MALIGNANT CATARRHAL FEVER
HUGH W. REID
The Moredun Foundation, Pentlands Science Park, Bush Loan, Penicuik, Midlothian
Malignant catarrhal fever (MCF) is a generally fatal disease of artiodactyla, primarily affecting ruminants of the subfamily Bovinae and family Cervidae(21).
It is caused by closely related rhadino herpesviruses, which characteristically infect their natural host in the absence of any recognized clinical signs but which are capable of transmission to other species, causing a catastrophic immunological dysfunction and resulting in dramatic clinical and pathological disease(22).AETIOLOGY
Worldwide, the principle cause of MCF is the rhadino herpesvirus, Ovine herpesvirus 2 (OvHV2), which infects domestic sheep and may infect other species of the subfamily Caprinae, in the absence of recognised disease1-23). The other principle cause of MCF is Alcelaphine herpesvirus 1 (AlHV1), which inapparently infects wildebeest (Connochaetes spp.). This form of the disease primarily affects cattle in Africa but has also affected other ruminant species in zoological collections elsewhere. In addition, Caprine herpesvirus 2 (CpHV2) of domestic goats and the so-called virus of ‘white-tailed deer’ have also been implicated as causal agents in a few cases.
I n the context of European wildlife, the only known potential causes of disease are OvHV2 and CpHV2, neither of which have been isolated in conventional culture systems. Infection with either agent can, however, be confirmed through PCR or detection of antibody that crossreacts with the AlHV1 antigens.
These viruses, together with those of large African antelope (Alcelaphinae and H ippotraginae) form a complex of viruses referred to as the MCFV complex (Figure 1.2)(24).
EPIDEMIOLOGY
GEOGRAPHICAL DISTRIBUTION AND HOSTS
Initially MCF was described as a disease of domestic cattle in Europe, but a very similar disease of cattle was recognized in southern Africa shortly thereafter and subsequently has been reported in a variety of species worldwide(25).
Cattle of Asiatic origin (Bos javanicus and Bos gaurus), water buffalo (Bubalus bubalis), many species from the family Cervidae, excluding fallow deer (Dama dama), and North American bison (Bison bison) are particularly susceptible to infection.Despite the normally dramatic fatal presentation of the disease and high incidences in deer and bison when managed as farm animals, there are relatively few reports of the disease affecting free-living animals(26-28). In addition, as it is now recognized that OvHV2 can cause MCF in domestic pigs(29), it is probable that wild boar would also be susceptible, although no disease has been reported in Europe or elsewhere. It should also be noted that experimentally both AlHV1 and OvHV2 can be transmitted to laboratory rabbits, producing characteristic MCF(30). It is therefore theoretically possible that wild rabbits could be affected, although no such cases have been reported.
Both sheep and goats appear to be able to act as natural hosts for OvHV2, whereas only goats have been identified in the case of CpHV2. In the natural host, infection appears to transmit efficiently with all, or most, adults
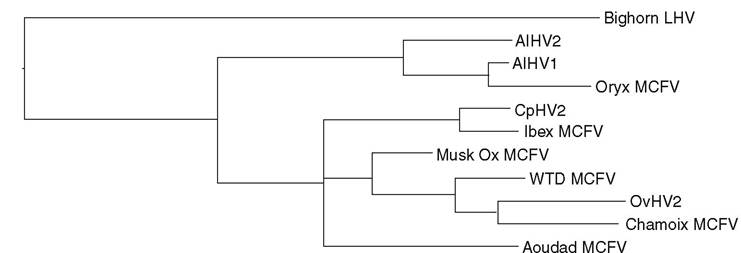
0.1 Expected Substitutions per Site
FIGURE 1.2 Phylogenetic analysis of MCF viruses was based on a 177 bp fragment of the DNA polymerase gene, for which the widest range of sequences were available. The DNA sequences were aligned using ClustalV, based on the translated amino acid sequences, and the phylogenetic analysis was done using TθPALi(24). Model selection was used to define the appropriate parameters for analysis by Mr Bayes using codon position models. The sequence from the bighorn sheep lymphotropic herpesvirus was included as an outgroup. The analysis was performed by Dr George Russell, Moredun Research Institute. AlHV = alcelaphine herpesvirus; CpHV = caprine herpesvirus; LHV = lymphotropic herpesvirus; OvHV = ovine herpesvirus; WTD = white-tailed deer.
carrying latent infection. Transmission of OvHV2 in Europe would appear to be essentially perinatally among lambs, establishing a life-long latent infection, probably as with other herpesvirus infections, with periodic recrudescence and virus excretion(31). All sheep and goats should thus be regarded as potential sources of infection. It is probable that native European species of sheep and goats and related species of the subfamily Caprinae are carriers of these, or similar, viruses, and evidence of infection with either virus is not normally associated with pathological changes.
