33 Intestinal leiomyoma in a dog
Case contributed by Carolina Urraca del Junco
Initial presentation
Intermittent melaena
Signalment: 12-year-old neutered male, English springer spaniel, body weight 19.8 kg
Case history
The dog presented to the hospital for investigation of 2 to 3 weeks of intermittent melaena, lethargy and pale mucous membranes.
His faeces were formed, but varied in colour from dark brown to tarry and black. There was no bright red blood or mucus present in the faeces and the dog did not have an increase in urgency of defecation. The dog’s appetite had recently decreased, although he was still eating. He was thought to have lost weight, although the amount was not known. He had not been vomiting.The dog’s usual diet was a high quality commercial dry dog food. He was not fed scraps or extra treats and did not have a history of scavenging. He was current on his vaccinations and had been de-wormed 5 months prior to presentation.
Physical examination
On presentation, the dog was quiet, but alert and responsive. His body condition score was 5/9. His oral mucous membranes were very pale, but capillary refill time was normal. His mucous membranes were moist and he appeared to be well hydrated. His heart rate was mildly elevated at 134 beats per minute and his respiratory rate was also slightly elevated at 36 breaths per minute. The rectal temperature was within normal limits at 38.2° C. Auscultation of the thorax and abdominal palpation were unremarkable and his peripheral lymph nodes felt normal.
Problem list and discussion of problems
The dog’s main problems were the lethargy, pale mucous membranes and intermittent melaena. Pale mucous membranes can be caused by either poor perfusion or anaemia. The dog had no evidence of cardiovascular disorders and was well hydrated. The lethargy and likely anaemia (confirmed by packed cell volume (PCV)) were thought to be due to intestinal blood loss resulting in the melaena.
Differential diagnosis
Differential diagnoses for melaena in this case included:
• Swallowed blood from oral, nasal, pharyngeal or respiratory system disorders (melaena)
• Oesophageal disorders, e.g. ulcer or neoplasia
• Internal parasites, e.g. hook worms
• Gastrointestinal neoplasia, e.g. adenocarcinoma, mast cell tumour, gastrointestinal lymphoma, multiple myeloma, gastrinoma, leiomyoma, leiomyosarcoma
•Inflammatory bowel disease with ulceration
•Sharp or penetrating gastrointestinal foreign body
• Vascular disorders, e.g. colonic vascular ectasia, although it would have to be in the proximal colon as there was no haematochezia
Other less likely differential diagnoses include:
•Hepatopathy (no other consistent clinical signs)
•Uraemia (no polyuria present)
•Pancreatitis (unlikely with no vomiting or evidence of abdominal pain)
•Disseminated intravascular coagulopathy (unlikely)
• Coagulopathies, e.g. vitamin K deficiency, thrombocytopenia, von Willebrand’s disease (less likely as no signs of bleeding elsewhere and no previous history of bleeding)
•Drugs, e.g. NSAIDs, corticosteroids (no history of drug administration)
• Toxins, e.g. caustic agents, heavy metals, Amanita (magic) mushrooms (no known history of ingestion of toxins)
Case work-up
Minimum data base
Routine haematology revealed a severe anaemia with a PCV of 0.11 l/l (reference range 0.39-0.55 l/l, with moderate red blood cell regeneration (corrected reticulocyte count 2.76%). There was a low mean corpuscular volume (MCV) of 56 fl (reference range 60-77 fl) and low mean cell haemoglobin concentration (MCHC) of 30.2% (reference range 32-36%). The microcytosis and hypochromia were consistent with iron deficiency anaemia. Blood smear evaluation revealed marked microcytic hypochromic anaemia with moderate numbers of polychro- matophils and small numbers of normoblasts. There was a moderate RBC anisocytosis and mild hypochromia. The platelet number appeared adequate.
