10 Vomiting
Pathophysiology of vomiting
Vomiting is a reflux of food and fluid from the stomach. It is a reflex act that involves prodromal signs of nausea, which may include anxiety, salivation, lip licking and restlessness.
Prior to vomiting, reverse peristalsis moves intestinal contents into the stomach and the animal begins to retch. There are then gastric antral and retrograde antral contractions with relaxation of the body of the stomach. The gastro-oesophageal and pharyngo-oesophageal sphincters relax. The driving force of vomiting is the contraction of the abdominal muscles and the diaphragmatic muscles.
Vomiting is a reflex act resulting from stimulation of the vomiting centre in the brain stem (Fig 10.1). The vomiting centre receives afferent input from peripheral receptors in the viscera from the chemoreceptor trigger zone (CRTZ) in the floor of the fourth ventricle of the brain, from the vestibular apparatus and from the higher centres of the brain such as the cerebral cortex. The peripheral visceral receptors are located throughout organs in the body, especially in the duodenum, sometimes referred to as ‘the organ of vomition or nausea’. Distension or irritation of the intestinal mucosa may stimulate the vomiting centre and inflammation of other organs such as the pancreas can also result in vomiting. Afferent nerve fibres run from these organs in the vagal and sympathetic nerves.
Fig 10.1
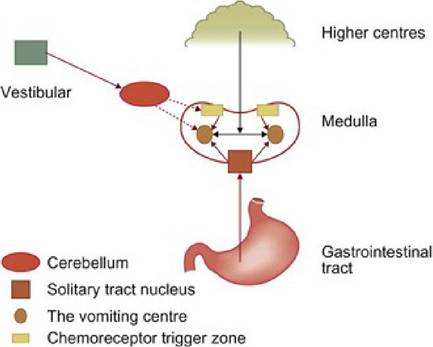
The vomiting centre
The CRTZ is on the floor of the fourth ventricle and mediates vomiting from toxins such as those present in uraemia and also vomiting associated with some drugs, e.g. apomorphine or xylazine.
The vestibular apparatus mediates vomiting due to motion sickness or vestibular disease. Stimulation of the higher centres such as the cerebral cortex from acute stress may result in vomiting, although this may be more common in human beings than in animals.
Diagnosis of vomiting
Several questions need to be answered early in the approach to vomiting cases. First, is it vomiting or regurgitation? Second, is the vomiting due to gastrointestinal (GI) disorders or due to disorders of other body systems? The signalment, history and physical examination often provide clues to these answers.
Signalment and history
The patient’s ‘signalment’ is the age, breed and sex. Knowing these factors often increases (or decreases) the index of suspicion for some disorders and helps the clinician order the differential diagnoses list.
The history should include the progression of the vomiting, the frequency, the timing with regards to eating and the time of day the vomiting most often occurs. Vomiting more than 12 hours after eating indicates delayed gastric emptying. Vomiting bile early in the morning can be part of the ‘bilious vomiting syndrome’ in dogs. A description of the contents of the vomitus, e.g. bile, foam, digested food, bright red blood or digested blood ‘coffee grounds’, is useful.
Careful questioning can usually allow the veterinary surgeon to determine if the patient is vomiting or regurgitating, although some cases do show both signs. Vomiting is the forceful ejection of gastric contents from the stomach, while regurgitation is the expulsion of ingesta from the oesophagus or pharynx. Regurgitation is described as a passive event; however, gagging may be present which can result in retching. With regurgitation, the animal should not show nausea, but drooling can be present if swallowing is impaired. Regurgitated food usually does not contain bile and should not have an acidic pH (unless refluxed from the stomach into the oesophagus). It is more common for animals to ‘re-eat’ regurgitated food than vomited food. Regurgitated food often appears undigested and may have the shape of the oesophagus. Regurgitation may take place immediately after eating, but can occur hours after eating, especially in cats where the normal oesophageal motility is slow.
Vomiting is usually accompanied by signs of nausea and a forceful ejection of food, with an abdominal effort present. The pH of vomitus may be acid, but can be alkaline, especially if duodenal contents are present. Expectoration - the ejection of material from the airway and laryngopharyngeal area - is also a forceful act and must be differentiated from vomiting and regurgitation. Expectoration and regurgitation are what cats do to remove hairballs from the laryngopharynx and oesophagus.
Environmental history should provide information regarding access to toxins such as lead, houseplants, cleaners, floor finishes, deodorants and organophosphates. The history of medication administered is important as many drugs can cause vomiting, e.g. non-steroidal anti-inflammatory drugs, corticosteroids, digitalis and some antibiotics. Asking questions regarding playing with toys, sticks, stones and string are important for possible foreign body ingestion, especially in young animals and retrievers.
