24 Small intestinal diarrhoea
Diarrhoea may be determined to be of small intestinal origin when there are large volumes of faeces produced without evidence of tenesmus or dyschezia and there is no bright red blood or mucus present on the stools.
Weight loss may accompany diarrhoea of small intestinal origin.Some of the differential diagnoses of small intestinal diarrhoea include:
• Dietary
• food poisoning
• adverse reaction to food (allergy or food intolerance)
• dietary indiscretion (e.g. raiding the rubbish bin)
• sudden change of diet
• Gastric
• dumping syndrome, where too much food is presented to the duodenum rapidly
• Small intestinal diseases
• infectious (viral infections, bacterial, e.g. Salmonella spp., Campylobacter spp., E. coli enterotoxins).
• parasites (e.g. Giardia, strongyloides, ascarids, hookworms)
• inflammatory bowel disease
• infiltrative neoplasia (e.g. lymphoma, mastocytosis)
• lymphangiectasia
• brush border enzyme defects
• antibiotic responsive diarrhoea (ARD) (or antibiotic responsive enteritis)
• partial obstruction (e.g. intussusception, neoplasia, foreign body)
• extraluminal obstruction
• ischaemic disease (infarction, torsions)
• haemorrhagic gastroenteritis
• Secondary systemic disorders
• pancreatitis
• exocrine pancreatic insufficiency (EPI)
• Liver disease, including biliary diseases and porto-systemic shunts, in- trahepatic cholestasis or bile duct obstruction
• Kidney disease
• Hyperthyroidism in cats
• Hypoadrenocorticism
• Congestive heart failure
• Feline viruses (feline infectious peritonitus (FIP), feline leukaemia virus (FeLV))
• Miscellaneous causes
• toxaemia (e.g. pyometra, peritonitis)
• toxins and drugs (e.g. non-steroidal anti-inflammatory drugs, lead, organophosphates)
• APUDomas (e.g. gastrinoma)
• autoimmune disorders (e.g.
systemic lupus erythematosus)Further investigation of chronic small intestinal diarrhoea
Dietary trial
If there are no abnormalities detected during the physical examination and the animal is bright and eating well, feeding an exclusion diet with a novel protein source or a hydrolyzed protein source for 2 to 6 weeks may be tried prior to further testing. In cats with diarrhoea, many respond to a restricted novel protein diet within a week. If the restricted diet is successful in improving the clinical signs, ideally a challenge with the previous food or snacks should be tried to prove that dietary sensitivity is the cause of the diarrhoea. Many owners are understandably reluctant to try this challenge and a new diet may be designed using the trial food. The owners should understand that the animal may become sensitized to the new diet and again develop diarrhoea.
Minimum data base
For cases in which the patient is systemically unwell or has not responded to dietary therapy and an appropriate de-worming programme, a minimum data base of haematology, serum biochemistry including basal cortisol and urinalysis should be performed. In cats, serologic tests for FeLV, FIP and a total serum thyroxine concentration should be included. These tests evaluate the patient for systemic diseases such as kidney disease, hepatopathies, hypoadrenocorticism, hyperthyroidism and viral diseases. A low albumin may be present in hepatopathies or protein losing enteropathy or nephropathy. If low protein is combined with low serum cholesterol and lymphopenia, lymphangiectasia may be present. Eosinophilia may be present with eosinophilic gastroenteritis, parasitism and hypoadrenocorticism. The minimum data base also aids in assessing hydration status and electrolytes which will guide the clinician in the choice of fluid therapy.
Faecal tests
Further testing may include faecal analysis for parasites and enteropath- ogenic bacteria, e.g. Salmonella, Campylobacter and Yersinia.
Diarrhoea due to Campylobacter is more common in younger animals and the bacteria can also be isolated from the faeces of healthy animals. Salmonella can also be present in the faeces of animals without clinical signs and should probably not be treated unless serious or systemic signs are present as treatment may prolong the carrier state.Toxin producing Clostridium difficile may cause acute or chronic diarrhoea. Faecal cultures for C. difficile are of no value because it is found in faeces from healthy animals and the presence of it does not prove that it is producing a toxin. Diagnosis of enterotoxigenic clostridia is best supported by a positive enterotoxin assay.
A fresh saline smear may detect Giardia trophozoites, although zinc sulphate flotation which detects Giardia cysts is more accurate. If giardiasis is suspected but cannot be confirmed a therapeutic trial with fen- bendazole may be indicated.
Faecal alpha-1-antiprotease
Faecal alpha-1-antiprotease has been measured in the USA as an indicator of gastrointestinal (GI) protein loss and is useful to determine that intestinal loss is the cause of hypoproteinaemia.
Trypsin-like immunoreactivity and pancreatic lipase immunoreactivity
If EPI is a possibility, a trypsin-like immunoreactivity (TLI) test should be done. This is the test of choice for EPI, in which the serum concentration is decreased. The TLI test may be also useful as an adjunctive test in some cases of acute pancreatitis where TLI is temporarily increased, although the pancreatic lipase immunoreactivity (PLI) tests are more spe-
cific and have a more prolonged increase in cases of pancreatitis. There are species specific PLI tests for dogs and cats and an in-house serum SNAP cPLI test for dogs (Fig 24.1).