There was a moderate mature neutrophilia and a mild monocytosis, with a few reactive lymphocytes.As the dog had a history of melaena, the regenerative anaemia was thought to be likely to be secondary to gastrointestinal blood loss, although haemolysis was possible. A slide agglutination test was negative and Coombs tests for IgG, IgM and complement were also not consistent with immune mediated haemolysis. The haematological parameters were consistent with an iron deficiency anaemia, also likely due to gastrointestinal blood loss.
The dog was dog erythrocyte antigen (DEA) 1.1 blood type positive on an in-house test, which also showed no evidence of auto-agglutination (Fig 33.1).
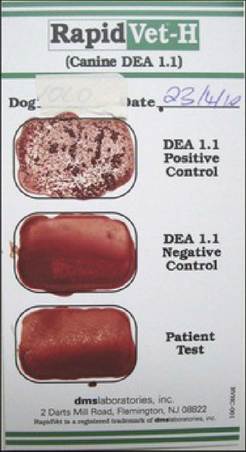
Fig 33.1
In-house blood typing showing a DEA 1.1 positive sample.
Serum biochemistry revealed mild hypoproteinaemia with a total protein of 46.4 g/l (reference range 58-73 g/l) due to decreased albumin of 20.4 g/l (reference range 26-35 g/l) and globulins at the low end of the reference range at 20 g/l (reference range 18-37 g/l). Decreased albumin can be caused by ongoing intestinal loss, urinary loss, third spacing or decreased hepatic production due to liver disorders or decreased production during an acute phase protein reaction (albumin is considered a ‘negative’ acute phase protein).
Urinalysis was unremarkable with a urine specific gravity of 1.032. Faecal analysis was negative for parasites and for enteropathogens.
The microcytic, hypochromic, mildly regenerative anaemia, reduced total protein and albumin, with globulins in the lower part of the reference range, suggested chronic blood loss.
Imaging
Right lateral and ventrodorsal thoracic and abdominal radiographs were obtained. In the thoracic radiographs, several well-defined 1- to 2-mm opaque nodules characteristic of pleural plaques were identified within the lung fields (Fig 33.2). The cardiac silhouette was within normal limits.
There was no evidence of thoracic metastatic disease. Both shoulders showed evidence of degenerative joint disease. Abdominal radiographs revealed a faeces-filled normal size colon (Fig 33.3). The transverse colon was partially displaced dorsally by a poorly marginated soft tissue mass.Fig 33.2
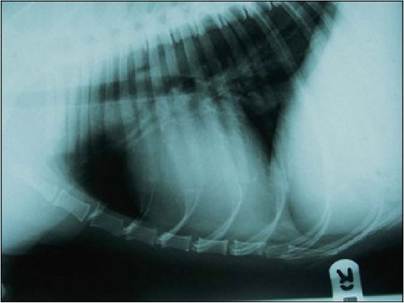
Lateral thoracic radiograph showing nodules characteristic of
pleural plaques
(courtesy of Carolina Urraca del Junco).

Fig 33.3
Lateral abdominal radiograph showing full colon
(courtesy of Carolina Urraca del Junco).
Ultrasonography of the abdomen showed a midline mass identified caudal to the stomach, in the ventral abdomen, with normal jejunal loops entering both ends. The mass was well vascularized and protruded into the intestinal lumen, with evidence of luminal dilatation and a partial loss of wall layering. At the centre of the mass, there was a rounded
vascularized out-pouching of intestinal wall tissue, which appeared to connect to the intraluminal tissue. This out-pouching showed no evidence of intestinal wall layering (Fig 33.4). The location of the mass was consistent in location with the radiographically identified soft tissue mass. The duodenum, ileum and the large intestines were within normal limits and the remainder of the ultrasound examination was unremarkable.
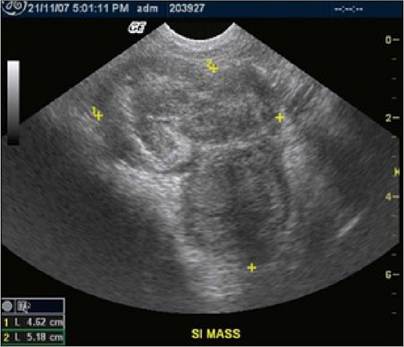
Fig 33.4
Ultrasound picture of jejunal mass with an outpouching of intestinal wall
(courtesy of Carolina Urraca del Junco).
