Oncologic Emergencies
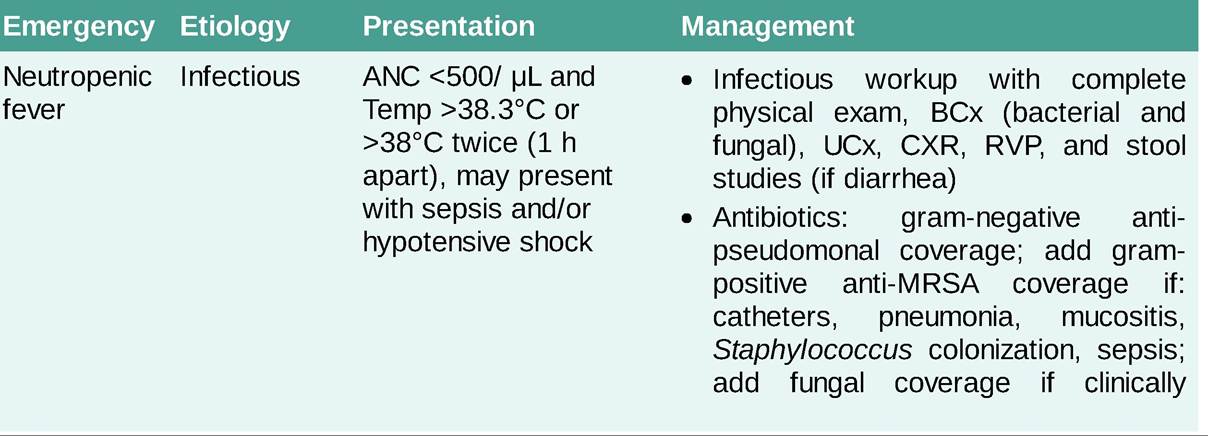
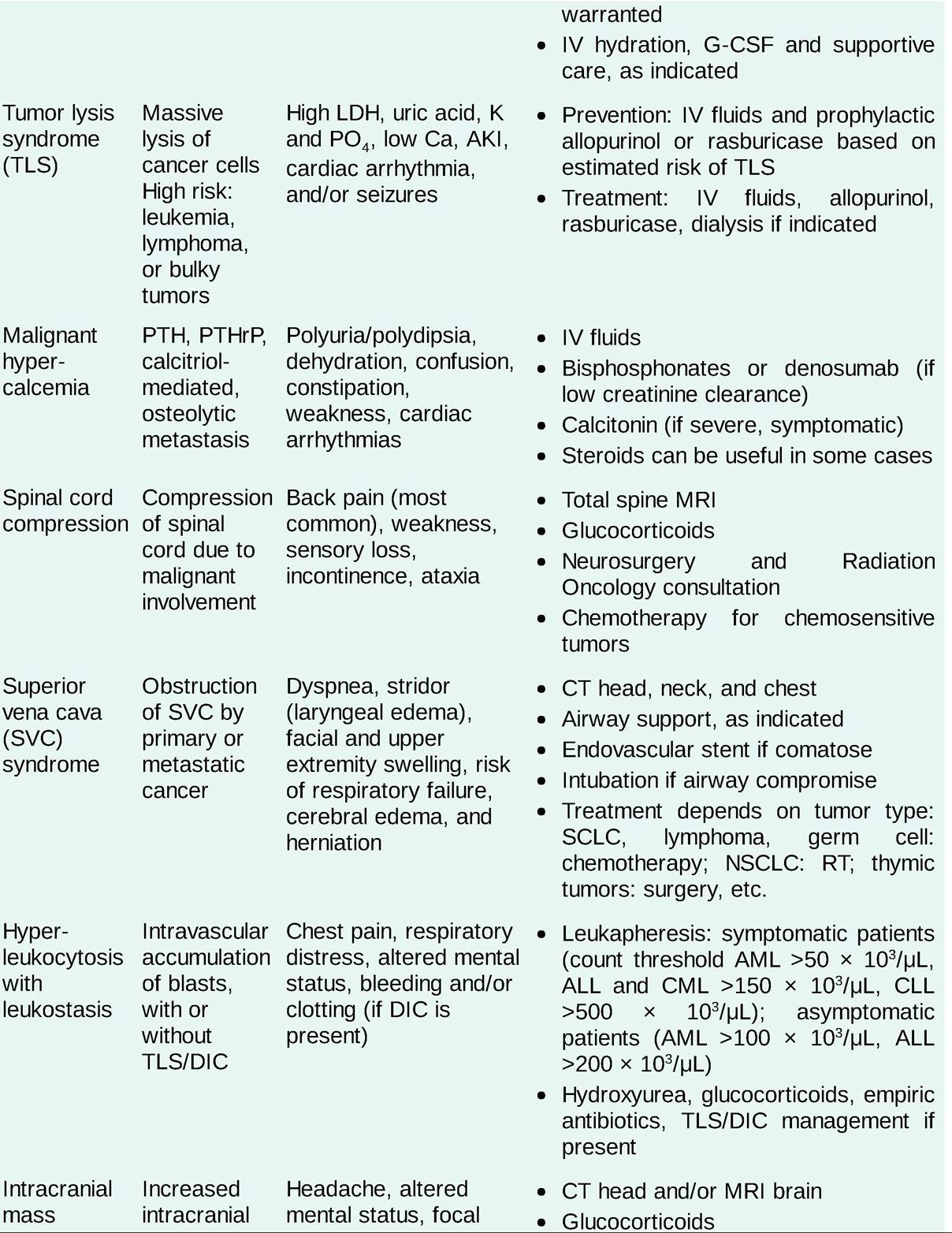
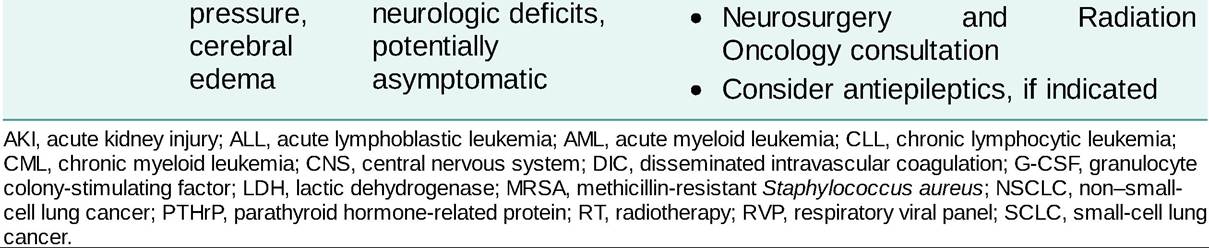
The most common oncology emergencies are febrile neutropenia (FN), TLS, malignant hypercalcemia, spinal cord compression, SVC syndrome, hyperleukocytosis, and brain metastases with increased intracranial pressure (Table 22-12).
TABLE 22-12
ONCOLOGIC EMERGENCIES
Supportive Care
Nausea and Vomiting
• If nausea/vomiting occurs, chemotherapy-induced nausea and vomiting (CINV), as well as alternative etiologies such as bowel obstruction, brain metastasis, constipation and gastroenteritis, should be considered.
• CINV can be categorized as acute (lt;24 hours) or delayed (gt;24 hours). Acute CINV is an important predictor of delayed CINV.
• Commonly used antiemetic medications for prevention and management of CINV include dexamethasone, 5-hydroxytryptamine-3 (5-HT3) receptor antagonists (ondansetron, granisetron, dolasetron, palonosetron), neurokinin-1 receptor antagonists (aprepitant, fosaprepitant, etc.), prochlorperazine, anxiolytics (lorazepam), and olanzapine (atypical antipsychotic).
Diarrhea
• Diarrhea can be a common complication of chemotherapy (irinotecan, 5FU, capecitabine), targeted therapy (erlotinib, cetuximab, sunitinib, lapatinib), immunotherapy (ipilimumab, nivolumab, pembrolizumab), and stem cell transplantation (GI GVHD, CMV colitis) or may be a manifestation of cancer itself (carcinoid syndrome in neuroendocrine tumors).
