11 A foreign body in the small intestine of a dog
Initial presentation
Vomiting and poor appetite
Signalment: 5-year-old male English springer spaniel, body weight 19.9 kg
Case history
The dog had been healthy until 2 weeks prior to admission.
He was dewormed regularly with fenbendazole and vaccinated yearly. Two weeks prior to admission he had started vomiting and had a progressive decrease in appetite. He was now vomiting 2 to 3 times per day and the vomitus included food and bile but no blood. The dog’s stools had been normal. The owner estimated that the dog had lost about 1 to 2 kg over this time period. The dog’s water intake and urine output had not changed, but his exercise tolerance had decreased.His usual diet was a mixture of dry and canned dog food and recently the owners had been hand feeding him with chicken and ham to encourage food intake. He was normally fed twice a day.
Physical examination
The dog was dull but responsive. His body condition score was 4/9. There was evidence of recent weight loss, with signs of muscle and fat loss over the lumbar and flank areas. Mucous membranes were pink but slightly
tacky; capillary refill time was less than 2 seconds. Peripheral lymph nodes felt normal.
Thoracic auscultation revealed normal heart and lung sounds, with a heart rate of 140 beats per minute and a respiratory rate of 24 breaths per minute.
There was no evidence of pain on abdominal palpation and the only abnormality found was increased gas in the small intestines. Rectal temperature was 39.1° C.
His prior treatment included clavulanate-potentiated amoxicillin, ranitidine and sucralfate (doses unknown), with no improvement in clinical signs. He was on no other medications or supplements.
Problem list and discussion of problems
• Vomiting
• Tacky mucous membrane
• Poor appetite
• Weight loss
• Increased intestinal gas
• Raised body temperature
Differential diagnosis
Vomiting is the primary complaint and the other problems were thought to be related to the vomiting.
The differential diagnoses for the vomiting in this dog include:• Disorders of the stomach
• foreign body
• gastritis
• ulceration
• chronic partial dilation-volvulus
• neoplasia
• Disorders of the small intestine
• foreign body
• inflammatory bowel disease
• neoplasia
• parasites
• intussusception (unlikely)
• Disorders of the large intestine
• colitis
• obstipation
• Systemic disorders
• pancreatopathy
• hypoadrenocorticism
• diabetes mellitus
• liver disorders
• peritonitis
• renal disease/uraemia (unlikely)
• Dietary causes
• dietary sensitivity
• dietary indiscretion
Most dogs (80%) with intussusception are less than 1 year of age, although it was still a possibility. He did not have any other signs of renal disease, so uraemia was an unlikely cause of the vomiting.
The slightly tacky membranes were likely indicative of mild dehydration. The dog had not drunk water that morning, had a 2-hour journey to the clinic and was also probably losing fluid in his vomitus.
Case work-up
The dog was admitted to the hospital and administered intravenous crystalloid fluids containing potassium, at a rate to correct 6% dehydration.
Minimum data base
Haematology, serum chemistry and routine urinalysis were performed. Haematology results were unremarkable, although a packed cell volume of 0.47 l/l (reference range 0.37-0.55 l/l) is high in breeds of dogs other than sighthounds. This was thought to likely be due to haemoconcentration.
Serum chemistry showed an increase in liver enzymes, with alanine aminotransferase (ALT) at 1100 IU∕l (reference range 21-102 IU∕l) and alkaline phosphatase at 114 IU∕l (reference range 20-60 IU∕l). Serum chloride and sodium were decreased at 84 mmol/l (reference range 99-115 mmol/l) and 137 mmol/l (reference range 139-154 mmol/l), respectively, and potassium was at the bottom end of the reference range at 3.6 mmol/l (reference range 3.6-5.6 mmol/l).
A basal cortisol was performed and was within the reference range at 97 nmol/l (reference range 20-230 nmol/l). If basal cortisol is greater than 70 nmol/l, hypoadrenocorticism is unlikely.Serum amylase and lipase were not elevated, making a pancreatopathy less likely, although a test for canine pancreatic lipase immunoreactivity was not performed.
Urinalysis was unremarkable. The urine specific gravity was 1.048, consistent with good renal concentrating ability and also with the mild dehydration detected clinically.
Serum albumin, urea and creatinine can also be increased due to dehydration, although they were within the reference ranges in this dog.
Imaging
Barium impregnated polyethylene spheres (BIPS) were administered to the dog as an intestinal obstruction was considered to be likely. BIPS aid in diagnosing partial obstructions as the large (9 mm) BIPS will persistently bunch at the site of an obstruction.
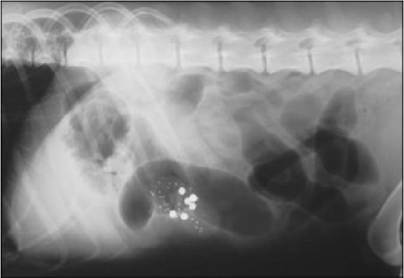
Ventrodorsal and lateral abdominal radiographs were taken about 8 hours later. These showed bunching of the BIPS and very large gas filled loops of small intestine (Figs 11.1 and 11.2). Some areas of the intestine were greater than twice the height of the vertebral body of L5 in width. This pattern is highly suggestive of small intestinal obstruction, so the dog was sent for an exploratory laparotomy.
