35 Introduction to the colon and colonic disorders
The large intestine comprises the caecum, colon, rectum and anus (Fig 35.1). The primary role of the colon is the resorption of water and electrolytes. Colonic bacteria break down fermentable fibre to produce short chain fatty acids - acetate, butyrate and proprionate.
Butyrate is an essential energy source for colonocytes.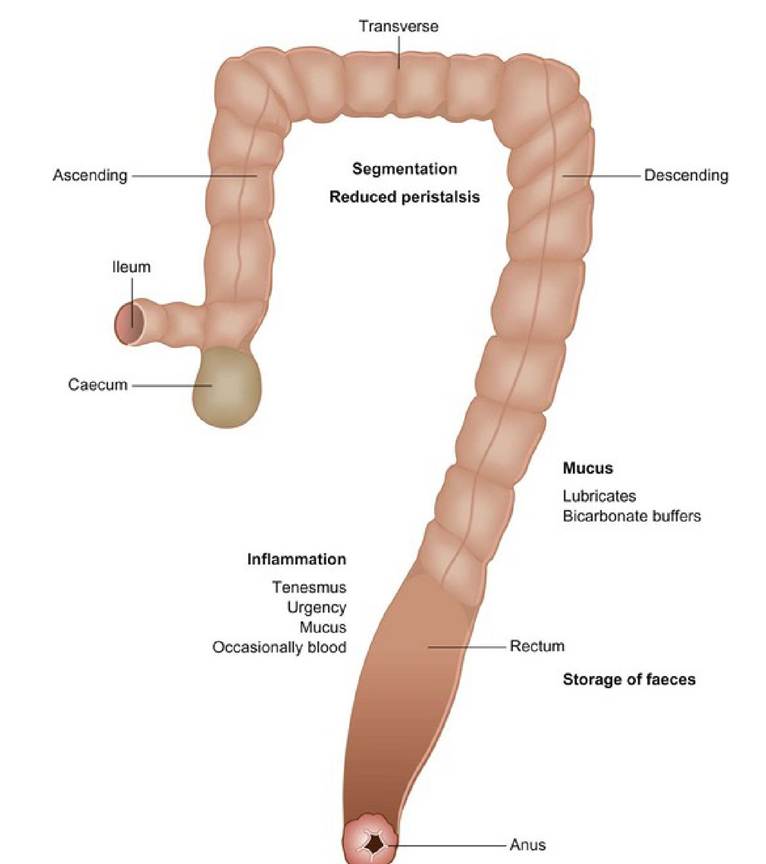
Fig 35.1
Illustration of the large intestine, which comprises the caecum,
colon, rectum and anus.
Diarrhoea associated with the colon occurs when there is interference with water or electrolyte resorption, abnormal motility or presence of abnormal luminal substrate following pancreatic, hepatic or small intestinal disease.
Diseases of the colon include:
• Diarrhoea
• Constipation and megacolon
• Neoplasia
• Rectal disease; neoplasia, strictures, foreign bodies
• Colonic vascular dysplasia
• Typhilitis - rare
Causes of large bowel diarrhoea include:
• Inflammatory disease
• acute non-specific colitis
• chronic colitis, non-specific colitis, inflammatory bowel disease
• infectious colitis (bacteria as for small intestinal disorders)
• parasites, e.g. Trichuris, Coccidia
• Obstructive disease
• intraluminal obstruction, e.g. tumour, constipation, foreign body, intussusception, stricture
• extraluminal obstruction (hernia, masses, adhesions)
• Ischaemic disease - infarct, intussusception
• Neoplasia
• adenocarcinoma
• lymphoma
• benign polyps
• Non-inflammatory disease
• motility disorders, e.g. irritable bowel syndrome (IBS)
• congenital malformations
• Systemic disorders
• toxaemias (e.g. pyometra, peritonitis)
• uraemia
• pancreatitis
• Dietary causes
• food poisoning
• intolerance or allergy
• foreign material (bones, hair, plastic)
• Secondary to unabsorbed nutrients from small intestinal diarrhoea
Clinical signs of large intestinal disease include:
• Chronic or acute diarrhoea
• Tenesmus
• Dyschezia
• Haematochezia
• Mucus production
• Abdominal pain
• Intermittent vomiting (20% of cases)
Investigation of large intestinal disorders
An initial minimum data base, especially faecal testing, as for small intestinal diarrhoea (see page 116) may be helpful in chronic cases.
