21 Porto-systemic shunt in a dog
Initial presentation
Vomiting and diarrhoea
Patient details: 14-month-old female entire Cairn terrier, body weight 5.7 kg
Case history
The dog had a history of vomiting digested food about an hour after eating.
The vomiting had been occurring for about a month. Because she did play with sticks the owners had been concerned about a possible gastrointestinal foreign body.She had also had intermittent diarrhoea for the past 6 months. Her stools were occasionally soft, with no blood or mucous present and no straining to defecate. This was thought to most likely be diarrhoea of small intestinal origin.
The owners also reported weight loss over the past several months and episodes of staring vacantly or pacing. When put in her pen in this state she became agitated and starting biting the wires. These episodes lasted about 9 to 10 hours and started post-prandially. The dog was fed a canned specialty puppy food twice a day. She had always been a picky eater and the owners often encouraged her to eat with treats and human food.
The owners did not report that the dog had polydipsia or polyuria, but she had been difficult to house train. She had been an active puppy, but had been quieter during the last couple of months. The dog was de-wormed regularly with fenbendazole and had been vaccinated as a puppy.
She had been to the veterinary surgery previously for the vomiting and had been administered intravenous fluids. She responded to this treatment temporarily, but the vomiting reoccurred the next day after she went home.
Physical examination
On physical examination the dog was alert but quiet. She was in thin body condition with a body condition score of 2/9, but appeared to be adequately hydrated. Oral examination identified an undershot jaw with laterally displaced upper canines. The tongue showed evidence of previous trauma with a V-shaped split to the tongue tip and an erythematous, horseshoe-shaped scar.
Her mucous membranes were pink and moist and her capillary refill time was 2 seconds.Thoracic auscultation was unremarkable. On abdominal palpation the liver could not be identified, but the caudal pole of the left kidney could be palpated easily. Her small intestines were easily palpated and felt normal. She did not show any evidence of discomfort during palpation. Her heart rate was 120 beats per minute, respiratory rate 24 breaths per minute and rectal temperature was 38.7° C.
Problem list and discussion of problems
• Vomiting
• Diarrhoea
• Decreased exercise tolerance • Episodes of abnormal behaviour.
The decreased exercise tolerance was thought to be related to the other disorders and was not addressed separately.
Differential diagnosis
For the vomiting
• Disorders of the stomach
• foreign body
• gastritis
• ulceration
• chronic partial dilatation-volvulus (less likely due to the breed and body shape of the dog)
• neoplasia (less likely, although lymphoma can occur in younger animals)
• Disorders of the small intestine
• foreign body
• parasites
• intussusception
The small intestinal disease differentials below were possible but less likely due to the dog’s young age:
• inflammatory bowel disease
• neoplasia
• Disorders of the large intestine
• colitis
• Systemic disorders
• liver disorders, including porto-systemic shunt
• pancreatopathy
The differentials below were possible but less likely due to the dog’s age:
• hypoadrenocorticism
• diabetes mellitus
• renal disease/uraemia
• Dietary causes
• adverse reaction to food (allergy or intolerance)
• dietary indiscretion
For the chronic small intestinal diarrhoea
• Dietary
• adverse reaction to food: intolerance or allergy
• gluttony - unlikely in this picky dog
• changes of diet
• Gastric disorders, rapid gastric emptying
• Small intestinal disease
• infectious, e.g. bacteria, viral, fungal
• partial obstruction, e.g.
intussusception, foreign body• gastrointestinal parasites
• brush border defects
• Less likely small intestinal disorders due to her age and clinical presentation:
• inflammatory bowel disease
• infiltrative neoplasia (e.g. lymphoma, mastocytosis)
• lymphangiectasia
• Pancreatic disease
• chronic pancreatitis
• exocrine pancreatic insufficiency
• pancreatic neoplasia (less likely due to age)
• Liver disease
• porto-systemic shunt
• bile duct obstruction
• liver failure
• Kidney disease
• Miscellaneous
• congestive heart failure - no signs consistent with this
• immunodeficiencies
• hypoadrenocorticism (less likely at this young age)
As the dog showed no other neurological signs, the abnormal behaviours were most likely to be cerebral in origin, either from the cerebrum itself or extra-cranial disorders affecting brain function. A behavioural problem was also possible but less likely.
