39 Colonic inflammatory bowel disease in a cat
Initial presentation
Diarrhoea, decreased appetite and weight loss
Signalment: 11-year-old, male neutered, domestic shorthaired cat, body weight 3.8 kg
Case history
The cat had a 1-month history of decreased appetite and weight loss, along with increasingly softer faeces.
There was some increase in the frequency of defecation and the owner reported that mucus and fresh blood had been present on some occasions. The consistency of the faeces was described as ‘cow-pat’, i.e. soft but formed. He sometimes vomited, although the owners reported that this had been occurring for years.The cat had been vaccinated within the past year, but had not been de-wormed for several years. His usual diet was a commercial canned cat food, fed two to three times per day. During the past month the owner had also been feeding him cooked ham and canned tuna to encourage his appetite.
Physical examination
Physical examination revealed the cat to be bright, alert and responsive. He was in slightly thin body condition (body condition score 4/9) and appeared well hydrated. His mucous membranes were pink with a capillary refill time of less than 2 seconds. Oral examination showed that most of his teeth were missing but was otherwise unremarkable.
Thoracic auscultation revealed a heart rate of 200 beats per minute with matched pulses. Heart and lung sounds and percussion and compression of the thorax were unremarkable. The respiratory rate was normal at 32 breaths per minute. Abdominal palpation was not resented. There was possible abdominal lymph node enlargement. Rectal temperature was 38.3° C. The remainder of the physical examination was unremarkable.
Problem list and discussion of problems
• Diarrhoea
• Weight loss
• Decreased appetite
The diagnostic approach to diarrhoea usually begins with determining if the cause is large or small intestinal in origin.
The diarrhoea in this case appeared to have a large intestine component due to the increased frequency and the presence of fresh blood and mucus. However, concurrent involvement of the small intestine could not be ruled out, especially with the presence of weight loss. The decreased appetite and weight loss were thought to be related to the diarrhoea. Differential diagnoses for decreased appetite include those which cause the animal to be unable to eat (can’t eat) and those in which the animal does not want to eat (won’t eat); in this case the cat was able to eat so the decreased appetite was likely due to illness.Differential diagnosis
Large intestinal diarrhoea
•Inflammatory conditions
• non-specific colitis
• chronic inflammatory colitis, e.g. plasmacytic/lymphocytic, eosinophil
ic, granulomatous, suppurative
•Infectious causes
•FIP
• feline leukaemia virus (FeLV)
• Salmonella
• Campylobacter
• Clostridium perfringens
•Parasitic
• whipworms
• hookworms
• Giardia
• Tritrichomonas foetus
• Toxoplasma gondii
•Diet related
• dietary sensitivity (allergy or intolerance)
• fibre responsive diarrhoea
•Neoplasia, e.g lymphoma, adenocarcinoma, others
•Systemic disorders
•Uraemia
• toxicities
• pancreatopathy
• Secretagogues, e.g. unconjugated bile acids, hydroxylated fatty acids secondary to small intestinal disorders
Small intestinal diarrhoea
• Diet related
• dietary sensitivity
• food poisoning
• sudden change of diet
• Small intestinal disease
• inflammatory bowel disease, e.g. plasmacytic/lymphocytic, eosinophilic, other
• infectious (viral, bacterial enterotoxins, fungal - although fungal disorders of the small intestine are unlikely in the UK)
• parasites, e.g. Giardia, cryptosporida, Strongyloides, ascarids, hookworms, Toxoplasma gondii
• neoplasia, e.g. lymphoma, mastocytosis
• lymphangiectasia (uncommon in cats)
• ileus, e.g. hypokalaemia, enteritis, dysautonomia
• antibiotic responsive diarrhoea
• Pancreatic disorders
• pancreatic exocrine insufficiency
• Chronic pancreatitis
• Liver disorders
• liver failure
• intrahepatic cholestasis
• bile duct obstruction
• Kidney disease and uraemia
• Hyperthyroidism
• Congestive heart failure
• Hypoadrenocorticism (uncommon in cats)
Case work-up
A 4- to 6-week dietary trial with a highly digestible restricted novel protein or hydrolyzed diet is appropriate in some cases of diarrhoea.
With cases of colitis, the addition of mixed soluble and insoluble fibre sources may also be of benefit. The use of probiotics and prebiotics are also being investigated in intestinal disorders of dogs and cats. In this case, however, as the cat was not eating well and had been losing weight, prompt investigation rather than waiting for the results of a dietary trial was indicated.Minimum data base
Routine haematology was performed and revealed a moderate mature neutrophilia (21.7 ? 109∕l; reference range: 2.5-12.8 ? 109∕l) and a mild monocytosis (1.06 ? 109∕l; reference range: 0.07-0.85 ? 109∕l). Blood smear analysis confirmed these findings and showed atypical, reactive appearing lymphocytes, suggestive of antigen stimulation.
