28 Feline exocrine pancreatic insufficiency
Case contributed by Nicki Reed
Initial presentation
Weight loss, diarrhoea, Steatorrhoea and vomiting
Signalment: 7-year-old, male neutered domestic shorthaired cat, body weight 3.33 kg
Case history
This cat presented for investigation of weight loss, diarrhoea, steator- rhoea and vomiting, which were accompanied by a good appetite.
The cat had been acquired 5 years previously and lived indoors. He had received core vaccinations and regular boosters, but no endo- or ectoparasiticides. His episodes of diarrhoea had occurred since acquisition. The diarrhoea was usually semi-formed and brown and would usually resolve without treatment after 2 to 3 days. The episodes occurred approximately six to eight times per year. The nature of the diarrhoea had changed approximately 3 months prior to presentation. The faeces were described as voluminous, greasy and malodorous and had also previously been white in colour. During defecation the cat did not strain and there was no blood or mucus in the faeces.
Occasional episodes of vomiting (one to three times per year) were also reported. The vomitus generally comprised semi-digested food. In the 3
months prior to presentation the cat’s appetite had increased. He was eating a 450 g tin of commercial canned cat food and approximately 50 g of dried biscuits per day.
The cat had always been overweight (previously 6 kg) but there had been a steady weight loss since his last vaccination 8 months previously.
Physical examination
The cat was in poor body condition (body condition score 2/9), but otherwise bright and well. His coat was greasy, matted and unkempt. On abdominal palpation the intestines felt fluid filled, but the cat did not appear uncomfortable during palpation. Thoracic auscultation was unremarkable. His heart rate was 160 beats per minute with matched good quality pulses, respiratory rate 28 breaths per minute and rectal temperature 37.9° C.
There was faecal soiling around the perineum.Problem list and discussion of problems
The primary problems were weight loss and diarrhoea, but the presence of a good appetite helped to narrow the differential diagnoses list and the vomiting and weight loss were thought to be related to the diarrhoea in this case. The clinical signs were consistent with diarrhoea due to small intestinal disease.
Differential diagnosis
Differential diagnoses for diarrhoea in this cat include:
• Maldigestion
• exocrine pancreatic insufficiency (EPI)
• Malabsorption
• inflammatory bowel disease (lymphocytic-plasmacytic, eosinophilic, granulomatous)
• lymphoma
• Metabolic disorders
• hyperthyroidism
• diabetes mellitus
• Gastrointestinal parasites
• Pancreatitis
• Lymphocytic cholangitis
The presence of steatorrhoeic, malodorous faeces suggested a maldigestion problem was most likely.
Case work-up
Routine haematology, serum biochemistry and urinalysis were performed as a minimum data base. Total thyroxine was also measured to screen for hyperthyroidism. Results were all within the reference range, with the exception of alanine aminotransferase (ALT), which was markedly elevated at 865 IU∕l (reference range 20-75 IU∕l) and alkaline phosphatase which was elevated at 124 IU∕l (reference range 20-80 IU/ l). Faecal analysis for parasites was repeated and was again found to be negative.
More specific investigations for the gastrointestinal tract were performed. Feline pancreatic lipase immunoreactivity (fPLI) and feline trypsin-like immunoreactivity (fTLI) were performed to assess pancreatic function. Folate and cobalamin were measured to assess for malabsorption of these vitamins. Folate and fPLI were both within their reference range. Cobalamin was low at 99 ng/l (reference range 290-1499 ng∕l) and fTLI was also low at 9.2 μg∕l (reference range 12.0-82.0 μg∕l).
Abdominal ultrasonography was performed, primarily to evaluate the liver and pancreas.
The liver appeared grossly normal and although the pancreas was identified, it appeared small. In light of the raised liver enzymes, a liver biopsy was felt to be useful; however, prior to this being performed an assessment was made of clotting times. Whilst the activated partial thromboplastin time (APTT) was normal, the prothrombin time (PT) was prolonged at 27.7 seconds (reference range 7.0-12.0 seconds). The liver biopsy was thus deferred.Diagnosis
The history, clinical examination findings and the sub-normal fTLI were supportive of a diagnosis of EPI. Cobalamin deficiency is frequently reported in association with EPI in cats and prolongation of the PT is attributed to Vitamin K deficiency.