For the abnormal behaviours
• Primary brain disorders include:
• congenital diseases such as malformation of the brain or Chiari-like malformation
• hydrocephalus
• inborn errors of metabolism
• granulomatous meningoencephalomyelitis
• intracranial or brain tumours
• epilepsy
• Systemic disorders affecting brain function include:
• Porto-systemic shunts (PSS) causing signs of hepatic encephalopathy (HE)
• hypoglycaemia
• toxins
• nutritional deficiencies or imbalances
Case work-up
The dog was admitted to the hospital for diagnostic investigation.
Minimum data base
Haematology, serum chemistry and routine urinalysis were performed. Results of routine haematology showed a slightly decreased packed cell volume (PCV) of 0.35 l/l (reference range 0.37-0.55 l/l) due to a microcytosis with an mean corpuscular volume (MCV) of 52% (reference range 60-77%). The red blood cell count was within the norm at 5.6 ? 1012∕l (reference range 5.5-8.5 ? 1012∕l) and haemoglobin was slightly low at 11.8 g/dl (reference range 12-18 g∕dl).
Clinical tip on haematology
When the PCV is decreased, check the cell size, i.e. the mean corpuscular volume (MCV). Microcytosis can decrease the PCV while the number of red blood cells stays within the reference range. Microcytosis can occur with iron loss (e.g. with gastrointestinal bleeding), with iron sequestration (as occurs with PSS or anaemia of chronic inflammation) and in some normal Akita dogs.
Serum biochemistry results showed a moderate increase in alanine aminotransferase of 233 IU∕l (reference range 21-102 IU∕l) and in alkaline phosphatase (ALP) of 116 IU∕l (reference range 20-60 IU∕l). The fasting bile acids were markedly increased at 243 μmol∕l (reference range 0-7 μmol∕l) and post-prandial bile acids rose to 521 μmol∕l. Serum albumin was at the lower end of the reference range at 22.3 g/l (reference range 26-35 g/l) and urea was also at the lower end of the reference range at 1.9 mmol/l (range 1.7-7.4 mmol/l).
Basal serum cortisol concentration was assessed to screen for hypoadrenocorticism and was within the reference range at 221 nmol/l (reference range 20-230 nmol/l). A coagulation profile was performed in case liver biopsies were required; the prothrombin time, activated partial thromboplastin time (APTT) and fibrinogen were all within reference ranges.
Clinical tip on coagulation profiles in dogs with porto-systemic shunts
While this dog’s coagulation profile was within the reference range, serious post-operative haemorrhage has been reported in dogs after closure of congenital porto-systemic shunts (PSS). Dogs with PSS often have lower platelet counts, lower activity of clotting factors II, V, VII and X, and increased factor VIII and APTT compared to healthy dogs. Surgical attenuation of the shunt results in increased frequency of abnormalities in coagulation times and factors immediately after surgery and there may be a risk of bleeding. Haemostasis does become normal in dogs where there is complete attenuation of shunting, in contrast to dogs with persistent shunting.
Urinalysis showed a urine specific gravity of 1.008. The chemical strip showed a pH of 6.5 and the sediment showed urate crystals.
Imaging
Abdominal radiographs showed a small liver size and the kidneys appeared to be large.
Abdominal ultrasonography supported the liver being small in size. The hepatic veins were small and a single extrahepatic PSS was iden-
tified, curving round the caudal pole of the right kidney and coursing Craniodorsally to enter the caudal vena cava close to the entry site of the right renal vein (Fig 21.1). Doppler ultrasound was used to confirm the presence of blood flow within the shunt (Fig 21.2). The kidneys were both enlarged at 6 cm and small calculi were identified within the urinary bladder; as there were urate crystals present in the urinalysis, these were presumed to be ammonium urate in origin.
