12 Chronic partial gastric dilatation in a dog
Initial presentation
Vomiting
Signalment: 8-year-old male entire Labrador, body weight 24 kg
Case history
The dog’s previous history included arthritis, for which he was fed a diet designed for dogs with arthritis and was previously given the non-steroidal anti-inflammatory medication, meloxicam.
He had been off the melox- icam for 3 weeks at admission.The dog had become lethargic during the past month and was vomiting food and brown foam several times a day. He was also occasionally retching. His faeces were soft to watery. The owner had seen the dog in the ‘praying position’ several times during the last week. In this position the dog’s head is down and front legs stretch forward. This usually occurs during episodes of abdominal pain. Prior to this he had had intermittent episodes of vomiting and diarrhoea every few weeks. He had lost about 3 kg during the past month.
The owner reported that during exercise the dog’s breathing pattern had become more laboured and he was not as willing to exercise as he previously had been.
The dog was de-wormed regularly with fenbendazole, although the owner reported that he was 3 weeks overdue for de-worming. He was vaccinated yearly.
His current medication was cimetidine (200 mg po q 8 hours), which had not improved his condition.
Physical examination
The dog was bright and responsive. His body condition score was 4/9. Hydration appeared to be adequate. Mucous membrane colour was pink and capillary refill time was less than 2 seconds. Peripheral lymph nodes were unremarkable.
Thoracic auscultation revealed normal heart and lung sounds, with a heart rate of 100 beats per minute. The respiratory rate could not be counted as the dog was panting. There was evidence of mild to moderate pain or discomfort on abdominal palpation. While this caused difficulty in performing a thorough abdominal palpation, no other abnormalities were detected.
Rectal temperature was 38.9° C.Problem list and discussion of problems
• Vomiting
• Diarrhoea
• Decreased exercise tolerance
• Abdominal discomfort
• Possibly respiratory distress
Differential diagnosis
Vomiting was the dog’s main problem and it was the one initially addressed. Differential diagnoses for vomiting in this dog include the following disorders:
• Disorders of the stomach
• foreign body
• gastritis
• ulceration
• chronic partial dilatation-volvulus
• neoplasia
• Disorders of the small intestine
• foreign body
• inflammatory bowel disease
• neoplasia
• parasites
• intussusception (less likely due to the dog’s age)
• Disorders of the large intestine
• colitis
• obstipation
• Systemic disorders
• pancreatopathy
• hypoadrenocorticism
• diabetes mellitus
• liver disorders
• peritonitis
• renal disease/uraemia (unlikely)
• Dietary causes
• adverse reaction to food (allergy or intolerance)
• dietary indiscretion
Most dogs with intussusception are less than 1 year of age, although it was still a possibility. He did not have any other signs of renal disease such as polyuria or polydipsia, so uraemia was an unlikely cause of the vomiting.
Case work-up
The dog was admitted to the hospital for diagnostic investigation.
Minimum data base
Haematology, serum chemistry and routine urinalysis were performed. Haematology results were unremarkable. Serum chemistry results including amylase, lipase and basal cortisol were within the reference range other than a mild elevation in bile acid concentrations to 19.4 μmol∕l (fasting reference range 0-7 μmol∕l).
A canine pancreatic lipase immunoreactivity test was within the reference ranges, as were serum trypsin-like immunoreactivity and folate. Serum cobalamin was slightly decreased at 268 ng/l (reference range 275-590 ng/l).
Urinalysis, including chemical strip and sediment, was unremarkable.
The urine specific gravity was 1.037.Imaging
Abdominal ultrasound showed decreased gastric motility and the pylorus and duodenum were shifted further towards the midline than normal. All other abdominal organs were considered normal. Contrast radiography was recommended.
Abdominal radiographs showed gas within the gastric fundus, which in the ventrodorsal (VD) view extended across the pylorus. Some gas was also seen in the proximal descending duodenum. The small intestines contained fluid and gas, but appeared to be normal in diameter.
Liquid barium was given to enhance visualization of the gastrointestinal tract. At 5 minutes post barium, a mixture of barium and particulate material was seen within the gas-filled fundus, with most of the barium pooling within the antrum, which appear rounded, dilated and medially displaced. On the VD view the angle between the fundus and the antrum was more acute than normal with the antrum moved toward the midline (Fig 12.1). On both views the pyloric region of the stomach appeared to terminate abruptly (Fig 12.2), with a narrow band of contrast present for several centimetres before the barium began to fill the duodenum.