Figs 11.1
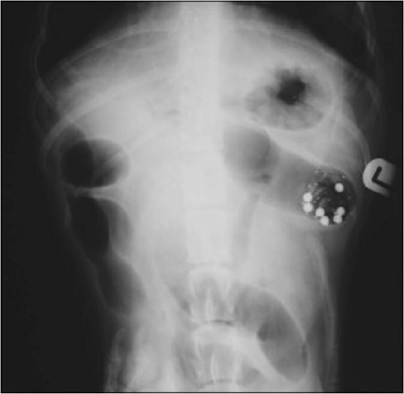
Figs 11.1 and 11.2
Lateral and ventrodorsal radiographs showing grouping of BIPS and grossly dilated intestines characteristic of intestinal obstruction
(courtesy of Dr Tobias Schwarz)
Surgery
At surgery the intestines were dilated with gas and a foreign body was located within the jejunum (Fig 11.3). A peach stone was removed from the mid-jejunal area. Closure was routine and omentum was wrapped around the enterotomy site.
Recovery was uneventful and a postoperative antibiotic (clavulanate-potentiated amoxicillin, initially at 20 mg/kg iv q 8 hours for the first day, then 19 mg/kg po q 12 hours for 4 days) was administered. Buprenorphine (20 μg∕kg iv q 6 hours) was used for postoperative analgesia for the first day.Fig 11.3

Small intestinal foreign body
(courtesy of Dr Donald Yool)
Follow-up
Five days postsurgery the serum chemistry values had improved with the ALT decreased to 290 IU/l and the AP decreased to 244 IU/l. Electrolytes were within the reference ranges. The dog had begun to eat, rectal temperature was normal; he was not vomiting and was discharged with no further medical treatment.
Discussion
The radiographs were highly suggestive of the presence of an intestinal foreign body in this dog. The use of the BIPS added to the interpretation of the radiographs, although it would likely to have been possible to make the diagnosis without them. Peach pits are a fairly common canine intestinal foreign body and are not usually clearly radiopaque on plain films.
The low serum sodium and chloride and borderline potassium are consistent with intestinal obstruction and may be due to loss in the vomit- us and/or sequestration within the intestines. Due to the dilation of the bowel cranial to the obstruction and the congestion of mesenteric blood vessels (Fig 11.4), after about 24 hours of obstruction the intestinal mu-
cosa cranial to the obstruction secretes instead of absorbing fluids, although it is still able to absorb nutrients.
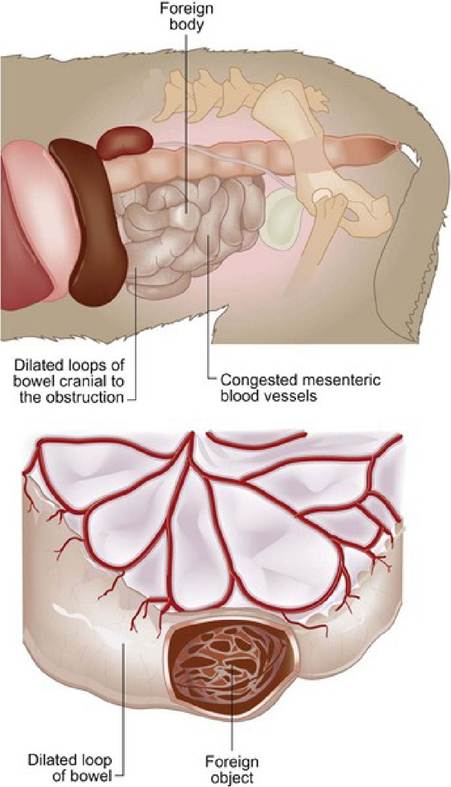
Fig 11.4
An intestinal foreign body causes dilatation of the bowel cranial to the obstruction, sometimes termed a ‘stagnant’ loop of bowel
Colloids may have been a better fluid choice as they support oncotic pressure more effectively in dogs with intestinal obstruction than do crystalloid fluids, although there is no evidence that the use of colloids increases survival rates.
Bacterial numbers increase in obstructed intestinal segments and can result in endotoxic shock. This dog did not appear to be in shock, but he did have an elevated body temperature. The use of antibiotics is indicated in obstructed animals to decrease the bacterial load and help prevent bacterial intestinal translocation and endotoxaemia.
Epidemiology
In one study, English bull terriers, springer spaniels, Staffordshire bull terriers, Border collies and Jack Russell terriers were over-represented in presenting for gastrointestinal foreign bodies. In dogs, 63% of obstructions occurred in the jejunum but foreign objects were encountered at all points along the gastrointestinal tract.
Prognosis
A longer duration of clinical signs, the presence of a linear foreign body and multiple intestinal procedures are associated with significantly increased mortality. Neither the degree of obstruction (partial or complete) nor the location of the foreign body has been shown to have a significant influence on survival. In a study in cats, those without preoperative perforation from a foreign body have an 85% chance of survival while those with preoperative perforation have only a 50% chance of survival.