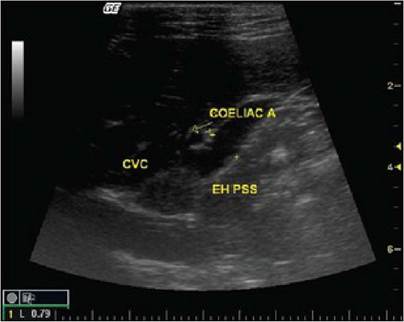
Fig 21.1
Ultrasound picture showing a large extrahepatic portocaval shunt
(coelic a, coelic artery; EH PSS, extrahepatic porto-systemic shunt; CVC, caudal
vena cava)
(courtesy of Carolina Urraca del Junco)
Fig 21.2
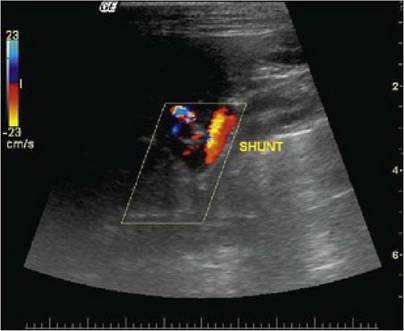
Ultrasound of colour Doppler showing blood flowing through the extrahepatic porto-systemic shunt
(courtesy of Carolina Urraca del Junco)
Clinical tip on imaging for PSS
Computed tomography can be useful to better determine the location of a shunting vessel, but was not used in this case. Transplenic portal scintigraphy has also been used as a diagnostic aid in some cases. Many surgeons like the portogram to be performed prior to surgery as this gives them information about the location of the shunting vessel so they can plan their surgical approach.
Case assessment
From the history, clinicopathological results and imaging a diagnosis of extrahepatic PSS was made.
Clinical tips
Microcytosis can lower the PCV as the smaller cells result in a lower percentage of the blood being cellular.
Causes of microcytosis include iron deficiency and PSS. The reason for the microcytosis in animals with PSS is thought to be due to iron sequestration or ineffective iron transport, which have been proposed as the causes of iron deficient erythropoiesis.Serum urea is often at the low end of or below the reference range in animals with PSS as ammonia is not being efficiently converted to urea within the liver. Hypoglycaemia can be seen in some cases and should be addressed therapeutically.
Urate crystals are found in many dogs with PSS due to hyperammonaemia and a decreased ability of the liver to convert uric acid to allantoin.
The presence of urate crystalluria is never normal and should prompt the clinician to look for PSS or other hepatic disorders. Some Dalmatian dogs also have urate crystals in their urine due to an inborn metabolic defect and they may form urate uroliths.
Many animals with PSS also have a low urine specific gravity and may present for polyuria/polydipsia. This poor urine concentrating ability may be due in part to decreased medullary tonicity from the low urea, increased adrenocorticotrophin hormone (ACTH) secretion and hypercortisolism, and there also appears to be a possible decrease in the synthesis or release of antidiuretic hormone from the pituitary for reasons that are not fully elucidated.
Nursing tip
As high protein diets can worsen clinical signs, animals with suspected PSS should be fed protein restricted diets, e.g. 15 to 20% protein on a dry matter basis or 2 g of protein/kg/day to decrease ammonia formation from colonic bacteria. If a puppy is still growing, commercial low protein diets designed to decrease the risk of HE may be too low in protein to support growth (22% protein on a dry matter basis). In that case, supplement the diet with cottage cheese at 100 g per 400 g of canned dog food. Cottage cheese is high in branched chain amino acids and has less tendency to cause encephalopathic problems than meat proteins. Vegetable proteins or soy proteins are also less likely to cause problems than meat proteins and can be used. These patients should also be fed small meals frequently, as that decreases the risk of hypoglycaemia.
Initial (pre-surgical) medical management
Initial medical treatment to decrease signs of HE were started as soon as the diagnosis was made. This included dietary management as mentioned above plus oral lactulose syrup (1 ml po q 12 hours). The dose was adjusted so that the faeces were soft but formed, as an overdose can cause diarrhoea. Metronidazole was started at 7 mg/kg po q 12 hours.