During the history taking, particular attention should be paid to the diet, including information about scavenging, treats, snacks and food provided by neighbours or children. When questioned carefully, many owners provide evidence of a dietary influence on the patient’s vomiting. A review of all body systems is always necessary. Anything that incites or exacerbates the signs should be noted, as well as abnormal posturing that may reflect abdominal pain.
Physical examination
A complete physical examination is always necessary, including a thorough abdominal palpation. Examination of the teeth can sometimes indicate if a dog is a rock chewer and could have swallowed a stone. The underside of the tongue should be examined for string or other linear foreign bodies. The neurological status should be noted, as some neurological diseases can result in vomiting. Dehydration should be assessed. If the history is consistent with insufficient fluid intake and vomiting, dehydration is estimated to be at least 5% regardless of physical signs (i.e.
subclinical dehydration). A rectal examination may reveal diarrhoea, melaena or haematochezia.Work-up
If the vomiting is chronic and the animal is not ill and is eating well, a 1-month dietary trial with a restricted novel protein may be tried. Either a homemade or a commercial diet may be used. In dogs that have a history of early morning bilious vomiting, a late night snack or meal may reduce the vomiting. Some of these dogs are also helped by an evening dose of oral metoclopramide, although motility modifying drugs such as metoclopramide should not be used prior to ruling out foreign bodies. Ideally all animals at least have a minimum data base performed.
Minimum data base and other laboratory data
In most cases of chronic vomiting, further work-up is necessary. Causes of vomiting may be divided into those which are directly caused by GI disorders and those that are caused by disorders of other body systems. The minimum data base aids in deciding if a primary GI disorder or a non-GI disorder causes the vomiting. The initial diagnostic work-up includes haematology, serum chemistry, urinalysis and faecal flotation. If there is any indication of dehydration, parenteral fluids should be administered, as oral rehydration may not be effective.
Haematology is useful for detection of infection, toxaemia, eosinophilia associated with eosinophilic gastritis, parasitism, mastocytosis or hypoadrenocorticism, lead toxicosis, blood loss and determination of hydration status. A buffy coat smear may show mast cells in cases of mastocytosis, but normal animals may also have mast cells in their buffy coat, so this is not specific for mastocytosis.
Serum chemistry provides information about possible protein-losing enteropathies, azotaemia, liver disease, hypoadrenocorticism, diabetes mellitus, hydration status and electrolyte concentrations. A serum basal cortisol of greater than 70 μmol∕l (or 2 μg∕dl) makes hypoadrenocorticism unlikely.
Determination of serum amylase and lipase may provide an indication (albeit neither sensitive nor specific) of pancreatitis in canine patients. In acute pancreatitis, serum trypsin-like immunoreactivity (TLI) will be increased and may aid in the diagnosis. Tests specifically for serum canine and for feline pancreatic lipase immunoreactivity (cPLI and FPLI, respectively) are more highly sensitive and specific tests for pancreatitis than total serum lipase.
Puppies and kittens with congenital porto-systemic shunts (CPSS) may present with GI signs. Some of the clinicopathological changes associated with CPSS include microcytosis, decreased albumin and increased liver enzymes, although values of these parameters within the reference ranges does not rule out CPSS. A bile acid stimulation test should be performed whenever there is a possibility of CPSS. (Copper coloured irises in cats are nearly pathognomonic for this disorder.)
In older cats, a serum total T4 (thyroxine) should be taken to rule out hyperthyroidism. Over 50% of cats with hyperthyroidism may present with vomiting.
Determination of serum total carbon dioxide (TCO2) can be useful. An increase in TCO2 indicates alkalosis (as opposed to increased PCO2, which indicates acidosis). Alkalosis in a vomiting small animal patient (who has not been administered alkalinizing agents such as sodium bicarbonate) nearly always means a pyloric or duodenal obstruction. Look for a foreign body!
Urinalysis provides information about renal and liver diseases, ketoacidosis, glucosuria and hydration. If possible, at least two drops of urine should be collected whenever initial serum chemistry is performed for chemical strip analysis and urine specific gravity. Ideally 5 to 10 ml should also be collected and centrifuged for a sediment examination.
Faecal examination for ascarids may be helpful, especially in puppies and kittens. De-worming with an effective agent such as fenbendazole would be recommended in some cases, even if parasite ova are not detected, as some parasites shed eggs only intermittently.
Ollulansus tricus- pis can cause vomiting in cats (and rarely in dogs) and is best diagnosed by a Baermann examination of the vomitus rather than faecal examination.Further tests useful in some cases
Serum lead concentrations should be measured if there is a history consistent with lead ingestion, e.g. remodelling of an older house or neurological or behaviour signs associated with the vomiting. Plasma cholinesterase can be measured if history and clinical signs indicate possible organophosphate toxicity. Cats from areas endemic for Dirofilaria immit- is heartworms should have a serologic test for D. immitis antigens and a thoracic radiograph, as this disease may present as vomiting in the cat.