Treatment options
Pancreatic enzyme replacement
A number of commercial pancreatic enzyme replacement products are available in powder or capsule form. Supplementation should be in a non enteric-coated formulation, as enteric coating has been shown to reduce the amount of available enzyme in the duodenum. The amount administered should relate to the amount of food fed, rather than the body weight of the animal and should be provided with each meal fed. Palatability appears to be more problematic with cats than with dogs.
This cat was given two capsules of a powdered pancreatic supplement opened and sprinkled on each meal of canned food and he was willing to eat the supplemented food.
A number of cats have refused to eat food containing enzyme replacement powder, despite the ravenous appetite induced by the condition. Fresh frozen pancreas is an alternative if it can be sourced. Bovine pancreas is not covered by the Specified Bovine Offal Order of 1995 and therefore may be used. Pig pancreas may be more appropriate in the United Kingdom where bovine prion disease could be a concern for owners. In countries where Aujesky’s disease is present bovine pancreas is more appropriate. Informed written consent should be obtained from owners, as the risk of contracting food poisoning organisms such as Salmonella, Escherichia coli and Toxoplasma gondii remains, although freezing greatly reduces the risk.
Approximately 30 to 40 g of pancreas should be mixed with each meal. Although no published data exist regarding the duration of efficacy following freezing, in the author’s experience, pancreas that has been frozen for up to 8 months still appears to retain its enzymatic function.Cobalamin
Replacement of pancreatic enzymes does not address the lack of intrinsic factor (see Clinical Tip in Ch 5). Cobalamin replacement is therefore required on a permanent basis and as the lack of intrinsic factor prevents absorption from the ileum this must be replaced parenterally. Variable doses have been reported. This cat was given 250 μg subcutaneously weekly for 6 weeks. His serum cobalamin concentration was still low at 179 μg∕l, so the dose was increased to 500 μg subcutaneously weekly. His serum cobalamin concentration was within the reference range at the next revisit 1 month later, so the frequency of the injections was decreased to monthly. Many owners can be taught to do these injections at home, in the same way diabetic owners will administer insulin.
Folate
Cobalamin deficiency can affect the intestinal villi, leading to malabsorption, which may cause folate deficiency. Folate levels should therefore be assessed and supplemented orally if found to be low (400 μg/ day), although in this cat they were within the reference range at diagnosis.
Vitamin K
If a prolonged PT (and/or APTT) is identified, as in this cat, where the PT was prolonged, then supplementation of vitamin Ki may be required in the short term to prevent potential bleeding problems. Vitamin Ki was administered subcutaneously using a fine gauge needle to minimize the risk of haematoma formation, at a dose of 2.5 mg/kg. Oral supplementation was not initially used at it may be less satisfactory because absorption may be compromised from lipase deficiency. The prolonged PT was within the reference range within 24 hours. As in most cases, once enzyme replacement is instituted enteric Vitamin K absorption was satisfactory.
Diet
If the above management strategies had not been fully effective, then consideration would have been given to dietary manipulation. Whilst use of a low fat diet has been proposed, there is little evidence to support that this is necessary. Inflammatory bowel disease is often associated with pancreatitis. This may arise from bacteria being forced up the pancreatic duct from the duodenum when cats vomit or from lymphocytic plasmacytic infiltrate of the pancreas in association with lymphocytic plasmacytic infiltrate of the intestine (and liver). The combination of pancreatitis, inflammatory bowel disease and hepatopathy is sometimes termed triaditis. Cats with EPI may therefore benefit from management of inflammatory bowel disease with a hypoallergenic diet or novel protein diet.
Discussion
EPI is a functional disorder of the pancreas, whereby inadequate production of digestive enzymes results in signs of maldigestion. The primary digestive enzymes involved are trypsin for the digestion of proteins, amylase for the digestion of carbohydrates and lipase for the digestion of fats. Deficiency of these enzymes gives rise to maldigestion of food, production of voluminous fatty stools and subsequent weight loss.