Serum biochemistry results revealed a marginal increase in urea (9.9 mmol/l; reference range: 2.8-9.8) and bile acids (7.2 mmol/l; reference range 0-7) and a marginal hypophosphataemia (1.39 mmol/l; reference range: 1.4-2.5). Mild hypoalbuminaemia (24.0 g/l; reference range: 28-39) was also present.
Clinical tip on decreased serum albumin
Decreased serum albumin can be due to decreased production by the liver, increased loss via the intestines or kidneys or a ‘third space shift’ (e.g. into an obstructed loop of intestine, the pleural space or the peritoneal space). Production may also be decreased in inflammatory states, as it is a negative acute phase protein and decreases whereas production of some of the other proteins increases. After checking for urinary loss (a urine protein to creatinine ratio), further diagnostics involve looking for evidence of hepatic or gastrointestinal disorders or inappropriate fluid accumulation.
To assess the pancreas, serum samples were submitted for measurement of feline pancreatic lipase (fPL) and trypsin-like immunoreactivity (TLI) which were both found to be within the reference range (fPL: 1.2 μg∕l; reference range: 0.1-3.5; TLI: 22.5 μg∕l; reference range: 12-82).
Both serum folate (4.2 μg∕l; reference range: 9.5-20.2 μg∕l) and serum cobalamin (186.0 ng/l; reference range: 270-1000 ng∕l) concentrations were decreased and supplementation was initiated.
Clinical tip on serum folate and cobalamin
Cobalamin is absorbed in the ileal part of the small intestine. It requires prior binding with intrinsic factor, which comes from the pancreas in cats (and the stomach and pancreas in dogs). Deficiency may be caused by poor absorption due to intestinal disease or exocrine pancreatic insufficiency, excessive bacteria in the upper small intestine utilizing the vitamin or a deficiency in intrinsic factor. In humans who are vegetarians (especially elderly humans), a dietary deficiency is possible; however, this is unlikely in cats as they cannot successfully be vegetarians.
Unlike most other B vitamins, cobalamin is stored in the body. In healthy cats the half-life is 11 to 14 days and in cats with gastrointestinal disease it is only 4.5 to 5.5 days. Clinical signs of cobalamin deficiency in humans include anaemia, thrombocytopenia, neuropathies and digestion abnormalities. In cats (and dogs) the clinical signs are not as well described; however, it has been suggested that response to treatment of intestinal disorders is improved with cobalamin repletion. A high serum concentration of cobalamin does not appear to have clinical significance and may occur with supplementation. The recommended dose for treatment of gastrointestinal disease in humans exceeds the recommended daily amounts and there is a consideration that there may be positive pharmacological effects.
Folate is absorbed only in the proximal intestine. A deficiency usually indicates small intestinal disease and if it is accompanied by a cobalamin deficiency it likely indicates widespread disease. A high serum folate can be caused by bacterial production, although serum concentrations of this vitamin can also be increased by dietary intake.
Serum T4 was at the low end of the reference range at 15.3 nmol/l (reference range: 15-48 nmol/l). An feline immunodeficiency virus (FIV)∕FeLV ELISA was performed which was negative for FeLV but positive for FIV antibodies.
Toxoplasma serology showed a negative IgM titre (1 : 64 or a four-fold or greater increase in paired (2 to 3 weeks apart) IgG titres is likely to indicate disease. The absence of the titre increases does not rule out toxoplasmosis as some cats and dogs with the disease will undergo an antibody class shift from IgA to IgM. A response to treatment (e.g. clindamycin) is diagnostically supportive (although not definitive of diagnosis) if there is a suspicion of disease.
Urinalysis showed a urine specific gravity of 1.048, indicating good urine concentrating ability. The chemistry strip was unremarkable, and the urine sediment was inactive. Urine protein to creatinine ratio was 0.13 (reference range there were no obvious mass lesions or ulcerated areas. Biopsy samples were collected from the stomach, duodenum and colon. While the cat was anaesthetized for endoscopy, fine needle aspirates of an enlarged mesenteric lymph node and the thickened colonic wall were also taken under ultrasound guidance and submitted for cytological evaluation.
Fig 39.3

Endoscopic picture of colonic mucosa showing thickening and loss of visualization of submucosal vessels
Cytology of the lymph node aspirate was suggestive of reactive hyperplasia. The colonic wall cytology was, unfortunately, non-diagnostic.
Histopathological examination of the gastric mucosal biopsies revealed the presence of some Helicobacter-like spiral organisms at the surface of the gastric mucosa. There was no associated gastric inflammation and it was therefore considered an incidental finding.
Clinical tip on gastric Helicobacter
A causal role of Helicobacter in chronic gastritis and vomiting in dogs and cats has not been established, although there are cases in which treatment improves the clinical condition.
As in this case the spiral bacteria present were only on the surface of the mucosa and there was no gastric inflammation or clinical signs; treatment was not warranted. Where there are clinical signs, evidence of inflammation and the organisms are located within the gastric pits or submucosally, treatment is probably indicated.The small intestinal mucosal biopsies revealed evidence of mild, diffuse chronic enteritis. Histopathology of the colonic mucosal biopsies showed severe, multifocal, granulomatous ulcerative colitis (Fig 39.4). There was no evidence of any aetiological agents and Ziehl-Neelsen stains of the colonic biopsies for the presence of acid fast (i.e. mycobacterial) organisms were negative.