• Treatment should be tailored to the underlying etiology. Supportive care with IV fluids and antidiarrheal medications (loperamide, diphenoxylate, atropine), antibiotics for infectious etiologies (oral vancomycin or IV metronidazole for Clostridioides difficile), and glucocorticoids for immune- related etiologies (ICIs or GI GVHD) may all be considered in the appropriate clinical context.
Interruption of treatment with the causative agent (until resolution of symptoms) and/or dose reduction may be considered, as indicated.Immune-Checkpoint Inhibitor-Related Adverse Events
• ICI-related adverse events (AEs) are due to activation of a patient's immune system toward selfantigens leading to autoimmune mediated toxicities, which can sometimes be permanent and lifethreatening. ICI-related AEs may include but are not limited to: rash, gastroenteritis/colitis, hepatitis, endocrinopathies, arthritis, pneumonitis, myocarditis, and cytopenias.
• The treatment of choice for ICI-mediated AEs is largely driven by the severity of the AE (grade) and usually involves prompt discontinuation of the ICI and initiation of glucocorticoids, such as prednisone (doses ranging from 0.5 to 1 mg/kg daily). Depending on the type of ICI-related AE, prolonged treatment with steroids followed by a long and gradual taper may be necessary. “Flare” of the ICI- related AE may be observed with weaning of steroids, even in the absence of re-exposure to the
immunotherapy.
• Additional supportive care for ICI-related AEs may include supplementation of hormones such as insulin for new-onset type-1 diabetes, thyroid replacement (levothyroxine) for hypothyroidism, and supportive care with hydration and anti-diarrheal medications for colitis, and transfusions and growth factors as necessary for cytopenias.