Based on these findings a tentative diagnosis of jejunal neoplasia was made. Adenocarcinoma, leiomyoma, leiomyosarcoma, other sarcomas, metastatic disease involving the jejunum and lymphoma were considered to be the most likely differential diagnoses.
Surgical treatment
After imaging, the dog received a blood transfusion with one unit of
DEA 1.1 positive blood and underwent enterectomy to remove the mass, which measured 4 cm in diameter and was localized within the jejunum. The appearance of regional lymph nodes and other abdominal organs was unremarkable. A jejunal end-to-end anastomosis was performed using surgical staples and the ventral midline incision was closed routinely.
Histopathology
The mass was submitted for histopathology. Macroscopically, the external appearance of the mass was contiguous and well-encapsulated, with a firm serosal surface.
The solid mass identified on ultrasound as expanding eccentrically from the jejunal lumen consisted of irregular swathes, whorls and streams of intensely eosinophilic bundles of uniform fibres, consistent with smooth muscle. These smooth muscle cells contained occasional ellipsoidal pale nuclei, with a finely stippled chromatin pattern. No mitotic figures were noted in the examined sections and no inflammatory cells were seen within the mass.
The solid mass was found to infiltrate the submucosa and mucosa and extend in an annular fashion around the lumen. Normal mucosa was partially replaced with whorls and streams of eosinophilic tissue and there was an oedematous inflammatory reaction at the mucosal surface. Dystrophic calcification was identified on one section at a junction between normal and abnormal mucosa (Fig 33.5).
Fig 33.5
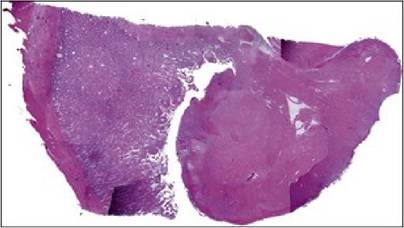
Histopathology of intestinal mass consistent with smooth muscle tissue
(courtesy of Carolina Urraca del Junco).
The appearance of well-differentiated smooth muscle cells and the absence of mitotic figures were consistent with a diagnosis of a benign leiomyoma, likely originating from the jejunal muscularis propria. As this was a solitary mass, the long-term prognosis was considered as very good.
Outcome
One week after surgery, the dog was discharged with instructions to restrict exercise until removal of skin staples.
A 10-day course of clavulanate-potentiated amoxicillin (250 mg po q 12 hours) was prescribed.In addition, iron supplementation (ferrous fumerate) was started at 200 mg po q 24 hours. At discharge the dog’s PCV was 0.17 l/l. Iron supplementation was continued until erythrocyte parameters were back within the reference range.
Six months later the dog had good exercise tolerance, had gained weight and was no longer anaemic.
Discussion and epidemiology
Melaena and microcytic, normochromic or hypochromic anaemia are common findings in cases with gastrointestinal ulceration due to tumours. Leiomyomas and leiomyosarcomas, in particular, may cause especially dramatic bleeding due to their propensity to ulcerate. Other signs of these intestinal tumours may include obstruction, vomiting, anorexia, diarrhoea, abdominal pain and weight loss. Hypoglycaemia associated with intra-abdominal leiomyoma has been reported. This was thought to be potentially due to an increase in insulin-like growth factor produced by the tumour. Leiomyomas are usually slow growing tumours and they may reach a large size before clinical signs are seen.
Intestinal tract neoplasia may be diffuse or nodular, with a variable incidence of local lymphadenopathy as a result of metastatic spread or reactive change. Therefore if the intestinal tract is abnormal, surgical biopsies should be taken from the tract itself and not just from the enlarged lymph nodes. Benign tumours are characterized by small cells, with small nuclei and little variation in cell and nuclear size. Leiomyoma is a benign tumour of smooth muscle origin and it is less common than leiomyosarcoma.
