic or extrinsic), an abnormal neuromuscular junction or abnormal smooth muscle. No anatomical abnormalities have been demonstrated with histopathological examination, but the contractile ability of the smooth muscle has been shown to be altered. It is not known whether this altered contractility is the cause of megacolon or simply an effect of prolonged stretch.
Two forms of megacolon are described - dilated and hypertrophic. Idiopathic megacolon is a dilated form of megacolon, with permanent loss of function. Hypertrophic megacolon may arise when the colon dilates proximal to an obstruction (e.g. fractured pelvis) and may be reversible if the obstruction is relieved in sufficient time (and compression of the thorax of both were normal. Abdominal palpation was mostly unremarkable, although their colons felt fluid filled. There was inflammation of the perianal area of one kitten. The rectal temperatures, heart rates and respiratory rates were within normal limits and the pulse quality was good in both kittens.
Problem list and discussion of problems
• Diarrhoea of large intestinal origin
Differential diagnosis
Differential diagnoses for chronic large intestinal diarrhoea in these kittens included:
• Inflammatory diseases
• chronic colitis
• inflammatory bowel disease
• infectious colitis, e.g. Salmonella spp., Campylobacter spp., Clostridium perfringens
• parasites, e.g. Tritrichomonasfoetus, Giardia, Cryptosporidium, cocci- dia
• Dietary
• food poisoning
• dietary intolerance or allergy
• Toxins, including toxic plants
• Congenital malformations
• Small intestinal malabsorption and the production of secretagogues such as unconjugated bile acids and hydroxylated fatty acids
• Other causes such as obstruction, ischaemia or neoplasia were less likely to involve two kittens. Infections and environmental (diet, toxin) factors were the most likely causes of the diarrhoea.
Case work-up
Minimum data base
Haematology and serum chemistry were performed and the results were unremarkable. Serum feline trypsin like immunoreactivity (TLI), cobalamin and folate were within the reference ranges, consistent with the presumed large intestinal origin of the diarrhoea. Screening tests for FeLV and FIV were negative. Routine urinalysis was unremarkable in both kittens.
Imaging
Abdominal ultrasound showed mildly enlarged mesenteric lymph nodes but no other abnormalities. Intestinal wall layering and thickness were within normal limits.
Faecal tests
Faecal flotation (performed on three samples) showed no parasitic ova and faecal culture for enteropathogens was negative. Zinc sulphate centrifugation-flotation preparations were negative for Giardia and Cryptosporidium.
A fresh faecal smear was collected by inserting a swab into the anus of each of the kittens. The faeces and mucus obtained was diluted with an equal volume of normal saline and examined under the microscope. Large numbers of motile spindle shaped trophozoites were observed (Fig 37.1), which had flagellae and moved with a jerky movement. This appearance is typical of Tritrichomonas foetus. To confirm the infection, a sample of faeces from each kitten was submitted for T. foetus polymerase chain reaction (PCR), which was positive in both kittens.
Fig 37.1
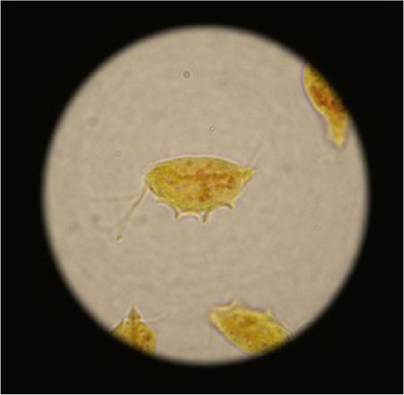
Microphotograph of Tritrichomonas foetus
(courtesy of Dr Andy Sparkes)
Treatment and outcome
The kittens were treated with ronidazole at 30 mg/kg q 12 hours po for 14 days. Both kittens improved on the treatment. Their diarrhoea completely resolved and they showed no adverse side effects from the treatment.
Discussion and epidemiology
T. foetus is a flagellated protozoan parasite that causes large bowel diarrhoea in infected cats. Clinical signs vary among cats, but often include increased frequency of defecation, passing of semi-formed to liquid diarrhoea often described as foul-smelling and containing mucus and blood, and flatulence. The anus may become inflamed due to the severe diarrhoea, as happened in one of these kittens. Affected cats are usually well otherwise and do not usually show significant weight loss.