I n addition, the quantity of viral DNA detected in affected tissues is trivial, and there is no evidence of productive viral replication in any MCF-affected animals. It is concluded that MCF-susceptible species are not responsible for the spread of the virus, nor do they act as carriers. Disease in European wildlife has only been described in species of deer, although the susceptibility of North American bison to MCF suggests the potential susceptibility of European bison, while rare cases in domestic pigs does raise the possibility that wild boar could also be susceptible. The most convincing evidence of MCF in free-living wildlife is from a report from Norway in which disease was confirmed in moose (Alces alces), roe deer ( Capreolus capre- olus) and red deer (Cervus elaphus) over a 23-year period. Evidence of MCF in these animals on both histological and molecular virological grounds is compelling, and both OvHV2 and CpHV2 appear to have been involved. MCF in farmed deer is a relatively common disease, and in the early years of deer farming substantial outbreaks occurred both in the UK and in New Zealand. Disease in free-living animals has, however, never been reported in either country, despite the very substantial numbers of deer and sheep in both countries. It is noteworthy that, compared with the high incidence of MCF experienced in the first 10 years of deer farming in the UK, the disease is now sporadic and relatively uncommon.
Spectacular outbreaks of MCF in farmed North American bison have also been reported in herds that have only recently been subjected to relatively intense management(32).I t is tempting to speculate that the susceptibility of certain species may therefore be related to exposure to management systems that have not been optimized in favour of animal welfare.
It is also noteworthy that reports of MCF of pigs have most frequently been associated with Scandinavia, although there are also reports of the condition from Germany, Switzerland and the USA. In these cases the causal virus has been OvHV2, and there is no evidence that a variant form of the virus with greater infectivity for pigs has been involved. In addition, the breeds of pigs affected in these outbreaks have been varied, which suggests that susceptibility is unlikely to be determined by breed. It is thus concluded that as-yet unidentified environmental factors result in pigs becoming apparently more susceptible to infection in Scandanavia. In the absence of any other explanation, such unidentified factors may be impacting similarly on free-living deer in Norway.
PATHOGENESIS, PATHOLOGY
AND IMMUNITY
The most likely route of entry of the MCF viruses is the mucosa of the upper respiratory tract and the tonsils. The virus infects lymphocytes (CD8+ T cells); their role in the pathogenesis is unclear. Lymphoproliferation is likely to be the result of dysfunction of T- lymphocytes. Disturbed cytotoxic T-cell activity is probably involved in the development of vascular and epithelial lesions.
Gross pathological changes reflect the variable clinical signs and may involve most systems. MCF is characterized by erosions and ulcerations in the mucosae and in the skin, vasculitis and lymphoproliferation. Skin lesions are not infrequent in deer and may involve extensive alopecia, erosions and crusting dermatitis, primarily of the limbs and perineum. Bilateral corneal opacity and conjunctivitis are frequently present and catarrhal encrustation of the nares and oral cavity are often a feature, together with erosion of the epithelium.
Lymph nodes are generally enlarged and oedematous, and may be haemorrhagic. Haemorrhage of the intestinal mucosa is frequently present and can affect the abomasum and most sections of the large and small intestine. Characteristic lesions of the urinary bladder include petechiae and ecchymosis and the kidney frequently has raised white nodules, which are the result of lymphocytic accumulations.Presumptive diagnosis has relied on the detection of histological lesions characterized by epithelial degeneration, vasculitis, hyperplasia and necrosis oflymphoid organs and widespread accumulations of lymphoid cells in nonlymphoid organs. All epithelial surfaces may be affected and are characterized by erosion and ulceration with sub- and intra-epithelial lymphoid cell infiltration, which may be associated with vasculitis and haemorrhage.
Vasculitis affecting veins, arteries, arterioles and venules, but most typically medium- sized arterioles, is generally present and most pronounced in the brain (Figure 1.3). It is characterized by perivascular accumulation of lymphoid cells, and fibrinoid degeneration or necrotizing vasculitis, and there may be endothelial damage, which may lead to occlusion of vessels.