The SNAP® cPL test used for in-house screening for pancreatitis
Folate and cobalamin (vitamin B12)
Serum folate and cobalamin (vitamin B12) may be decreased in small intestinal disease due to poor absorption.
In some cases where there are excessive bacteria in the proximal small intestine the cobalamin may be low due to bacterial consumption and the folate increased due to bacterial production. Excessive bacteria in the intestine has been termed small intestinal bacterial overgrowth (SIBO), a disease process documented in people with >105 colony forming units (CFU) per millilitre of fasting duodenal intestinal fluid. The accuracy of the term SIBO in small animal patients is dubious. In many dogs with bacterial disorders of the small intestines, it is probably an incorrect description. Studies have shown that clinically normal dogs can have >108 CFU/ml of bacteria in the upper small intestine and this number is clearly in excess of what was initially accepted as being definitive for SIBO (>105 CFU/ml).The terms antibiotic responsive enteropathy (ARE) or antibiotic responsive diarrhoea (ARD) are now more commonly used. The terms ARE or ARD seem to be preferable to SIBO in most dogs because essentially this is a syndrome in which the patient has small intestinal disease which responds to the administration of antibiotics.
Histopathology and cytology of the intestinal mucosa are extremely insensitive at detecting ARE. Serum cobalamin and folate concentrations have been used for diagnosis and finding both a low serum cobalamin and an increased serum folate concentration had been considered to be relatively specific for ARE.
Dietary folate supplementation contributes to increased blood folate values. Measuring serum cobalamin and folate concentrations is relatively insensitive at detecting ARE or SIBO. There are many dogs with chronic GI disease that respond to antibiotic administration but which have normal cobalamin and/or normal folate concentrations. However, they should be measured in animals suspected to have intestinal disease as hypocobalaminaemia or low serum folate should be treated.
In cats, low serum cobalamin may occur with EPI, intestinal disease (e.g.
IBD or LSA), hepatobiliary disease or pancreatic disease. Cats appear to be highly susceptible to cobalamin deficiency as it has a short half-life in this species (12.75 days in healthy cats, 5 days in cats with intestinal disease).Serum lead concentrations should be determined if there is a history consistent with exposure to lead (e.g. remodelling an older house, lead pipes), especially if central nervous system or behaviour changes are present. Serum organophosphate concentrations should be determined if there has been possible access to these toxins.
Gastrointestinal permeability testing with inert sugar analysis
During some intestinal diseases the mucosal cells are destroyed, decreasing the number of cellular small pores and increasing the number of large pores between the cells, thereby changing the ratio of the two types (Fig 24.2). By using oral administration of sugars of different sizes which move through the different types of pores and measuring the urine recovery of the sugars, a ratio of the recovered sugars can be determined. This appears to correlate with the degree of pathological increase in intestinal permeability.
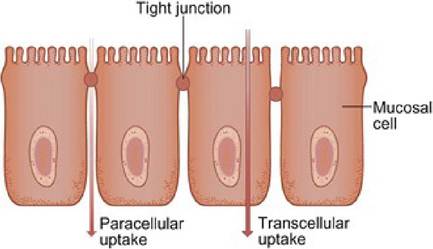
Fig 24.2
Testing of intestinal permeability testing is based on the difference between uptake of sugars via the transcellular route and via the paracellular route
Imaging
Radiography
While generally survey radiographs are of limited value in patients with chronic diarrhoea, contrast studies may help in some cases. Abdominal radiography can aid in the diagnosis of complete or partial obstructions (especially when combined with contrast study using barium suspension or barium impregnated polyethylene spheres), assessment of ileus and diagnosis of an intussusception.
Radiography also helps assess liver and kidney size, presence of abdominal fluid, organ torsions, peritonitis and sometimes pancreatitis.
Ultrasonography
Abdominal ultrasound is more sensitive than radiography for the detection of masses, assessing the pancreas and liver parenchyma, mesenteric lymph nodes and intestinal wall thickness and irregularity.
In some cases ultrasonography can provide additional information, in particular to evaluate the GI peristalsis, and also can allow the identification of the cause of the ileus such as an intussusception or an intestinal foreign body.
Ultrasonographic examination of the small intestine includes evaluation of wall thickness and layering, evaluation of luminal contents and measurement of peristaltic function. In the normal dog, the gastric wall is 3 to 5 mm thick when the stomach is moderately distended and may be slightly thicker when the stomach is not distended. The normal thickness of the small and large bowel wall is 2 to 3 mm when measured during bowel relaxation.
Pathologic thickening should be suspected when wall thickness exceeds 6 to 7 mm in the stomach and 5 mm in the bowel.
Ultrasonography allows differentiation of the layers of the intestine, which alternate in echogenicity. Under optimal conditions, five separate layers can be identified (see Figs 15.4-15.5). These include the mucosal surface (hyperechoic), mucosa (hypoechoic), submucosa (hyperechoic), muscularis (hypoechoic) and serosa (hyperechoic). The submucosa and subserosa-serosa are hyperechoic because of the presence of relatively more fibrous connective tissue. Examination of the layers of the stomach and bowel may be helpful in determining the severity and location of pathologic processes.