In cats, a fresh saline faecal preparation should be examined for Tritrichomonas foetus under the microscope and a sample sent for PCR test.Imaging
Radiology and ultrasound may be helpful for diagnosing megacolon, foreign bodies, bowel thickening or focal masses, mesenteric lymphadenopathy (usually a non-specific finding) and intussusceptions. Computerized tomography is also useful for localizing and assessing focal or generalized bowel thickening.
Colonoscopy and biopsy
Colonoscopy allows for visualization of the colonic mucosa (if preparation is adequate) (Fig 35.2) and observation of intraluminal masses, mucosal texture and colour. Submucosal vessels should be visible; if they are not visible, it indicates thickening of the mucosa. Generalized or focal haemorrhage is seen in some cases.
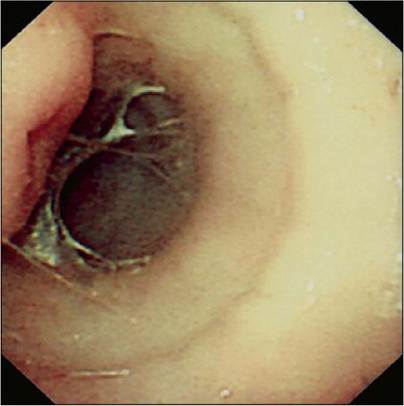
Fig 35.2
Colonoscopy allows visualization of the colonic mucosa.
Biopsy may confirm the presence of inflammatory or neoplastic cells. Often in cases of large bowel diarrhoea the histology of the colonic biopsy shows little or no inflammation. These cases may be analogous to the human condition of IBS.
Irritable bowel syndrome
Irritable bowel syndrome (IBS) is thought have an underlying motility disorder and possibly the patient has an increased sense of colo-rectal pain. The patient presents with diarrhoea or constipation, often intermittent, and may also show vomiting, abdominal pain, borborygmi and flatulence. No pathological lesion is found at colonoscopy or on histopathology of colonic mucosa. It may be associated with stress and is sometimes detected in working dogs. There is no definitive diagnostic test for IBS, it is diagnosed by exclusion of other disorders.
Dietary management with increased soluble fibre helps some cases. Motility modifying drugs such as loperamide, buscopan and mebeverine may also be tried.
Constipation
Constipation may be defined as infrequent or difficult passage of faeces.
This may be an acute or chronic problem, but there is no permanent loss of function, whereas with obstipation the constipation is refractory and no longer responds to medication.Megacolon, which literally translates as huge colon, is often a clinical finding in association with obstipation. Colonic impaction is the presence of hard faeces within the colon that are no longer moving caudally. It can be associated with constipation, obstipation or megacolon, but does not necessarily mean loss of function.
The clinical signs may include tenesmus, dyschezia, small volume and increased frequency of defaecation. Blood may appear on the surface of faeces.
The aetiology of constipation is extensive and not confined to disorders of the colon. It is therefore very important to examine the patient thoroughly as part of the investigation of this disorder.
Causes of constipation include:
• Ingestion of indigestible material, e.g. bones, hair, cat litter, fibrous plants
• Lack of exercise, e.g. obesity, orthopaedic disease, hospitalization
• Painful defecation, e.g. orthopaedic disease, perianal disease
• Mechanical obstruction
• colorectal mass
• congenital anorectal lesions
• healed pelvic fracture with stenosis
• intrapelvic mass
• perineal hernia
• enlarged prostate
• pseudocoprostasis
• rectal diverticulum
• strictures
• Neurological disease
• dysautonomia
• idiopathic megacolon (most common cause of obstipation in cats)
• paraplegia
• sacral spinal cord deformity (e.g. in some Manx cats)
• Miscellaneous, e.g. dehydration, drugs, hypokalaemia, hypothyroidism, hypoparathyroidism
Treating the impaction may involve giving enemas, oral laxatives, mineral oils and, if necessary, manual removal of faecal material under general anaesthesia. Most cases should receive intravenous fluids prior to starting other treatments.
The prognosis is guarded as the problem may recur, especially if the underlying problem has not been resolved.
Failure to correct the constipation may lead to the development of megacolon.Megacolon
Congenital and acquired cases of megacolon occur (Fig 35.3). Acquired cases of dilated megacolon are often the end stage condition of idiopathic colonic dysfunction. There is an abnormality of smooth muscle function in cats with idiopathic dilated megacolon.