In dogs the condition is most frequently caused by selective atrophy of the acinar glands responsible for the production of digestive enzymes. It is proposed that in some breeds this may be the result of immune-me- diated destruction. In cats, EPI is attributed to destruction from chronic pancreatitis and the history of this case is suggestive of bouts of pancreatitis (with likely concurrent cholangitis).
Lipase deficiency in EPI prevents the breakdown of dietary triglycerides into monoglycerides and fatty acids, resulting in the production of steatorrhoea. It is the rancid fat in the faeces that gives rise to their malodorous nature. In addition, absorption of fat-soluble vitamins (A, D, E and K) may be compromised. Vitamin K is necessary for the synthesis of clotting factors II, VII, IX and X.
Of these, factor VII has the shortest half-life, therefore the extrinsic clotting cascade, as measured by the PT, is affected before the intrinsic clotting cascade, as measured by the APTT (Fig 28.1).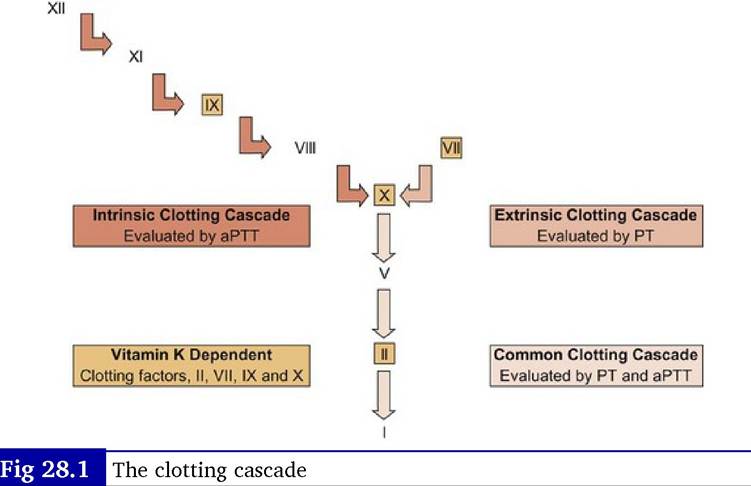
Cobalamin absorption requires intrinsic factor. In dogs, intrinsic factor is produced partially by the stomach, whereas in cats it is produced exclusively by the pancreas. In addition to deficiency of digestive enzymes, cats with EPI are also deficient in intrinsic factor, which in turn leads to an inability to absorb adequate cobalamin. Cobalamin deficiency may be found in association with canine EPI, and may be worth checking in poorly responsive patients, as deficiency of cobalamin can lead to villous atrophy and malabsorption.
Epidemiology
The incidence of EPI is much rarer in cats than dogs. The condition is common in German shepherd dogs and Rough collies, but may be underrecognized in cats. One study gave an incidence of only 11 cases out of 180,648 submissions (0.006%), although this was a post-mortem based study. The majority of cats with EPI are middle aged to older, which refleets the underlying pathogenesis of chronic pancreatitis. No breed or sex predisposition has been identified.
Prognosis
Although this is a lifelong condition, the prognosis for control is usually reasonable, provided the cat tolerates the enzyme replacement. Typical of many cats, this cat responded rapidly to treatment (Fig 28.2). Owners should be advised of the potential for the cat to develop diabetes mel- litus as both conditions share the same aetiology, i.e. recurrent/chron- ic pancreatitis. Diabetes mellitus would appear to be the more common outcome with chronic pancreatitis and whilst it is possible for the cat to develop both conditions, this rarely appears to happen. The reason why some cats appear to have damage to the exocrine pancreas more than the endocrine pancreas is not known.

Fig 28.2
The cat after 6 weeks of treatment showing weight gain and improvement in coat condition
Nursing aspects
Cats with EPI develop a greasy coat as a result of fat malabsorption and cobalamin deficiency. In addition, their coats may become soiled with faecal matter, particularly if longhaired. Bathing with an anti-seborrhoeic shampoo may be beneficial until clinical signs are controlled.