Cytokine Release Syndrome and Immune Effector Cell-Associated Neurotoxicity Syndrome
• Cellular and cell-engaging therapies, such as CAR-Ts, are associated with unique toxicities including cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS). CRS is characterized by the systemic release of supraphysiologic proinflammatory cytokines (e.g., IL-2, IL-6, IFN-gamma, TNF-alpha) by immune effector cells characterized by systemic inflammation, fevers, hypotension, and hypoxemia. ICANS is an incompletely understood syndrome characterized clinically by the presence of tremor, dysgraphia, expressive speech impairment (particularly naming objects), decreased level of consciousness, and when severe, coma, cerebral edema, and seizures.
• Grading and treatment: The American Society of Transplantation and Cellular Therapy (ASTCT) has published guidelines for the grading and management of CRS and ICANS.41
• CRS is graded on a scale of 0-4, with Grade 0 representing no CRS up to Grade 4 representing severe CRS characterized by fevers, hypotension requiring multiple vasopressors, and/or respiratory failure requiring mechanical ventilation. In general, CRS is managed with supportive care including empiric antibiotics, IV fluids, antipyretics, blood pressure support, and O2 support adjusted to the associated CRS Grade. In addition, tocilizumab (an IL-6 receptor monoclonal antibody), siltuximab (an IL-6 monoclonal antibody), and glucocorticoids are frequently used in the management of Grade 2-4 CRS.
• The ICANS Grade is determined by combining the Immune Effector Cell-Associated Encephalopathy (ICE) Score with the presence of additional clinical findings. The ICE score ranges from 10 representing a normal score to 0 representing a severely impaired score. The clinical findings impacting ICANS include level of consciousness, seizures, cerebral edema, and other neurologic deficits. ICANS is graded on a scale of 0-4, with Grade 0 representing no ICANS up to Grade 4 representing severe ICANS characterized by complete obtundation, ICE score of 0, cerebral edema, and the potential for focal neurologic deficits and/or seizures. In general, ICANS is managed with supportive care, seizure prophylaxis (levetiracetam), close neurologic monitoring, glucocorticoids, and intensive management of seizures and/or cerebral edema if they occur.
Cancer Pain
• Cancer patients frequently experience pain due to multiple etiologies, including somatic pain (bone metastases, musculoskeletal inflammation, surgery/procedures), visceral pain (tumor infiltration/compression/distention of viscera), and neuropathic pain (tumor infiltration of nervous tissue, nerve injury due to chemotherapy, radiotherapy, or surgery).
• Cancer pain is usually managed through a rational, stepwise approach to target the underlying cause of pain as well as the symptoms of pain. Common pain medications include non-opioid analgesics (NSAIDs, acetaminophen, and/or topical agents), opioids (tramadol, hydrocodone, oxycodone, morphine, hydromorphone, methadone, transdermal fentanyl, etc.), systemic glucocorticoids in certain circumstances, (bone metastases, spinal cord or nerve compression), antidepressants (nortriptyline, etc.), gabapentin, or pregablin. In addition, bisphosphonates and radiolabeled agents (strontium-89 and samarium-153) may help in treating bone metastases-related pain. Patients who experience inadequate pain control despite aggressive medical therapy may benefit from interventional therapies, such as regional infusion of analgesics and neuroablative or neurostimulatory procedures.
• Common side effects of opioid therapy include constipation, nausea, respiratory depression, and sedation. Constipation prophylaxis with stimulant laxatives (senna) and stool softeners (docusate) is frequently used. Constipation, if it occurs, can be managed with lactulose, magnesium citrate, polyethylene glycol, enemas, and/or mu opioid receptor antagonists.
Fatigue
Fatigue occurs in an estimated 80% of patients with advanced cancer, often with multiple contributing factors such as pain, poor nutrition, emotional distress, sleep disturbance, and medical comorbidities (anemia, infection, organ dysfunction). Appropriate pain management, nutrition support, sleep therapy, exercise, and necessary supportive care can help address some of these issues. Transfusion support and erythrocyte stimulating agents may be helpful in select patients with anemia. Psychostimulants such as methylphenidate or modafinil can prove helpful in some patients with severe symptoms. Antidepressants may be useful if concurrent depression is present.
Anorexia and Cachexia
Decreased appetite and weight loss are common. In addition to caloric supplementation orally, enterally (nasogastric or gastric tube), or parenterally (total parenteral nutrition), patients may benefit from pharmacologic therapy to increase appetite, including megestrol acetate, glucocorticoids, or dronabinol.
More on the topic Oncologic Emergencies:
- Oncologic Emergencies and Supportive Care
- 26 Medical Emergencies
- Airway Emergencies
- Chapter 16 Cardiological Emergencies in HIV-Infected Patients
- Many cardiac complications in acquired immunodeficiency syndrome (AIDS) that may be faced by emergency department (ED) physicians are due to opportunistic infections or malignancy, but they may also be associated with other aspects of human immunodeficiency virus (HIV) disease and its treatment (Table 1) [1].
- Emergency of technogenic character
- It was early 2008. By this time, I had heard many stories from people in Mali, Cambodia, El Salvador, and Guatemala about how Saving for Change had changed their lives.
- ABDOMINAL PAIN
- Summary
- Agency Planning to Ensure Continuity of Essential Veterinary Functions during a Pandemic Is Incomplete
- Radiation safety
- Information Processing and Documentation During Transport