Evaluation of intestinal motility should be included in the examination. The mean number of peristaltic contractions in the stomach and proximal duodenum is four to five per minute.
In some cases of intestinal neoplasia, a focal thickening of the intestinal wall can be observed, with intestinal dilatation present proximal to it and often fluid accumulation. In the area of wall thickening, the normal layered pattern of the intestinal wall is usually absent. Intestinal lymphomas are often characterized by a diffuse neoplastic infiltration of the wall rather than a focal mass.
Endoscopy and intestinal biopsy
Endoscopy allows visual assessment and biopsy of the intestinal mucosa and is safer and less invasive than surgery, which is especially useful in hypoalbuminaemic patients. The investigation of small bowel diarrhoea, protein losing enteropathies, chronic vomiting (intermittent or persistent) and melaena are the major indications for duodenoscopy. The prior work-up should first rule out underlying metabolic, parasitic, infectious and pancreatic causes before pursuing primary intestinal disorders with endoscopy. The diffuse nature of many intestinal causes of small bowel diarrhoea and protein losing enteropathies means that duodenoscopy may enable a diagnosis to be obtained without recourse to surgery.
Endoscopy allows the clinician to assess the mucosal colour, presence of haemorrhage, texture (e.g. friability or granularity) and detect luminal masses. Friability describes the ease with which the mucosa is damaged by contact with the endoscope or the biopsy forceps and, along with granularity (sometimes referred to as a cobble-stone appearance), is a good indicator of increased cellularity, although differentiation between inflammation and neoplasia cannot be made without histopathology. Gross abnormalities such as undigested food, large amounts of fluid, tumours, foreign bodies and parasites are easily detected. Deflation and inflation of the duodenum enables detection of alterations of distensibility and mucosal irregularities.
Histopathology of intestinal biopsies is frequently required to make a diagnosis and should be part of the endoscopic procedures in dogs and cats with diarrhoea. The biopsies are restricted to the mucosa unless multiple samples are taken in the same location. The endoscopist rarely is able to proceed much further than the duodenum, so focal lesions in the jejunum may not be accessible. For these lesions and for full-thickness biopsies, an exploratory laparotomy or laparoscopy is required.
Exploratory laparotomy
If the patient is a good surgical risk, surgical exploration of the abdomen provides a good, although invasive, method of examining the abdominal organs, obtaining full thickness intestinal biopsies and potentially treating some intestinal disorders such as focal tumours, intussusception and foreign bodies. In diarrhoea cases, biopsies of the small intestine should always be performed (even if it grossly appears normal).
Investigation of acute diarrhoea
The majority of cases of acute diarrhoea are dietary induced and selflimiting. Dietary problems can include ingestion of excessive amounts of food, especially fatty or high carbohydrate foods to which the animal is not accustomed, ingestion of spoiled foods or carcasses or ingestion of a food to which the animal is allergic or intolerant.
Viral infections, bacterial infections and metabolic disorders are also possible causes of acute diarrhoea. Ingestion of toxins, exacerbation of hypoadrenocorticism, pancreatitis, ischaemic disease or haemorrhagic gastroenteritis can cause the acute onset of diarrhoea.
Differential diagnosis of infectious causes of diarrhoea in dogs and cats include:
• Parvovirus, Coronavirus
• Salmonellosis
• Campylobacter infection
• Yersinia spp. (uncommon)
• Clostridium perfringens
• E. coli
Tests for these are the same as for chronic diarrhoea (see page 116).
Many patients remain bright and may continue to eat. Depending on the cause, they may or may not vomit. The diarrhoea may be soft to liquid in consistency.
Treatment for dietary indiscretion (e.g. patient ate from the rubbish bin) is supportive. If the animal is vomiting or dehydration is present intravenous or subcutaneous fluid administration is advised. If osmotic diarrhoea is suspected (e.g. food overload) withhold food for 12 to 48 hours followed by the use of a highly digestible, low fat diet fed frequently and in small amounts. Anti-emetics (e.g. maropitant or metoclopramide) may be used if needed. Anti-diarrhoeal drugs (e.g. loperamide or diphenoxylate) may be used if an infectious cause is not suspected; these are relatively contraindicated with infectious diarrhoea as they may prolong the presence of the bacteria within the intestinal tract. Antibiotics should be given if there is a known bacterial cause of the diarrhoea and are contraindicated for acute diarrhoea cases otherwise. Spasmolytics are also contraindicated as they decrease intestinal segmentation. The use of probiotics or prebiotics may have some beneficial effects in the treatment of diarrhoea.
More on the topic 24 Small intestinal diarrhoea:
- Intestinal Trematodes Sphaeridiotrema globulus AND S. PSEUDOGLOBULUS
- Haemorrhagic gastroenteritis in a dog
- 14 Hypoadrenocorticism in a dog
- Faecal incontinence
- MALIGNANT CATARRHAL FEVER