Clinical tips on treatment of feline EPI
• Regular monitoring of cobalamin and folate levels with appropriate supplementation is recommended. Measurement of cobalamin by competitive chemiluminescent enzyme immunoassay appears to be more reliable than measurement by radioimmunoassay, therefore checking which method the laboratory uses may be worthwhile.
• If pig pancreas can be sourced, then approximately one-third of a pig pancreas is an appropriate portion per meal. Wrapping each pancreas in cling film prior to freezing means an individual pancreas can be removed from the freezer for defrosting each day.
• Feline TLI can be increased by renal disease or feeding, therefore this should be borne in mind if a low normal value is obtained in a cat with typical clinical signs. Re-evaluation of a fasted sample should be performed if there is strong clinical suspicion. Values dry puppy food.
Physical examination
On presentation the puppy was extremely depressed. He had a body condition score of 4/9. His mucous membranes were slightly dry and pale pink, with a capillary refill time of 3 seconds. A skin tent was present. He was drooling, which was thought likely to be due to nausea. His heart rate was 90 beats per minute with somewhat weak peripheral pulses. Respiratory rate was 40 breaths per minute and rectal temperature was 39.6° C. There were bloody faeces present on the thermometer.
Problem list discussion of problems
The puppy’s main problems were acute haemorrhagic diarrhoea and vomiting. While there was some fresh blood present in the faeces, the diarrhoea was thought to be primarily small intestinal in origin. The vomiting and diarrhoea were combined for the differential lists in this puppy as the concurrent onset suggested a single disorder.
Differential diagnosis
Potential causes of acute vomiting and haemorrhagic diarrhoea in this puppy included:
• Parvovirus infection
• Intussusception or intestinal volvulus
• Hookworms
• Caustic agents
• Medications (e.g. corticosteroids, NSAIDs)
• Haemorrhagic gastroenteritis
• Severe acute pancreatitis
• Neoplasia and exocrine pancreatic insufficiency are unlikely due to his young age
Clinical tip on haemorrhagic diarrhoea
Haemorrhagic diarrhoea has a characteristic odour - once smelled, not easily forgotten. This odour is associated with other causes of haemorrhagic diarrhoea and is not specific for parvovirus enteritis
Case work-up
Emergency diagnostic tests and treatment
The puppy was admitted for diagnostic tests and treatment and was housed in an isolation unit to prevent spread of a possibly contagious disease to other animals.
Nursing tip for infectious diseases
With cases of possibly infectious disease, patients should be kept in an area separate from other patients, especially those patients that may be immunocompromised (e.g. on corticosteroids or chemotherapeutic agents, elderly or young patients). Gloves and protective clothing should be worn to handle the patient and the same materials should not be worn when handling other patients. Scrupulous washing of hands and a dip bath or covers for shoes should also be used. When possible, different staff members should handle a potentially infected case than those handling other patients, especially immunocompromised patients. A thermometer should be kept for use in the potentially infected patient only and a cover used on the thermometer. Stethoscopes and any other equipment used should be cleaned after use or kept only for that patient.
Parvovirus may survive outside the host and is resistant to many disinfectants. For parvovirus, kennel cleaning should be done with bleach at 1 : 32 dilution (half cup bleach per gallon water). Also note that hand sanitizers are probably not viricidal since they are alcohol-based.
The puppy was estimated to be approximately 8% dehydrated. A balanced intravenous crystalloid fluid therapy (lactated Ringers) was initiated at 116 ml/hour.
Clinical tip
Calculation of intravenous fluid amounts
Fluid therapy is calculated based on the amounts needed for maintenance, rehydration and to replace ongoing losses. Maintenance requirements are 40 to 60 ml/kg/24 hour. In this puppy, they were calculated as: 20 kg ? 60 ml/ kg = 1200 ml/24 hour or 50 ml/hour. The upper end of the maintenance requirement was used in this dog as he was a puppy and they have a larger percentage of body weight as fluid compared to increased body fat in adult animals. Usually the lower end is used for large breed dogs.
