27 Intussusception in a cat
Initial presentation
Diarrhoea and poor appetite
Signalment: 2-year-old female entire domestic shorthaired cat, body weight
3.2 kg
Case history
The cat lived at a rescue centre and was brought in with a 3-day history of poor appetite and having watery diarrhoea.
She had been at the rescue centre for about a month and had not been vaccinated or de-wormed during that time as she was pregnant when admitted there. She was nursing two 3-week-old kittens at admission to the hospital and was producing an adequate amount of milk for them.There was no blood or mucus present in the cat’s diarrhoea. It was not known how frequently she was defecating, but she had not been observed to be straining to defecate. The staff at the rescue centre did not believe that she had been vomiting, but were unsure about that part of the history. She did not appear to be drinking or urinating more than previously.
Her previous history was not known as she had come to the rescue centre as a stray cat.
Physical examination
The cat was bright and alert. There was evidence of recent weight loss and she was estimated to be about 6% dehydrated. Her body condition score was 3/9. Her mucous membranes were pink with a capillary refill time of structure present within the intussus- cipiens which was suspected to be an abscess.

Fig 27.1

Figs 27.1 and 27.2
Transverse and sagittal ultrasound pictures of an intussusception in a cat showing the ‘doughnut’ appearance in the transverse, and the double layering of the intestine in the sagittal
(courtesy of Carolina Urraca del Junco)
Treatment and outcome
Presurgical medical management
The cat was started on intravenous clavulanate-potentiated amoxicillin (20 mg/kg q 8 hours) and intravenous fluids were continued until she was thought to be stable enough for anaesthesia and surgery.
Clinical tip
Medical management of intussusception is generally not possible, so the primary treatment is surgical. Surgical management of intussusception involves reduction and/or resection and anastomosis. Upon identifying the intussusception, it is isolated and packed off from the peritoneal cavity. When possible, reduction is facilitated by gentle milking of the intussusceptum from the intussuscipiens. The ensheathing layer is gently compressed over the apex of the intussusceptum while gentle traction is placed on the ileum. In relatively acute cases, reduction is usually accomplished and bowel viability is closely scrutinized. When mature adhesions have formed between the inva- ginated and ensheathing layers, as in this cat, reduction is usually not possible and resection and anastomosis are performed.
In some cases, following reduction and/or resection and anastomosis of the intussusception, a bowel plication or enteropexy technique is performed.
Surgical treatment
In this case, surgery proceeded with a routine midline incision through the linea alba from just caudal to the xiphoid to just cranial to the pubis. An exploratory coeliotomy located a jejuno-jejunal intussusception. The intussusception proved to be non-reducible, as the serosa started to tear when reduction was attempted. The affected piece of bowel was resected with an oblique cut made on the oral side and a straight cut on the aboral side. The oral side of the intestine was spatulated and an end-to- end anastomosis was performed. A routine ovariohysterectomy was performed at the same surgery. The excised loop of intestine was submitted to histopathology to look for an underlying cause.
The histopathology of the biopsy of the resected intestine was described as appearing to be a classic intussusception with a necrotic in- tussuscepted portion of bowel surrounded by degenerating compressed proximal bowel. There were many bacterial colonies present thought to be commensal bacteria proliferating in the hypoxic and necrotic environment.
There was a granulation-like reaction in part of the invaginated part of the intestine that was thought to have been a scarred or healing segment that could have been predisposed to abnormal peristalsis and be the cause of the intussusception.Postoperative care
After surgery the cat was continued on intravenous fluids, antibiotics and analgesia with morphine. Her rectal temperature increased that night to 40.3° C, but decreased the next morning to 39.0° C without intervention. Enrofloxacin (5 mg/kg iv q 24 hours) was added to her antibiotic treatments.
Clinical tip on use of enrofloxacin in cats
In cats, use of enrofloxacin has caused rare incidences of ocular toxicity characterized by mydriasis, retinal degeneration and blindness. These effects were generally seen at higher dosage ranges (>15 mg/kg) and have necessitated a reduction in dosage recommendations in cats to a maximum of 5 mg/ kg/day. Other rare adverse effects seen in cats may include: vomiting, anorexia, elevated hepatic enzymes, diarrhoea, ataxia, seizures, depression/leth- argy, vocalization and aggression.
After 2 days, the cat was bright and had a good appetite. She was initially offered one-third of her resting energy requirement (RER) of food. Initially it was planned to increase her feed to 100% of resting energy requirement by day 3, but after the first day of feeding she had diarrhoea again, so she was kept at one-third of RER. The diarrhoea resolved 3 days later.
Outcome
Prior to discharging the cat back to the rescue centre, she was dewormed with 5 days of fenbendazole at 50 mg/kg/day po. At her re-visit appointment 5 days later she was very bright and eating well and the diarrhoea had resolved.
Discussion and epidemiology
Intussusceptions occur less often in the cat than in the dog. When they do occur, intussusceptions are most often seen in immature cats, although the results of one study suggested that in cats, intussusception has a bimodal age distribution and half of 20 cases were seen in cats less than 1 year of age and nearly half were over 9 years of age.