Clinical tip on HE treatment
Lactulose decreases intestinal transit time and acidifies colonic content which aids in trapping ammonia in the colon and decreasing absorption. In cases with severe signs of HE, lactulose enemas may be helpful. Oral antibiotics such as metronidazole, ampicillin or neomycin may be given to decrease intestinal urease-producing bacteria, although low dosages are recommended, e.g. 7 mg/kg metronidazole po q 12 hours.
One-third of animals do well with medical management alone, especially dogs which are older at diagnosis; however, over half of dogs treated with medical management alone undergo euthanasia within the first year after diagnosis.
This patient was sent home for 3 weeks on a low protein diet with cottage cheese supplementation, lactulose at 2 ml po q 12 hours and ampicillin (10 mg/kg po q 8 hours) to stabilize her HE and improve her body condition prior to surgery. She was then readmitted for placement of an ameroid constrictor on the shunting vessel and liver biopsy.
Surgical treatment
Surgical treatment is recommended in most patients with PSS to improve long-term outcome. There are several methods of occluding the shunt, including gradual occlusion with ameroid constrictors, cellophane banding, embolism with coils and suture ligation. The traditional surgical treatment involved placement of a ligature around the anomalous vessel, which is gradually tightened during the surgical procedure while measuring portal pressure and observing the splanchnic viscera. If the ligature is placed too tight, there is a significant risk of inducing portal hypertension, a severe and often fatal post-operative complication. Up to 68% of dogs with single extrahepatic PSS cannot be completely ligated and surgery results in partial shunt attenuation. Partial PSS attenuation is associated with an increased risk of persistence or recurrence of clinical signs. Recurrence of clinical signs is reported in 32 to 50% of partially ligated and 0 to 12% of completely ligated extrahepatic PSS. Therefore, gradual rather than acute occlusion of PSS is advocated as a surgical technique. Theoretically, this allows development of the portal circulation and hepatic architecture in response to the increased vascular supply, while reducing perioperative complications associated with portal hypertension.
The ameroid ring constrictor used in this case (Figs 21.3 and 21.4) is commonly used for gradual PSS attenuation, although actually it produces a delayed acute reduction in blood flow associated with vascular thrombosis rather than the gradual attenuation it was originally thought to cause. The clinical results of ameroid constrictor placement in dogs with single extrahepatic PSS is much better than in dogs with intrahep- atic PSS.
Fig 21.3

Ameroid constrictor
(courtesy of Dr Donald Yool)
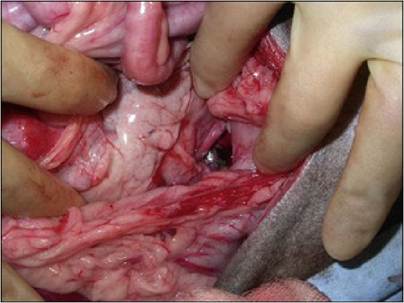
Fig 21.4
Ameroid constrictor in position in a dog with an extrahepatic porto-systemic shunt
(courtesy of Dr Donald Yool)
Post-operative care
Post-operative care included monitoring for hypothermia, hypoglycaemia and especially for signs of portal hypertension. Occlusion of the shunting vessels forces blood through the liver, opening previously closed vessels and some cases do not tolerate this very well. Signs of portal hypertension include an increasing abdominal effusion. If evidence of portal hypertension had been present, treatment with intravenous colloids would have been tried, although many of these dogs need to return to surgery to have the constriction lessened or removed.
Medical management was continued after surgery for 7 weeks; once serum bile acid concentrations were within the reference range, indicating improved liver function, the dietary protein was gradually increased.
Nursing tips on diet after surgery for PSS
The adult canine requirement for protein is not high (18% dry matter basis), so it may be satisfactory for the dog to remain on a moderately restricted protein diet. Especially in dogs which continue to have some shunting of the vessel a moderately restricted protein diet may be beneficial.
Follow-up
The dog recovered well from the surgery, although she was rather lethargic for the first few days. Difficult or slow recovery from anaesthetic drugs is common in dogs with hepatic compromise.