To correct his hydration over 24 hours, his body weight times his percent dehydration was used: 20 kg ? 0.08% = 1.6 l (1600 ml)/24 hours or 66 ml/ hour. This was added to the maintenance amount so that the initial fluid rate was 116 ml/hour. The dehydration could also have been corrected in a shorter time period, e.g. 10 to 12 hours with a faster fluid rate (210 ml/hour for 10 hours or 183 ml/hour for 12 hours).
Estimates of the amount of fluid lost in vomiting or diarrhoea may be added to the maintenance plus rehydration rates. The hydration status should be reevaluated frequently (hourly while on the fast rates) to determine if the rate should be changed and to assess for overhydration.
Clinical tip
Choice of fluids
For rehydration a crystalloid fluid containing some electrolytes is usually appropriate. With dehydration due to diarrhoea and most cases of vomiting (other than those caused by upper gastrointestinal tract obstruction), the patient is in a state of metabolic acidosis due to decreased tissue perfusion. Buffered crystalloid intravenous solutions such as lactated Ringers are more alkalinizing than 0.9% sodium chloride and may help correct the acidosis, although reperfusion of the tissues is the most crucial part of the treatment.
Emergency minimum data base
Haematology showed a marked neutropenia of 0.06 ? 109/l (reference range 3.0-12.0), a lymphopenia of 0.4 ? 109∕l (reference range 0.5-4.99). His packed cell volume (PCV) was 0.322 l∕l, at the bottom end of the reference range used (0.32-0.55 l∕l); however, he was dehydrated so the true value of his PCV would likely have been lower upon rehydration. Haemorrhagic diarrhoea can result in a rapid decrease in PCV.
An in-house electrolyte analysis showed a decreased serum potassium concentration of 2.9 mmol/l, reference ranges 3.6-5.6 mmol/l, with the serum sodium and chloride within the reference ranges. A decreased serum potassium concentration is common in gastrointestinal disorders and can result in further gastrointestinal ileus. Treatment was potassium chloride added at 15 mEquiv/l of fluid.
Clinical tip on potassium supplementation
For maintenance fluids, the rates of potassium supplementation based on serum concentrations are:
| Serum concentration | mEquiv KCl to add per litre |
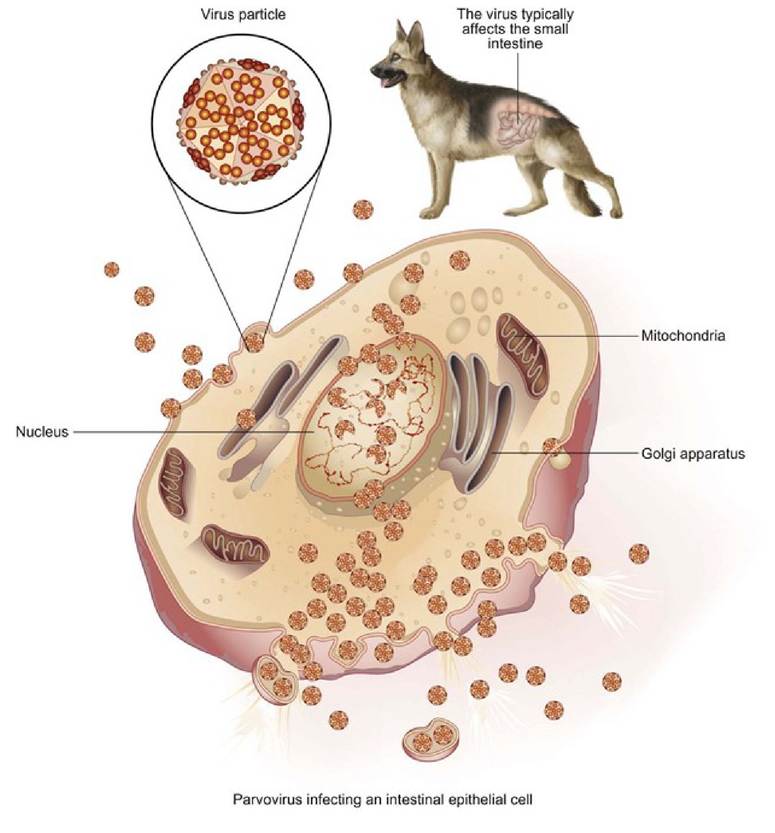
| is used for severe vomiting, a constant rate infusion is better than SQ administration as the half-life is not long enough for consistent efficacy. Metoclopramide and ranitidine both have promotility effects, which were important in this case as ileus was present. Nursing tip Intravenous catheters should be well bandaged to keep them clean, especially in cases with vomiting and diarrhoea. They should be checked and flushed several times a day for patency. Catheter infections are a common cause of pyrexia so good hygiene is imperative. A rise in rectal temperature in patients with intravenous catheters is often associated with inflammation at the catheter site. A faecal SNAP™ Parvo test was performed and was positive. As the signalment and clinical signs were also consistent in this puppy, a diagnosis of parvovirus gastroenteritis was made. Clinical tip on parvovirus testing The ELISA faecal SNAP™ Parvo test is the most common in house test for parvovirus. The test does have some limitations. Recent vaccination with a live vaccine may interfere with the test results causing false positive readings. This interference usually occurs 5 to 12 days after vaccination so if a positive faecal ELISA SNAP™ test is obtained within this period after vaccination, additional tests may be recommended. The test is highly sensitive (100%) and specific (99.9%). The puppy was a bit brighter the following day, but still had diarrhoea containing blood and was vomiting. A full haematology and serum chemistry was performed at a veterinary laboratory. Haematology showed a decreased PCV of 0.30 l/l (reference range 0.35-0.55 l/l). White blood cell counts had improved, but were still decreased with a neutrophil count of 2.1 ? 