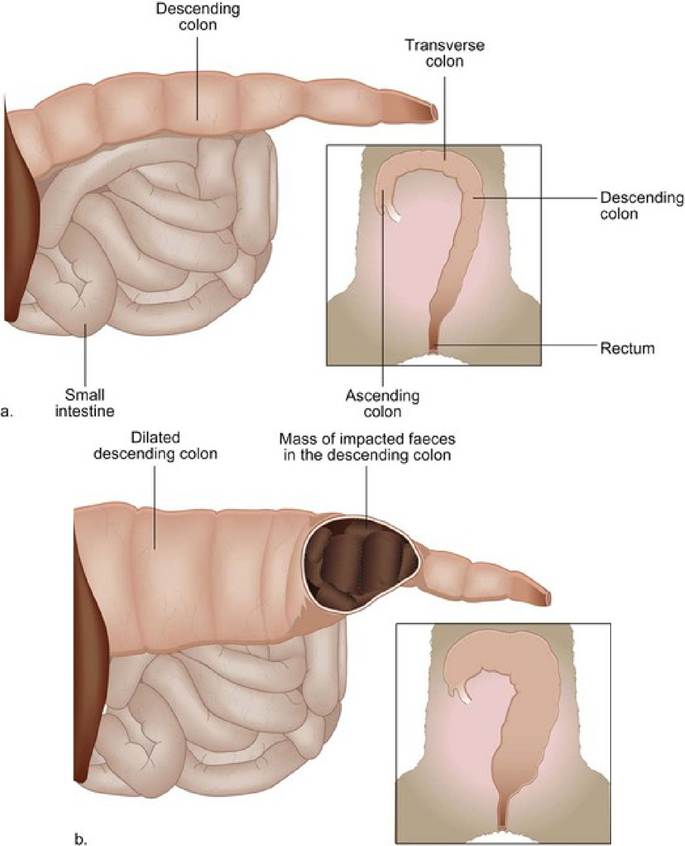
(a) Normal colon. (b) Megacolon.
Fig 35.3
Hypertrophic megacolon may occur due to obstructions such as pelvic fracture and stenosis, neoplasm or chronic foreign body. Feline dysauto- nomia and canine dysautonomia are also acquired causes of constipation that may lead to megacolon.
Congenital cases are thought to be associated with failure of adequate myenteric plexus development.
Patients may present with reduced, absent or painful elimination of hard faeces. Dehydration may occur. Radiographs usually show an enlarged colon, with distension occurring throughout the colon. A healed pelvic fracture with malunion or other obstruction may be seen with hypertrophic megacolon. The diagnosis is based on history, clinical findings and radiography.
There are five aspects to managing the patient with megacolon: optimal systemic hydration, removal of impacted faeces, increased dietary fibre (early in disease) to increase faecal bulk and stimulate motility, laxatives and colonic prokinetic agents such as cisapride (where available), prucalopride and tegaserod.
Colonic neoplasia
The most common tumours seen in the large intestine include lymphomas, adenocarcinomas and rectal adenomatous polyps.
Diagnosis depends on rectal examination, imaging studies (e.g. barium enema and radiography or CT scan, ultrasound of the more proximal colon) and colonoscopy and biopsy with histopathology.
Treatment depends on the type of tumour. If an adenocarcinoma is focal and surgically accessible, it may be resected. Piroxicam either as a rectal suppository or orally or other non-steroidal anti-inflammatory drugs may decrease the clinical signs of rectal adenocarcinomas and adenomas.
Rectal diseases
Rectal stricture
Rectal strictures are surprisingly common in dogs but rare in cats. The aetiology is often not determined but may be the result of previous trauma or associated with neoplasia.
Patients present with haematochezia and dyschezia. They may become constipated due to avoiding painful defecation.
On rectal examination the stricture will usually be palpated easily and where neoplasia is present, a roughening or obstruction may be felt. Endoscopy and biopsy with histopathology are essential to rule out neoplasia.
Treatment involves surgical correction where possible. Stretching may also be considered in those cases unsuitable for surgery.
More on the topic 35 Introduction to the colon and colonic disorders:
- 5 The Colon and Colonic Disorder
- Resources for tests for gastrointestinal disorders
- Cerebral palsy (CP) is defined as “a group of disorders of the development of movement and posture, causing activity limitations that are attributed to nonprogressive disturbances that occurred in the developing fetal or infant brain” (1).
- 32 Colonic vascular ectasia in a dog
- 39 Colonic inflammatory bowel disease in a cat
- Introduction to haematochezia and melaena
- 1 Introduction
- Introduction
- Introduction
- 19 Introduction
- Introduction
- Introduction
- INTRODUCTION
- Introduction
- Introduction
- Introduction
- Introduction