The histopathology results for the liver biopsy taken at surgery showed periportal arteriolar and biliary duplication with lobular atrophy and lipogranulomas and marked diffuse hepatocellular fatty change. These changes are all consistent with a PSS and correlated well with the clinical and surgical findings. The degree of abnormality was thought to explain the poor body condition and neurological signs.
At the 7 week recheck the dog was very bright and there had been no further episodes of vomiting, diarrhoea or neurological problems. Haematological and serum chemistry parameters were within the reference ranges and at ultrasound scan the ameroid constrictor was still in place and occluding the vessel. The urate cystic uroliths were not detected on ultrasound. The restricted protein plus cottage cheese diet was continued while the lactulose and ampicillin were discontinued.
Pathophysiology
In the embryonic dog, the ductus venosus carries oxygenated placental blood to the circulation, bypassing the hepatic circulation. This vessel normally closes within the first 1 to 2 weeks after birth. Abnormal patency of this vessel or other abnormal vasculature formation connecting the portal venous system to the systemic circulation result in the signs seen in PSS. Congenital shunts are generally one vessel, whereas shunts acquired due to liver disease (e.g. cirrhosis and fibrosis) are more often multiple.
Common types of shunts include intrahepatic porto-caval shunts and extrahepatic porto-caval (Fig 21.5) or portal-azygos shunts.
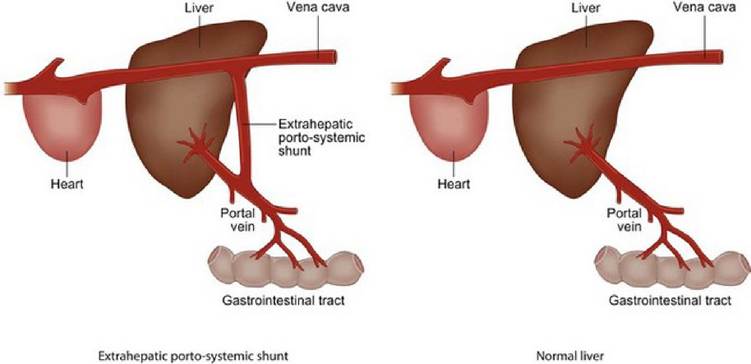
Fig 21.5
A liver with an extrahepatic porto-systemic shunt and a normal liver.
The degree of change in the hepatic histology is probably a function of the amount of portal blood that is diverted from the liver and may vary between liver lobes depending of the site of the shunt vessel, particularly with intrahepatic shunting associated with a persistent ductus venosus. Typical histopathologic changes in the liver include arteriolar hyperplasia, loss of portal vein profiles and hepatocellular atrophy with increased lipogranuloma formation. Similar histopathological changes can also be found in cases of hepatic microvascular dysplasia, only in those cases no shunting vessel is found. Pathologic changes may be present in the central nervous system, especially in encephalopathic animals.
Since the liver relies on a substantial amount of nourishment from the portal circulation, decreased blood flow and subsequent decreased nourishment results in hepatic atrophy. Decreased insulin supply due to the shunting may also contribute to atrophy since insulin aids in the development of hepatic parenchyma. Atrophy of the liver further reduces hepatic function.
Gastrointestinal signs are seen in about 30% of dogs with PSS and include vomiting, diarrhoea and anorexia. Other signs often seen include poor growth and abnormal neurological behaviours, as in this case. High portal pressure is not usually a feature of PSS, so abdominal effusion does not usually develop unless the serum albumin is very low and a transudate forms due to decreased oncotic pressure.
An increase in plasma cortisol is common in dogs with PSS and may account for the elevations in ALP levels and hepatic hydropic degeneration as well as the polydipsia/polyuria. Increased plasma cortisol is thought to be due to dysregulation of pituitary ACTH secretion by GABAergic mechanisms. Hypercortisolaemia regresses with correction of the shunt.