Several ultrasonographic features of gastrointestinal smooth muscle tumours are helpful in differentiating them from other types of gastrointestinal neoplasia. Leiomyosarcomas and leiomyomas are often large (over 3 cm) intramural lesions growing out of the serosa as large eccentric or extraluminal masses. Uncommonly, as in this case, they also invade or project into the gastrointestinal lumen. Anechoic and hypo- echoic foci within the mass may correlate with the areas of central degeneration and necrosis frequently found in these lesions.
Gastrointestinal leiomyomas that show phenotypic features of typical smooth muscle cells occur most commonly in the oesophagus in humans. Published case series in humans show median ages of 30 to 35 years and these tumours are very rare in the stomach and intestines. In dogs, by contrast, benign leiomyomas occur most commonly in the stomach of geriatric dogs, while a higher incidence of malignant tumours with smooth muscle appearance are reported in the small intestine and caecum.
The signalment of this case, a 12-year-old male dog, is in keeping with published data - most leiomyomas occur in older male dogs. In one study, 82% of leiomyomas occur in male dogs, with a mean age of 11 years (range 8-17 years) at presentation. Only 31% of the cases had associated clinical signs. In another study, the mean age for dogs with small intestinal smooth muscle tumours (9.1 ± 2.3 years) was lower than for dogs with caecal tumours (10.7 ± 1.9 years). In contrast to dogs with intestinal tumours, which all showed clinical signs in this study, four dogs with caecal tumours showed no clinical signs at all and the mass was an incidental finding. In dogs with intestinal tumours, weight loss was observed more often, whereas intestinal perforation and peritonitis were observed more commonly in dogs with caecal tumours. In general the caecal tumours showed higher scores for necrosis and bleeding. No breed predilection has been reported.
In humans, many of these tumours were formerly diagnosed as smooth muscle tumours but have been reclassified as gastrointestinal stromal tumours. Apart from the surgical therapy in humans, an additional medical treatment under investigation is selective receptor tyrosine kinase inhibitor (imatinib mesylate) therapy.
Prognosis
An increased tumour diameter has been observed to be an important negative prognostic indicator and castrated or spayed dogs have been reported to have better survival statistics than intact dogs. In one study, in the 42 dogs with small intestinal tumours that were surgically-treated, the overall 1- and 2-year survival times were 63% and 52%, respectively. For the 19 dogs with caecal tumours that were surgically treated, the respective survival times were 84% and 66%. Of the surgically treated dogs, nine (of 42) with a small intestinal tumour and one (of 19) with a caecal tumour, died within 15 days because of surgery or tumour-related complications. For the remaining dogs with small intestinal tumours, the 1- and 2-year recurrence free period was 80% and 67% whereas, for the dogs with the caecal tumours, this was 83% and 62%, respectively.
No significant influence on prognosis after surgical removal has been identified based on tumour type or histological characteristics. Even dogs with tumours with very malignant histological appearance have a relatively good prognosis for long-term survival if complete excision of the tumour is accomplished.
More on the topic 33 Intestinal leiomyoma in a dog:
- Intestinal Plasmacytosis
- 24 Small intestinal diarrhoea
- Intestinal Pseudo-Obstruction (Ileus)
- Eimeria spp. Infection: Intestinal Coccidiosis
- ACUTE INTESTINAL OBSTRUCTION
- Intestinal Obstruction and Rupture
- 38 Colorectal neoplasia in a dog
- 23 Intestinal disorders
- 14 Hypoadrenocorticism in a dog
- 16 Ingestion of glue by a dog
- STOMACH AND INTESTINAL WORMS
- 11 A foreign body in the small intestine of a dog
- 12 Chronic partial gastric dilatation in a dog
- 13 Pancreatitis and alimentary lymphoma in a dog
- 21 Porto-systemic shunt in a dog
- 2 Idiopathic megaoesophagus in a dog
- INTESTINAL MALFORMATIONS
- 3 Myasthenia gravis in a dog