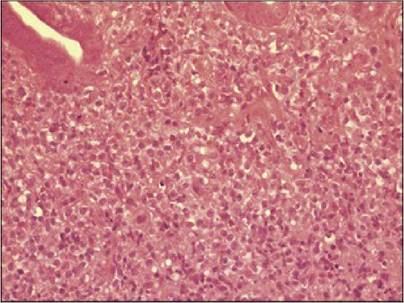
Fig 39.4
Histopathology of the colon showing severe, multifocal, granulomatous ulcerative colitis
(courtesy of Professor Elspeth Milne)
Treatment and outcome
This cat was diagnosed with a granulomatous ulcerated from of colonic inflammatory bowel disease, complicated by a positive FIV status. The FIV may either have caused or contributed to the cat’s clinical condition. The enteritis in the small intestine was thought to be of less significance, although may have contributed to decreased nutrient absorption.
Initial treatment included:
• Prednisolone: 5 mg po q 24 hours
• Marbofloxacin: 7.5 mg po q 24 hours
• Folic acid: 2.5 mg po q 24 hours
• Vitamin B12: 300 μg sq every 7 days for 3 weeks
• A novel restricted protein, highly digestible canned diet
Clinical tip on fluoroquinolone use in cats
In some cats given enrofloxacin, retinal degeneration leading to partial, temporary or total blindness has occurred. This reaction is not common even with very high doses, but there is no way to predict which cats will react. This reaction has only been reported with enrofloxacin and not with other fluoroquinolones, as it is theorized that the biochemical structure of enrofloxacin leads to especially high concentrations in the feline eye. Because of the potential adverse reactions to enrofloxacin in cats, marbofloxacin was initiated in this cat prior to the results of the periodic acid-Schiff tests in the chance that similar pathophysiology to the histiocytic colitis of Boxer dogs might be present.
At the time of discharge the cat was very bright, with a good appetite, having gained 500 g since admission and with only intermittently soft stools.
Two weeks later the owners reported that the cat had done very well; his faecal quality was improving and he had gained some weight. After the marbofloxacin was stopped, the cat immediately showed signs of diarrhoea again and it was re-instituted 2 days later. The cat again improved and has remained well while continuing on marbofloxacin.
Pathophysiology and prognosis
In general, the more common forms of inflammatory bowel disease, with infiltration of lymphocytes and plasmacytes or even eosinophils, carry a relatively good prognosis for improvement in clinical signs.
Granulomatous colitis or enteritis, however, has a more guarded prognosis. Granulomatous colitis is characterized by the presence of aggregates of histiocytes in the lamina propria. In this cat the infiltration of the mucosa and lamina propria was described as predominantly large macrophage like cells, which may have been a histiocytic type of cell. The presence of underlying infectious causes (e.g. mycobacterial organisms, parasitic organisms, feline infectious peritonitis or fungal infections, although the latter are uncommon in the UK) should be ruled out before treatment with corticosteroids or other immunosuppressive drugs is used. Metronidazole is commonly used in feline chronic colitis, as it has multiple effects: antibiotic, antiprotozoal and inhibition of some aspects of cell mediated immunity.
An ulcerative histiocytic colitis has been reported in young Boxer dogs, which presents with thickened colonic mucosa and haemorrhage. This disorder shows a cellular infiltrate of plasma cells, lymphocytes and periodic acid-Schiff positive macrophages. The presence of the periodic acid-Schiff positive macrophages is a discriminating feature between this form of colitis and granulomatous colitis.
An infectious aetiology is suspected for this histiocytic disorder and treatment of cases early in the course of disease with enrofloxacin has been successful. Treatment is lifelong in these cases.
Cats with FIV show a significant incidence of dental disease (50-52% of seropositive cats) and most of the teeth in this cat had been lost or removed. A significant number (15-20%) of seropositive cats show chronic enteritis or enterocolitis. Clinical signs include anorexia, chronic diarrhoea, dehydration and weight loss. The diarrhoea may be persistent and, as in this cat, intestinal thickening develops. A high mortality rate is seen in FIV positive cats with gastrointestinal signs.
More on the topic 39 Colonic inflammatory bowel disease in a cat:
- 39 Colonic inflammatory bowel disease in a cat
- Table of Contents
- Canine inflammatory bowel disease activity index (CIBDAI)
- 4 Haematochezia and Melaen
- 15 Lymphocytic inflammatory bowel disease/al- imentary lymphoma in a cat
- 32 Colonic vascular ectasia in a dog
- 35 Introduction to the colon and colonic disorders
- 19 Pancreatitis in a cat
- 20 Linear foreign body in a cat
- 26 Inflammatory bowel disease and adverse reaction to food in a dog