109∕l (reference range 3-12 ? 109∕l) and a lymphocyte count of 0.47 ? 109∕l (reference range 0.7-4.8 ? 109∕l). The puppy’s ALP was increased to 422 IU∕l. The reference range for ALP for this laboratory is 20 to 60 IU∕l for adult dogs. In 6-month-old puppies the value can be expected to be increased, but usually in the range of two to three times the adult range (i.e. probably not much greater than 180 IU∕l). Gastrointestinal disease can also increase ALP, so there was likely an increase due to illness in this puppy. Serum phosphorus was also increased to 2.4 mmol∕l, with the adult canine reference range for this laboratory being 0.4 to 2.0 mmol∕l. He was, however, within the reference range for a growing puppy at 6 months of age, which is about 1.65 to 2.84 mmol∕l. Serum glucose was within the reference range at 5.0 mmol∕l (reference range 3.0-5.0 mmol∕l). Clinical tip on haematology and serum chemistry in puppies and kittens The reference ranges for several Clinicopathological parameters are different in young growing animals compared to adults and most laboratory reference ranges are those for adults. See Appendix 5 for a table of some juvenile blood values. Serum potassium increased to 4.4 mmol/l (reference range 3.6-5.6 mmol/l) after supplementation and all other electrolytes were also within the reference ranges. Serum albumin concentration was decreased at 17.6 g/l (reference range 26-35 g/l) as was the globulin concentration of 17.5 g/l (18-37 g/l). Serum albumin is decreased in young puppies, but by the age of 4 months should be within adult reference ranges. The decrease in this puppy is likely due to intestinal loses. Outcome and further treatment The puppy gradually improved over the next several days. He was first offered ice cubes to lick and then small amounts of water. By the fourth day he was eating small amounts of cooked chicken. An oral balanced electrolyte solution containing glutamate was also given to him in small amounts by syringe. Over the next few days his lymphocyte and neutrophil counts improved and serum albumin and globulins increased. Nursing tip on nutrition of vomiting patient If a patient that has been vomiting is offered water or food too soon, they may start vomiting again. After 12 to 24 hours of no vomiting, allowing them to lick ice cubes is a good way to gently start them back on oral intake, as they can only swallow very small amounts at a time. Use of oral fluids that contain glutamate may provide some nutrition for the cells lining the intestinal tract, which have usually been depleted during severe diarrhoea. The first foods offered need to be highly digestible and low in fat, as the intestinal tract needs some time to adjust and re-develop digestive enzymes. Some puppies that have had parvovirus may require a highly digestible diet for months or even for the rest of their lives. Partial parenteral nutrition has been used successfully in puppies with parvovirus and provides good short-term nutritional support. This may be administered through a peripheral vein and can be utilized in a practice setting. It has been shown that early enteral nutrition in dogs with parvovirus results in an earlier clinical improvement and possibly an improved gut barrier function. Some people have recommended enteral feeding by naso-oesophageal tube, but this should be well monitored to make sure the dog does not vomit the tube and cause feeding in to the trachea. Recombinant feline interferon (type omega) has also been recommended for use in dogs with parvovirus and one study showed an improvement in clinical signs and decreased mortality rates when this was administered at 2.5 million units/kg intravenously once a day for 3 days. The puppy was sent home after 5 days in hospital. He continued to have diarrhoea for