20 Linear foreign body in a cat
Case co-written by Carolina Urraca del Junco
Initial presentation
Vomiting
Signalment: 9-month-old neutered male domestic shorthaired cat body weight 3.3 kg
Case history
The cat had been vomiting for 5 days.
The vomitus initially had contained food and then contained primarily liquid. The cat was not eating and had reportedly lost weight. There had been no diarrhoea, although he had not passed faeces for 2 days.He had been given his vaccinations as a kitten and had last been dewormed 4 months previous to presentation. He had not been given any treatments for ectoparasites. His usual diet was canned cat food, plus cooked ham, chicken and tuna.
Previous treatment had included intravenous fluids, maropitant, clavulanate-potentiated amoxicillin and ranitidine. After this treatment, he had initially vomited less and was brighter. A feline pancreatic lipase immunoreactivity test for pancreatopathy had been negative. He then vomited a large amount of greenish bile-stained fluid several times and became lethargic and was referred to a specialist centre.
Clinical tip on histaminergic H2 blockers
Ranitidine, unlike cimetidine, has a gastrointestinal promotility effect by inhibiting acetylcholinesterase inhibitors and is used in some cases for this effect. It also is reported to produce fewer adverse drug interactions, have less systemic toxicity and greater potency than cimetidine. Cimetidine is the only H2 blocker which inhibits the P450 enzymes in the liver, causing the metabolism of other drugs to be decreased. Cimetidine induced leukopaenias and thrombocytopaenia have also been reported.
Clinical tip on maropitant use in cats
While maropitant is not approved in cats (at the time of writing), studies have shown that at 1.0 mg/kg it is highly effective in preventing motion-induced emesis in cats.
These studies indicate that the NK-1 receptor antagonist maropitant is well tolerated, safe and has excellent anti-emetic properties in cats.Physical examination
On physical examination the cat was quiet but alert. He was in slightly thin body condition (body condition score 4/9) and appeared well hydrated. His mucous membranes were pink and his capillary refill time was less than 2 seconds. Thoracic auscultation revealed a heart rate of 185 beats per minute with matched pulses. Heart and lung sounds and percussion and compression of the thorax were unremarkable. The cat appeared to be uncomfortable on abdominal palpation. His respiratory rate was normal at 32 breaths per minute. Rectal temperature was 38.9° C.
Problem list and discussion of problems
The cat’s primary problem was vomiting; the decreased appetite, weight loss and abdominal discomfort were thought to be related to the vomiting.
Differential diagnosis
Differential diagnoses for vomiting in this cat included:
• Disorders of the stomach
• foreign body
• gastritis
• ulceration
• chronic partial dilation-volvulus
• neoplasia
• Disorders of the small intestine
• foreign body
• inflammatory bowel disease
• neoplasia
• parasites
• intussusception
• Disorders of the large intestine (although there was no history consistent with large intestine disorders)
• colitis
• obstipation
• Systemic disorders
• pancreatopathy
• hypoadrenocorticism
• diabetes mellitus
• liver disorders
• peritonitis
• renal disease/uraemia (unlikely)
• Dietary causes
• dietary sensitivity
• dietary indiscretion
Case work-up
As this cat was clinically unwell, a dietary food trial was not appropriate.
Minimum data base
Haematology results were within the reference ranges. Serum chemistry results showed decreased potassium of 3.0 mmol/l (reference range 3.5-5.8 mmol/l). Other serum chemistry parameters were within the reference ranges.
Urine was not obtained at admission. Intravenous fluid therapy at a rate of 2 ml/kg/hour, with potassium added at 12 mmol/l of fluids, was initiated.Nursing tip on intravenous fluids therapy and potassium supplementation
Moderate or severe hypokalaemia (≤3.0 mmol/l) requires parenteral administration of potassium chloride (KCl) for correction. It is usually recommended that the rate of administration does not exceed 0.5 mmol/kg body weight per hour (1 mEquiv of KCl = 1 mmol KCl). Potassium supplementation is contraindicated in oliguric or anuric states as the kidneys are unable to excrete it. Guidelines for estimating the dose of KCl to add to intravenous fluids are listed in Table 20.1. Remember that Ringer’s solution and lactated Ringer’s contain 4 mmol/l of KCl.
Table 20.1 Amount of potassium chloride (KCl) to add to crystalloid fluids based on the serum potassium (K + ) concentration of the patient. Remember to subtract the amount already in the fluids.
| Serum K+ of the patient in mmol/l | mmol KCl to add per 250 ml of fluids | mmol KCl to add per litre of fluids |
| >3.5 | 5 | 20 |
| 3.0-3.5 | 7 | 28 |
| 2.5-3.0 | 10 | 40 |
| 2.0-2.5 | 15 | 60 |
| 2.0 | 20 | 80 |
Imaging
Abdominal radiographs showed a small intestinal corrugation cranial to the urinary bladder, at the level of the 5th to 6th lumbar vertebrae. There was an abnormal plicated appearance to the small intestine ventral to the descending colon, cranial to and overlying the bladder shadow (L4-6 level) and a small focus of gas within the small intestinal lumen suggested a linear foreign body (Fig 20.1).
Fig 20.1
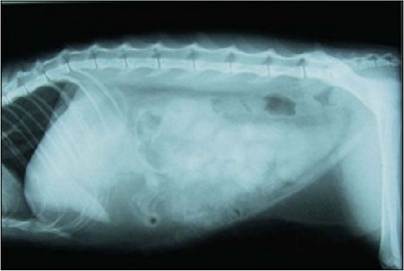
Lateral abdominal radiograph showing small intestine bunched mid-abdomen
(courtesy of Carolina Urraca del Junco)
Abdominal ultrasound also showed plication of the descending duodenum with a linear foreign body evident in the lumen of the duodenum (Fig 20.2). The small intestinal motility appeared to be increased.