Fig 12.1
Ventrodorsal abdominal radiograph with barium contrast showing the abnormal (medial) displacement of the pylorus
(courtesy of Dr Tobias Schwarz)

Fig 12.2
Lateral abdominal radiograph with barium contrast showing the narrow band of contrast present for several centimetres before the barium began to fill the duodenum
(courtesy of Dr Tobias Schwarz)
At 30 minutes post barium, most of the barium had passed into the lower small intestine; however, the antrum still appeared to have an abnormal location.
At 2 hours post barium, some barium was still retained within the stomach, predominantly in the antrum and pylorus. The antrum appeared less rounded and had a less acute angle with the lesser curvature than previously.
The filling of the proximal duodenum remained incomplete with a narrow band of contrast in it.Gastrointestinal endoscopy was attempted. The endoscopist had unusual difficulty passing the endoscope through the lower oesophageal sphincter into the stomach. The endoscopic view of the stomach was initially abnormal with the landmarks of the stomach (e.g. lesser curvature, antrum) appearing to be in the wrong place. During the endoscopy the stomach changed shape and landmarks appeared in the correct places. The duodenum was unremarkable. Routine biopsy samples were taken of the stomach and duodenum.
Case assessment
From the history, imaging and endoscopy it appeared that the dog had a chronic dynamic partial gastric torsion which was occurring intermittently. Exploratory surgery was scheduled.
Surgical management
At surgery a partial gastric torsion was identified. A belt loop gastropexy was performed to prevent reoccurrence or progression to gastric dilatation volvulus (Fig 12.3). Further full thickness biopsies were taken of the stomach and jejunum.
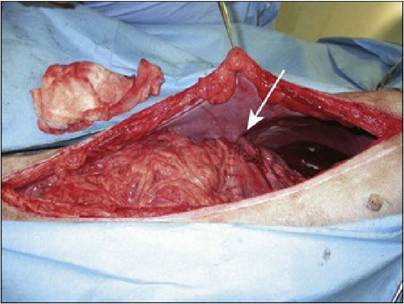
Fig 12.3
Belt loop gastropexy in place (arrow)
(courtesy of Dr Donald Yool)
Histopathology
Histopathology of the biopsies showed that the stomach and duodenum were normal. The histopathology of the jejunum was diagnosed as mild, diffuse, Chronicjejunitis.
Follow-up
The dog recovered well from the surgery and at 1 month was exercising at nearly normal levels. He was eating well and not vomiting.
Medical management
While the surgery should prevent the stomach from torsing, some cases do continue to have episodes of gastric dilatation. Recommendations for these cases include the frequent feeding of small, low carbohydrate, low fat, high protein meals and the use of prokinetic drugs such as metoclopramide, cisapride or low dose erythromycin (0.5-1.0 mg/kg po q 8 hours, in between meals).
In dogs, erythromycin at these low doses stimulates motilin release and promotes the interdigestive ‘housekeeping’ wave, promoting emptying of solids. Products containing peppermint have a mild prokinetic effect and may be useful. Anti-foaming agents such as dimethacone or simethacone have been shown to be of benefit in some animals.Case discussion and epidemiology
Dogs with chronic gastric distension and radiographic evidence of a twisted stomach may have a chronic intermittent form of gastric volvulus which usually corrects spontaneously. The radiographic appearance is of the pylorus moving too close to the midline as the stomach fills with air. It is possible for this to progress to a gastric dilatation volvulus with torsion (Fig 12.4). The cause is unknown, but may be due to an impaired ability to eructate and possibly delayed gastric emptying.
Sequence of gastric dilation with torsion
Clockwise rotation as viewed from a ventral position.

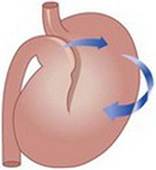
The pyloric antrum is displaced downward.
The pylorus crosses the midline, passes underneath the distended proximal part of stomach, and moves upward along the left abdominal wall.
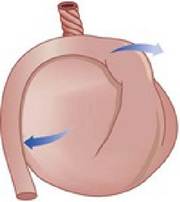
The gastric fundus moves ventrally and becomes located in the ventral abdomen.
The continuing gastric dilation displaces the greater curvature ventrally.
Fig 12.4
An illustration of how the pylorus crosses the midline in a gastric torsion, causing the pylorus to be closed off and resulting in increased gas and fluid in the stomach
Eructation should be initiated by gaseous distension of the stomach (especially the cardia) and is mediated by receptors in the cardia and vagal afferents to the brain.
The response is a reduction in the pressure at the cardia and lower oesophageal junction to less than that of the rest of the stomach so that the gas can escape. Defective eructation could be due to a defect in the junction sphincter in the reflex, e.g. a disorder of the vagal innervation or a deficit in the sensory function of the cardia. The gastric cardia may be damaged by over-distension, so that dogs which have had gastric dilatation may be prone to recurrent episodes.Gastric gas is usually from swallowed air, the reactions of gastric acid with secretions containing bicarbonate or from bacterial fermentation. Rapid eating and drinking increases the amount of swallowed air; nervous, excited or dysphagic (e.g. oesophageal motility disorders) animals are more likely to swallow air. Animals with respiratory distress or hyperventilation also tend to swallow air.
Composition of the diet has been suggested to increase the incidence of gastric dilatation; however, this has not been proven and gastric dilatation volvulus has been reported in dogs fed fresh meat, soy-based or cereal-based diets. The intake of a large amount of food rapidly will cause gastric dilatation and the stomach takes longer to empty. It is recommended that dogs at risk for gastric dilatation or that have a history of dilatation be fed several smaller meals per day instead of one large one.
Large breed deep-chested breeds of dogs appear to be at increased risk, but no age or sex predilection has been recognized.
Prognosis
Resolution of most of the clinical signs often follows gastropexy and management of gastric dilatation. Some animals continue to bloat, but with gastropexy the stomach should not be able to twist, so that overall the prognosis is good.