about another week, although the vomiting stopped and he was eating well. Discussion and epidemiology Canine parvovirus is widespread in the dog population and most dogs are exposed to the virus either by vaccination or from contact with other dogs or dog faeces. The virus can survive for about 5 to 7 months in faeces and contact with infected faeces is the most common route of infection. The incubation time is 3 to 8 days and shedding of the virus may occur prior to the onset of clinical signs. Following ingestion of the virus, it replicates in the lymphoid tissue of the oropharynx and then spreads to the bloodstream. The virus is deposited in the rapidly dividing cells of the body, including the bone marrow and the epithelial cells of the intestinal tract. The replication of virus in the lymphopoietic system and bone marrow results in the lymphopenia and neutrophilia usually seen. The presence of the replicating virus in the intestinal cells (Fig 29.1) causes depletion of the intestinal villi and epithelial necrosis, resulting in the typical severe haemorrhagic diarrhoea. Intestinal bacteria such as Clostridium perfringens and Escherichia coli may translocate across the compromised intestine into the body and can cause sepsis and death.
Fig 29.1 Illustration of parvovirus infecting an epithelial cell. Rottweilers, Labrador retrievers and Doberman pinschers appear to be predisposed to the infection. Most cases occur in dogs less than 1 year of age and most often in dogs from 6 to 18 weeks of age. While this dog had been vaccinated, vaccine ‘breaks’ (disease in the face of vaccination) can occur. This is sometimes due to the effect of antibodies from the dam’s milk (maternal antibodies) interfering with the response to vaccination. Immunity is also not likely to be sufficient in a dog where only one vaccination has been given. A first parvovirus vaccination should be given between 6 and 9 weeks of age and a second parvovirus vaccination should be given 3 to 4 weeks later. There is some debate about whether the second vaccine should be given at 10 or 12 weeks of age. If it is delayed until 12 weeks, this may mean keeping puppies away from other dogs until then and that time period is thought to be an important age for puppies to interact with other dogs for socialization purposes. However, maternal antibodies are more likely to interfere with vaccines in puppies less than 12 weeks of age. In breeds or individuals at risk, another vaccination at 14 to 16 weeks of age is appropriate. A booster should be given 1 year later and then subsequent booster vaccinations every 3 years. A diet supplemented with antioxidants, e.g. vitamins E and C, β- carotene and selenium was shown in one study to result in an increased response to parvovirus (and distemper) vaccination in puppies. New strains of parvovirus (CPV-2a, 2b, 2c) have emerged since the original (CPV-2) strain was identified in 1978. Novel CPV variants have also emerged in cats and dogs. Vaccines against the original strain can confer protection against the new strains, but disease outbreaks have been reported. Generally dogs with partial immunity from vaccination have a less severe form of the disease. Prognosis Most dogs that survive the initial 2 to 3 days of treatment will recover. The mortality rate without treatment has been estimated to be as high as 91%, but with aggressive supportive therapy decreases to 5 to 20%. Deaths are now less common than when the disease first arose in the 1970s. The improvement in mortality may be due to improved immunity, decreased virulence and/or improved treatment.
More medical literature on Medic.Studio
More on the topic 28 Feline exocrine pancreatic insufficiency:
-
Infectious diseases -
Internal diseases -
Obstetrics and Gynaecology -
Pediatrics -
Veterinary medicine -
-
Conflictology -
Ecology -
Economy -
Finance -
History -
Law -
Medicine -
Philosophy -
Religious studies -
|