Lymph nodes characteristically are affected by lym- phoblastoid cell expansion in the paracortex and degeneration of follicles, and oedema and inflammation are present in the perinodal tissue. Interstitial accumulation of lymphoid cells, particularly in the renal cortex and periportal areas of the liver, are commonly present and may be exten-
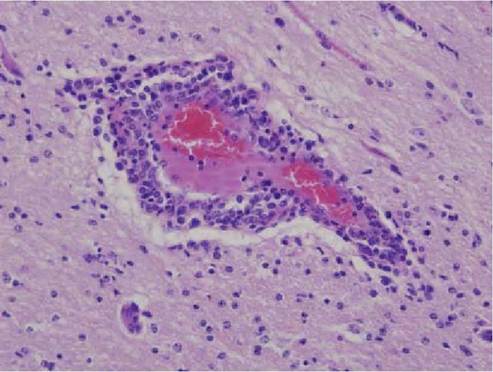
FIGURE 1.3 Histological section of farmed red deer brain with MCF, showing non- suppurative encephalitis. Note the characteristic accumulation of predominantly lymphoid inflammatory cells around the blood vessel (peri-vascular cuff) along with those free in the neuropil (gliosis, to the left of the blood vessel). Haematoxylin and eosin, original magnification ?100.
sive. Non-suppurative meningoencephalitis with lymphocytic perivascular cuffing is frequently present in the brain. Histological lesions of the cornea are characterized by lymphoid cell infiltration originating in the limbus and progressing centrally, and vasculitis, hypopyon and iridocyclitis may also be present.
The serological response of MCF-affected animals may be undetectable or directed at only a few viral epitopes, implying that there is only limited virus antigen expressed in diseased animals(33). The development of antibodies does not prevent a lethal outcome.
CLINICAL SIGNS
The clinical presentation of MCF is very variable and can involve most systems, ranging from peracute to chronic. In the peracute cases that have been observed in farmed deer, high fever, depression and profuse diarrhoea, which may be haemorrhagic, are the principle clinical signs. Generally, the course is more protracted and involves nasal and ocular discharges, which may be profuse and catarrhal, bilateral corneal opacity, enlarged lymph nodes, erosions in the oral cavity, erosion and/or hyperkeratosis of the skin and/or neurological signs involving blindness and behavioural changes. In chronic cases in deer, alopecia has also been a feature. In the cases involving wild deer, they were thin, often recumbent and showed a variety of clinical signs, including diarrhoea, abnormal behaviour, incoordination, blindness and convulsions1-26). Thus in light of the variability of the clinical presentation of MCF, this disease should be considered in any unexplained condition observed in deer.
DIAGNOSIS
I n suspected cases of MCF in wildlife, examination of tissues for evidence of characteristic histological lesions, especially in the brain, is the most appropriate method of achieving an initial presumptive diagnosis.
Of the viruses that have been associated with MCF, only AlHV-1 has been recovered in conventional tissue culture, although lymphoblastoid cell lines with limited productive virus replication have been propagated from animals affected with both AlHV1 or OvHV2 forms of the disease. Despite not being applicable as an aid to diagnosis, these lymphoblastoid cell lines have proved valuable in understanding the pathogenesis of disease and have provided a source of viral DNA. Such DNA has facilitated the sequencing of the genome of both viruses and permitted the selection of suitable PCR reactions for amplifying DNA sequences that detect either the MCF group of agents or are virus-specific(23). Such PCR reactions are now the method of choice for reaching a definitive diagnosis of MCF and identifying potential carrier animals.
All serological tests rely on AlHV1 antigens, as none of the other viruses can be productively replicated in tissue culture to provide virus specific reagents. The only critical report employing immunoblotting indicated that the sera of sheep and cattle infected with OvHV2 reacted erratically with AlHV1 antigens compared with sera of wildebeest(33). It is also known that serological tests for herpesviruses as a group can cross-react. Thus, despite a number of serological tests being available, caution in interpreting results when employing them with sera from novel species, which are almost certainly infected with their own specific herpesviruses, is essential. In addition, sera from free-living animals may be of variable quality, which has the potential to impact on the reliability of tests. The merit of surveys for evidence of infection with MCF viruses employing sera from free-living species of wild animals is thus questionable and the results should not be assumed to indicate evidence of the incidence of infection.
PUBLIC HEALTH CONCERN
There are no indications that MCF can infect humans.
MANAGEMENT AND CONTROL
Control of MCF is based on preventing contact between susceptible hosts and the natural carriers (sheep and goats).
ACKNOWLEDGEMENTS
The author acknowledges the contribution to the manuscript and the figures kindly provided by Dr Mark Dagleish (Moredun Research Institute).