The protozoal induced diarrhoea appears to be more common in younger cats (often less than a year of age), cats from households containing pedigree cats or other multi-cat households and young cats from rescue centres. It has been reported that the Siamese and Bengal breeds of cats may have an increased risk and purebred cats in general seem to be over-represented. It may be that genetic factors increase the risk in these cats, although the high density management likely increases the risk of infection.
Cats shed the organism in their faeces and infection is thought to be faecal-oral. The distribution of the organism is not completely understood yet, but it has been reported in the USA, UK and Germany and there are indications that it is also present in other European countries, China and South America.
Fresh faecal smears diluted with saline may be examined microscopically for the presence of typical motile trophozoites. If any mucus has been passed with the faeces this should be included in the smear as it is the most likely place to find the organisms. A cover slip should be pressed over the smear and then the slide can be examined under ?200 and ?400 magnification.
In most clinically affected cats, large numbers of organisms can be seen. They have short tails and an undulating membrane that runs over the length of the body. They are described as having a jerky, forward motion. Examination of multiple smears and multiple faecal samples will improve the rate of detection of the organism. Rectal swabs, as used in this case, can also be examined for the organism. A cotton swab is inserted into the anus and rotated over the colonic mucosa. It is then withdrawn and a smear made on a microscope slide which is again diluted with saline and examined. The organism should to be distinguished from Giardia. With Giardia infection the trophozoites tend to be far fewer in number, they are binucleate with a concave ventral sucker, sometimes described as a ‘monkey face’. Giardia do not exhibit the same forward motion as T. foetus. If a cat has had recent antibiotic therapy, the number of T. foetus trophozoites shed may be decreased which can make the diagnosis more difficult. In such cases, more sensitive diagnostic techniques may be preferable.
Two other diagnostic tests are available which are both more sensitive and specific for this organism than examination of fresh faeces. The first test is PCR (polymerase chain reaction) which can detect the presence of the genetic material of the organism. This is a highly sensitive test. In the USA, samples can be submitted to the College of Veterinary Medicine, North Caroline State University for this test. Information on this is available in Appendix 6. The PCR test is available in the UK from Capital Diagnostics in Edinburgh (phone 0131 535 3145). See Appendix 6 for further information about testing for T. foetus.
Treatment
Treatment with ronidazole at 30 to 50 mg/kg has been shown to resolve the diarrhoea and eradicate infection (on the basis of the PCR test). However, ronidazole is not licensed for use in cats and although it appears to be relatively safe from limited studies, it should be used with caution and only with informed and signed owner consent. Neurotoxic side effects have been reported with ronidazole, including agitation, facial tremors and trembling, seizures, ataxia and anorexia. In two reported cases, the signs stopped when the drug was withdrawn. Metronidazole has also been used, but has shown poor efficacy. Tinidazole has been trialled as it is thought to possibly have less risk of neurotoxicosis compared to ronidazole. While tinidazole decreased the detection and shedding of T. foetus, it appeared to be less efficacious than ronidazole.
Prognosis
The clinical prognosis for most infected cats is good, although many owners report subsequent infrequent and short-duration relapses of diarrhoea. It is not known if these relapses correspond with faecal shedding of T. foetus. As the diarrhoea does resolve over time and is often more of an inconvenience than being associated with significant adverse effects in affected cats, it may not be necessary or advisable to treat all affected cats with ronidazole. Using a simple, highly digestible diet frequently results in improved faecal consistency and this alone may allow sufficient control of clinical signs in some cats.
More on the topic 36 Feline constipation and megacolon:
- CONSTIPATION
- Constipation
- Feline Polyps
- FELINE INFECTIOUS PERITONITIS
- 8 Feline dysautonomia
- FELINE PANLEUCOPENIA
- 28 Feline exocrine pancreatic insufficiency
- Medications used in the treatment of feline hepatic lipidosis
- Index
- Case study contributors
- MAIN RETROVIRUSES OF WILD MAMMALS
- PERIANAL DISORDERS
- canine Parvoviral enteritis
- Toxin-Mediated Infections Clostridioides difficile Infection
- HIRSCHSPRUNG’S DISEASE
- SHIGELLOSIS
- Infantile Botulism
- Oncologic Emergencies