Imaging
Survey (plain) radiographs of the abdomen are essential for any animal with chronic vomiting. They are used to look for radio-opaque foreign bodies, intestinal dilation, gastric size, position and content, liver and kidney size, uterine size (i.e. for pyometra), abdominal masses and bowel perforations. In cats, congestive heart failure can also cause partial anorexia and vomiting, so thoracic radiographs should be taken if the clinical examination indicates cardiac abnormalities.
Contrast radiography
Liquid gastrograms with barium or with iodinated compounds if a perforation is suspected may be useful for detection of gastric masses, gastric or intestinal foreign bodies, identifying the size and shape of the stomach and estimating the size of the liver. If enough barium is used, mucosal detail can be evaluated. Liquids and solids empty from the bowel differently, so liquid barium gives no information about most gastric motility disorders.
Barium mixed with a meal gives some indication of gastric emptying, which should begin within 30 minutes of ingestion. The barium may separate from the meal and be emptied separately as a liquid.
Barium impregnated polyethylene spheres (BIPS) are used to detect motility disorders and obstructions of the GI tract. There are 30 1.5-mm and 9 5-mm BIPS packaged in gelatin capsules (Fig 10.2). The small BIPS mimic the action of food particles; when mixed with food they can be used to estimate the GI transit time of food. The large BIPS are useful for detection of partial (or complete) obstructions (Fig 10.3). Determination of functional (i.e. functional ileus) vs. physical obstruction is made by a combination of history, clinical signs, laboratory findings, radiographic appearance and the BIPS radiographic pattern. Performing surgery or endoscopy after using BIPS is preferable to doing these procedures after barium has been used.

Fig 10.2
Barium impregnated polyethylene spheres (BIPS)
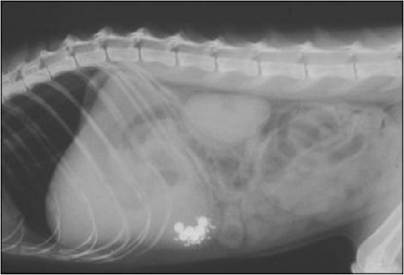
Fig 10.3
BIPS used to show an obstructive pattern where they have bunched together and are not being emptied from the stomach
Ultrasound
Ultrasound is more sensitive than radiography for examining masses, intestinal mural thickenings, GI infiltrative diseases and mesenteric lymphadenopathy. The pancreas, liver, kidneys, prostate and uterus can be more fully evaluated by ultrasound than with radiography. In the hands of a good ultrasonographer, this technique is one of the best methods of diagnosing pancreatitis.
Intussusceptions can sometimes be clearly observed and intestinal peristalsis can be assessed. The organs can be seen through ascitic fluid, but gas, ingesta and faeces can obscure the view. Ultrasound guided fine needle aspirates or larger needle biopsies can sometimes provide useful information and may be preferred to surgically obtained samples in some animals (e.g. with severe hypoalbuminaemia).
Endoscopy
Endoscopy is not appropriate for every animal with GI disease. The more clinically ill patients, with severe signs (e.g. intractable vomiting or haematoemesis), weight loss, anorexia or ultrasonographic signs of infiltrative disease are candidates for endoscopy.
Endoscopic examination and biopsy of the stomach, duodenum and sometimes colon and ileum (Fig 10.4) is an aid in diagnosing inflammatory bowel disease (a common cause of vomiting in dogs and cats). It also aids in the diagnosis of some lymphomas, gastric adenocarcinoma and other gastric cancers, gastroduodenal ulcers, gastritis, pyloric stenosis and some foreign bodies. Some alimentary lymphomas require full thickness biopsy for diagnosis. Foreign bodies may sometimes be removed using the endoscope and forceps or snares.

Fig 10.4
Use of endoscopy to take intestinal biopsies to aid in the diagnosis of vomiting in a cat
Exploratory celiotomy
Exploratory surgery is necessary for the diagnosis of mural diseases (e.g. where mucosal biopsies obtained with an endoscope are not deep enough), for small bowel lesions distal to the reach of the endoscope and for removal of many gastric and nearly all small bowel foreign bodies. Surgery is necessary for the definitive diagnosis and treatment of pyloric stenosis. It is very helpful for the diagnosis of pancreatitis, especially in the cat. It allows visualization and biopsies of multiple organs, including the stomach, small intestine, liver and pancreas. No vomiting (or diarrhoeic) animal should undergo an exploratory surgery without biopsy of the stomach and intestines; performing endoscopy after an exploratory surgery performed without biopsy is an absurd diagnostic approach.
More on the topic 10 Vomiting:
- Nausea and Vomiting
- Medications used in the treatment of gastrointestinal disorders
- 14 Hypoadrenocorticism in a dog
- Port site closure
- HEADACHE
- 10.11 CHOLERA
- Chapter 6 Complications of early pregnancy
- 51 Palliative Care
- Haemorrhagic gastroenteritis in a dog
- Liver disease