In the older cats it was often associated with alimentary lymphoma or inflammatory bowel disease. In dogs, 80% of the cases of intussusception are in patients less than 1 year of age. Generally there is no increased risk for any breed reported, although in one study over-represented breeds included Siamese and Burmese cats. There is no increased risk reported with gender or neutering.The exact biomechanical cause of the condition is unknown and it has not been reproduced experimentally. It appears that there is a focal area with inhibited normal propulsive and segmental motility. When a wave of peristalsis moves over the affected area, a proximal bowel segment in- vaginates (becoming the intussusceptum) into a distal section of bowel (the intussuscipiens). Three layers of bowel wall are essentially created, with two from the intussusceptum and one layer from the intussuscipi- ens (Fig 27.3).
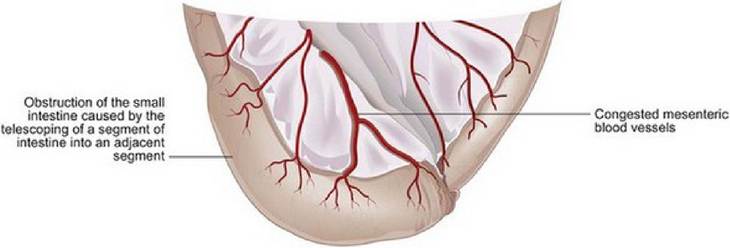
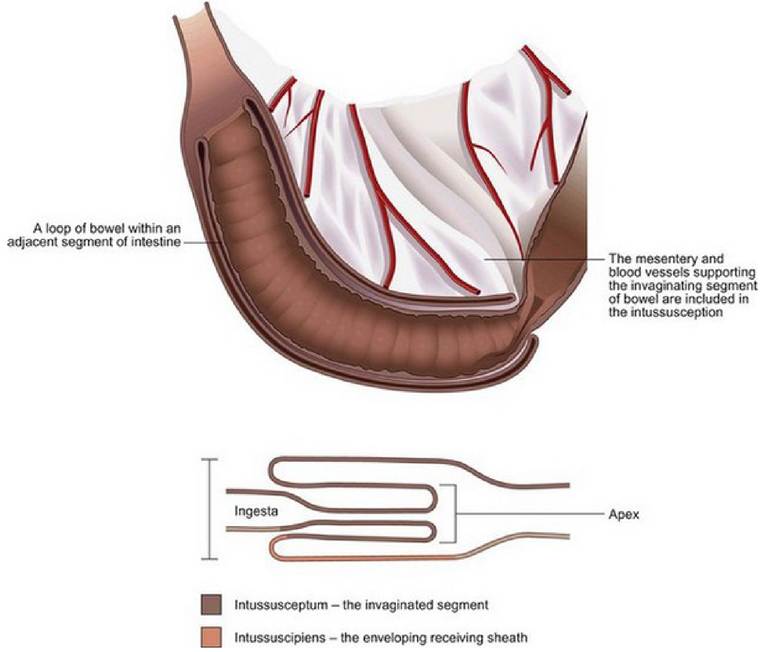
Fig 27.3
Illustration of an intussusception showing the invaginated intussus-
ceptum and the invaginating intussuscipiens
Heavy intestinal parasitism with ascarids or coccidia as well as severe enteritis are possible predisposing causes and as a rescue cat, the chances of parasitism in this case were thought to be high. Other causes include intestinal viral infection, linear foreign bodies, intestinal tumours and adhesions. Intussusceptions are also seen with increasing frequency after laparotomy on elective or non-elective intra-abdominal procedures.
Clinical signs depend on the completeness and level of obstruction. The majority of intussusceptions in dogs occur at the ileocecocolic junction but jejuno-jejunal intussusceptions or pylorogastric and gastro-oe- sophageal intussusceptions are reported. In one study the location was most commonly jejuno-jejunal in cats.
Patients with high intussusceptions usually have profuse vomiting, rapid dehydration and early death. Ileocolic intussusceptions often present with a history of sporadic vomiting, inappetence or bloody stools. If jejuno-jejunal intussusceptions like this one do not cause a complete obstruction, it is possible for them to be chronic and have subtle clinical signs. With more complete obstructions, fluid and electrolyte imbalances occur with the distension of the intestines and the number of bacteria proximal to the obstruction increases dramatically resulting in potential endotoxaemia.
Ultrasonography aids in the diagnosis of intussusception of the intestine. The sonographic appearance of an intussusception in a transverse plane has been described as a ‘target lesion’ or as the ‘multiple concentric ring sign’, reflecting the concentric layers of bowel wall within the intussuscepted segment (Fig 27.1). On longitudinal scan, an intussusception has the appearance of a thickened segment of bowel with an excessive number of layers that alternate in echogenicity (Fig 27.2). It should be noted that other gastrointestinal disorders can also cause ‘target’ or ‘bull’s eye’ type lesions. Therefore, when intussusception is suspected on a transverse image, the lesion must be examined in a longitudinal plane as well.
In most cases, the obstruction is incomplete and a chronic course of poor appetite, diarrhoea or bloody tenesmus is seen for several weeks.
In the majority of reported feline intussusception cases, resection and anastomosis of the intestine was necessary. Enteroplication of the intestines after surgery for intussusception used to be routinely recommended, although one study found no significant difference in the follow-up of canine cases where this procedure was or was not done and it is not without potential complications.
Although the invaginated bowel may become devitalized, perforation resulting in peritonitis is relatively rare because the outer ensheathing layer retains its viability and fibrinous adhesions seal the proximal border of the intussusception. Occasionally spontaneous recovery occurs when the nonviable intussusceptum is sloughed and patency of the intestinal lumen is re-established.
Prognosis
Prognosis for a successful outcome after surgery is good; with over 80% of reported cases doing well, although the number of cases reported is low.