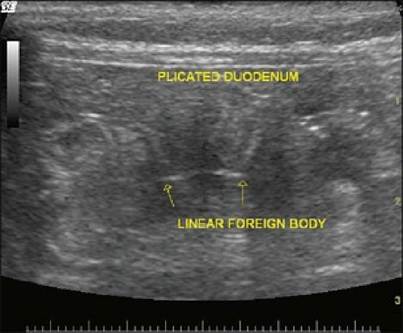
Fig 20.2
Ultrasound picture showing the plication of the small intestine around a linear foreign body
(courtesy of Carolina Urraca del Junco
Treatment
Surgical treatment
The cat was referred to the surgery service for management of a suspected linear foreign body. At surgery, the linear foreign body (thread) was removed by one gastrotomy and four enterotomies. During these procedures, one area of the jejunum perforated at the mesenteric border where the thread had been cutting into the mucosa. The distal two enterotomy sites were excised with adjacent intestine and an end-to-end anastomosis was performed. A more proximal area which appeared to have some compromise to the serosal surface near an enterotomy site had a serosal patch applied.
Follow-up medical treatment
Immediate postoperative treatment included intravenous clavulanate- potentiated amoxicillin (20 mg/kg iv q 8 hours), analgesia with buprenorphine (20 μg∕kg iv q 8 hours), ranitidine (2 mg/kg SQ q 12 hours) for its antacid and promotility effects and intravenous fluids.
Outcome
At 24 hours postoperatively the cat became lethargic, pyrexic and had vomited. A guarded prognosis was given as it was suspected that the patient had injuries to the mucosa along much of his intestinal tract. However, by 4 days post surgery, he was bright and alert and was drinking and eating without assistance. He did not pass faeces until 5 days post-surgery, but they were normal at that time.
His treatments were changed to oral medications and he was discharged on 1 week of oral ranitidine (2 mg/kg po q 12 hours) and clavulanate potentiated amoxicillin (15 mg/kg po q 12 hours). He has continued to do well.Discussion
Often, linear foreign bodies such as pieces of string, cord or fabric will pass through the intestines with few clinical signs; however, if one part lodges within the intestine an obstruction and potentially a perforation will result. Linear foreign bodies most often lodge in the oral cavity or in the pylorus. The free end may eventually come lose from the oral cavity or pylorus and travel to the small intestine. Within the intestine the foreign body causes the intestine to be pleated or bunched up around it. The peristalsis of the intestine causes the pleating. The linear foreign body then abrades the wall of the intestinal loops and eventually multiple perforations and peritonitis occurs.
Linear foreign bodies are more common in cats than in dogs, likely due to cats’ fascination with string and similar objects. Clinical signs include anorexia, vomiting and abdominal pain, as in this young cat and sometimes diarrhoea. If the obstruction is complete, the signs will be acute. If it is a partial obstruction, signs may be more subtle and last for weeks before diagnosis. On palpation of the abdomen, bunched loops of bowel may be felt.
Imaging is often diagnostic as linear foreign bodies produce characteristic signs. On survey radiographs the affected loops of intestine appear gathered or clumped and may be situated to one side of the abdomen. Contrast studies may show the pleating of the intestine. Linear foreign bodies can be difficult to identify on ultrasound, but the corrugated appearance of the intestine may be seen. The small intestinal loops of the intestine proximal to an obstruction may be dilated. In this case the foreign body was actually visible.
In some cases where a linear foreign body is looped around the tongue, it can be cut and allowed to pass through the intestines, which will usually take 1 to 3 days.
This conservative management is contraindicated if the cat shows any gastrointestinal signs or depression or if the cat cannot be monitored very carefully. In one study, 9 out of 24 cats were successfully managed conservatively, with passage of the linear foreign body occurring 1 to 3 days after presentation. The cats that were managed successfully via conservative treatment had a shorter duration of clinical signs before presentation, decreased incidence of abdominal pain, less palpable intestinal plication and less severe haematological abnormalities.Surgery is indicated if there is plication of the intestines or any other indication that the foreign body is not moving through the intestines without damage. At surgery, multiple enterotomies are often necessary to remove the foreign body. Perforated areas of the intestine are repaired and treatment with broad spectrum antibiotics is indicated.
Prognosis
In one study on linear foreign bodies in cats, surgery (gastrotomy and multiple enterotomies) was necessary in 96.9% of the cases and most (83.9%) of the cats so treated did well. Approximately 50% of the cats with linear foreign body-induced bowel lacerations recovered.
More on the topic 20 Linear foreign body in a cat:
- FOREIGN BODY ACCIDENTS
- Oesophageal foreign body in a dog
- 11 A foreign body in the small intestine of a dog
- Foreign Body Periondontitis: Hair Tooth
- Appendix 6A Spurious Negative Quadratic Influence in Estimation Based on Related Linear Equations
- 22 Hepatic lipidosis in a cat
- 19 Pancreatitis in a cat
- 4 Oesophageal stricture in a cat
- 27 Intussusception in a cat
- 39 Colonic inflammatory bowel disease in a cat
- 15 Lymphocytic inflammatory bowel disease/al- imentary lymphoma in a cat
- Cat Scratch Disease (Bartonellosis)
- Foreign bonds
- Microbiology of the Ear o f the Dog an d Cat
- Foreign Material
- Article 6.11 Cat bond investors show their limits
- Foreign Relations
- Foreign Competition, Public Listing, and WTO Entry
- Article 3.1 Foreign investors dump Treasuries at record pace