Epidemiology
Congenital PSS has been reported in 0.18% of all dogs and 0.05% of mixed-breed dogs. The proportion of diagnoses of congenital PSS has increased from 5 in 10,000 dogs in 1980 to 5 in 1000 dogs in 2001. In one study, the greatest numbers of shunts were found in Havanese (3.2%), Yorkshire terriers (2.9%), Maltese (1.6%), Dandie Dinmont terriers (1.6%) and Pugs (1.3%). In another study of 242 cases from Australia, breeds that were significantly over-represented included the Maltese terriers, Silky terrier, Australian cattle dog, Bichon Frise, Shih Tzu, miniature schnauzer, Border collie, Jack Russell terrier, Irish wolfhound and Himalayan cat. Bichon frises with shunts were significantly more likely to be female than male.
Congenital PSS appears to be hereditary in Yorkshire terriers, but the exact mechanism of inheritance has not been elucidated. In Cairn terriers, extrahepatic shunts are inherited as an autosomal trait with variable expression. Familial lines with increased incidence of PSS have been reported in miniature schnauzers, Irish wolfhounds and old English sheepdogs. Multiple extrahepatic PSSs have been found in related female American cocker spaniels and breed predispositions for multiple extrahepatic shunts include the German shepherd dog and Doberman pinscher.
Single intrahepatic shunts are most commonly found in large breed dogs such as Irish wolfhound, old English sheepdog, golden and Labrador retrievers and Samoyed and in medium-sized breeds such as Australian shepherd dogs and Australian cattle dogs.
Most dogs with PSS are diagnosed at less than 2 years of age, although sometimes the signs are subtle and the cases are not brought in for veterinary attention until they are older. Intrahepatic PSS may occur more commonly in male dogs than in female dogs.
Prognosis
Nearly one in five dogs has a seizure after shunt ligation, for reasons not yet well understood. Treatment has been tried with intravenous phenobarbitone or continuous infusion of propofol (0.025-1 mg/kg/minute) for 12 to 24 hours. Prognosis is poor for animals with seizures post-op- eratively.
In one study of dogs treated for single extrahepatic shunts with an ameroid constrictor post-operative mortality rate was 7.1%. Predictive factors for post-operative death included high preoperative WBC count and post-operative complications such as seizuring. In another study using silk ligatures to close the shunting extrahepatic vessel, short-term and long-term mortality were 27% and 2.9%, respectively. Clinical recurrence occurred in 10% of dogs. The degree of closure was significantly associated with mortality, but not with clinical recurrence. The preoperative size of the liver (in relation to the dog’s weight) also appears to be an indicator of prognosis, with the greater the liver size, the better the prognosis.
Twenty-one percent of dogs after surgery using ameroid constrictors and three of 10 dogs using ligatures had continued shunting. Predictive factors for persistent shunting included low preoperative plasma albumin concentration, high portal pressure after complete occlusion and high portal pressure difference (post-occlusion minus baseline).
In a study of 168 dogs with single extrahepatic shunts treated by placement of an ameroid constrictor, there was a low prevalence of postoperative complications (10%); the most common complications were seizures, ascites and haemoabdomen. The prophylactic use of an anticonvulsant drug, such as potassium bromide, is recommended by some clinicians in dogs undergoing PSS surgery. Twenty-one percent of dogs had continued porto-systemic shunting, usually associated with the development of multiple extrahepatic shunts, though many dogs with persistent shunting were clinically normal. The long-term outcome was classified as excellent in 80% of dogs, good in 14% and poor in 6%.
More on the topic 21 Porto-systemic shunt in a dog:
- Systemic Sclerosis
- 38 Colorectal neoplasia in a dog
- SYSTEMIC RISK EXPOSURES AND LOSSES
- 14 Hypoadrenocorticism in a dog
- 16 Ingestion of glue by a dog
- 33 Intestinal leiomyoma in a dog
- SYSTEMIC RISK AND PORTFOLIO DIVERSIFICATION
- COUNTERPARTY SYSTEMIC RISK
- 11 A foreign body in the small intestine of a dog
- Systemic Antimicrobials
- Systemic Relevance of Financial Institutions
- 12 Chronic partial gastric dilatation in a dog
- 13 Pancreatitis and alimentary lymphoma in a dog