25 Protein losing enteropathy in a dog
Initial presentation
Diarrhoea and weight loss
Signalment: 9-year-old neutered male Jack Russell terrier, body weight
5.3 kg
Case history
The dog presented with a 3-month history of diarrhoea, which had initially been intermittent, but had become more persistent during the previous month.
The faeces were described as soft to watery, containing no blood or mucus. He produced large volumes two to four times a day. He did not strain to defecate. He had lost about 0.5 kg during the previous month. He rarely vomited, but his appetite had decreased. His exercise tolerance was decreased and the owners thought he had become a bit quieter and less active in the house.He had previously been a healthy dog and was fully vaccinated yearly. He had been treated for internal parasites with a commercial product (unknown type) about 4 months prior to consultation. His usual diet was a commercial dry dog food and during the month prior to his consultation the owners had been adding canned tuna and other foods to encourage him to eat.
Physical examination
On physical examination the dog was quiet but alert and responsive. His body condition score was 4/9, with evidence of recent weight loss.
His mucous membranes were pink with a capillary refill time of range 3.6-12.0 ? 109∕l). Lymphopenia was present with a lymphocyte count of 0.46 ? 109∕l (reference range 0.7-4.8 ? 109∕l).
Serum chemistry results showed panhypoproteinaemia with a total serum protein concentration of 28 g∕l (reference range 58-75 g∕l), due to a decreased albumin concentration of 13.7 g∕l (reference range 26-35 g∕l) and decreased globulin concentration of 15.3 g∕l (reference range 18-37 g∕l). Total serum calcium concentration was decreased to 2.0 mmol/l (reference range 2.3-3.0 mmol/l), likely due to the decrease in the albumin bound fraction of calcium.
Clinical tip on hypocalcaemia with hypoalbuminaemia
Normally about 40% of the total serum calcium is bound to albumin, with about 10% chelated to anions and about 50% ionized and unbound. The ionized fraction is the biologically active fraction. With decreased albumin, the bound fraction is decreased, but the ionized fraction is often within the reference range and therefore clinical signs of hypocalcaemia are usually not seen. Ionized calcium can be measured to ensure that it is within the reference range.
The total calcium can also be ‘corrected’ for hypoalbuminaemia and while the accuracy of this calculation is questionable, it is useful as an estimation. The SI units must first be converted to conventional units, e.g. for this case:
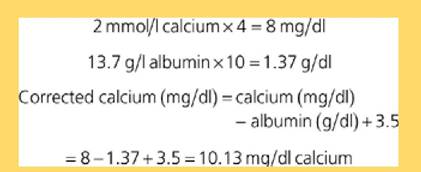
To convert this back to SI units, divide by 4, e.g. 10.13/4 = 2.54 mmol/l, which is within the reference range.
Serum cholesterol concentration was decreased to 1.7 mmol/l (reference range 3.8-7.0 mmol/l). Serum liver enzyme concentrations were moderately increased, with an alkaline phosphatase of 242 lU/l (reference range 20-60 lU/l) and ALT of 174 lU/l (reference range 21-102 lU/l).
Serum cobalamin concentration was decreased at 112 ng/l (reference range 215-908 ng/l) as was serum folate at 4.5 μg∕l (reference range 7.7-24.4 μg∕l).
Urinalysis results were unremarkable, with a urine specific gravity of 1.040. Urine protein to creatinine ratio was 0.05 (reference range in the jugular vein or threaded up the saphenous vein to the vena cava. Solutions of 400 to 650 mOsm/l may be administered via a standard catheter in a peripheral vein using a 1.2 micron in-line filter. When using a central line, the nutritional goal is to meet but not exceed the patient’s resting energy requirement, as calculated by body wt0∙75 ? 70 = daily kcal. Peripheral parenteral nutrition is an excellent way to provide partial nutrition for several days and either peripheral or central can be combined with partial enteral nutrition.
Further medical support included azathioprine at 2 mg/kg po q 24 hours, ranitidine at 2 mg/kg po q 8 hours and budesonide at 1 mg po q 24 hours. Budesonide is a locally acting corticosteroid which has high first-pass metabolism in the liver and therefore has minimal systemic side effects compared to other corticosteroids. Prednisolone was continued at a reduced dose of 1 mg/kg po q 24 hours. The dose was reduced as corticosteroids may be associated with an increased risk of pancreatitis. As the restricted protein home-cooked diet had not improved his clinical signs, he was changed to a canned low fat diet to decrease the risk of recurrent pancreatitis. Weekly subcutaneously injections of 250 μg cobalamin were given.
Clinical tip on cobalamin
Many cats and dogs with small intestinal disease are deficient in cobalamin (vitamin B12) and it is often necessary to supplement this parenterally. Weekly subcutaneous injections of cobalamin at 250 to 500 μg per patient are efficient in repleting serum cobalamin concentrations. Adequate serum cobalamin may be necessary for repair of the inflamed bowel.
The dog responded very well to the change in medication and the treatment with parenteral nutrition. His serum albumin concentration increased to 20.8 g/l and his serum globulin concentration increased to 19.2 g/l. His ascites resolved with the increase in serum protein concentrations. His appetite improved and his faecal consistency improved to a soft formed consistency.
Over the next 2 months (month 3 after diagnosis), the dog continued to improve in his appetite, stool quality and exercise tolerance. His weight increased to 5.65 kg. The jugular vein where the central line catheter had been placed did not fill when occluded and the presence of a thrombus was suspected. His serum proteins had improved, with an albumin concentration of 26.1 g/l and serum globulin concentration of 16.0 g/l.
Nursing aspects of jugular catheters
The main issues with indwelling catheters are the accumulation of thrombus and the risk of infection.
Thrombus formation starts the moment you puncture the endothelium of the vein and forms a sleeve around the catheter that either breaks and sloughs off or plugs the end. Thrombosis also starts away from the insertion site because the catheter tip irritates the vessel wall.Bacteria can be carried in during venepuncture or can be introduced to the catheter during injections, line changes or by having hair contaminating the hub at the time of iv line connection. Thrombi favour the accumulation of bacteria, which form biofilm that itself favours thrombosis. To reduce these sources of damage to the vessel and catheter, you can
1 use minimally traumatic venepuncture technique
2 use soft catheters
3 use sterile technique meticulously for every catheter placement and every subsequent use of the catheter.
It is often recommended to leave jugular catheters in for no longer than 3 days; however, if you are diligent with the care (and lucky), you can extend the catheter life for much longer than 3 days. If the clinical staff is not careful and meticulous, then even 3 days can be too long.
One month later (month 4 after diagnosis) the prednisolone dose was decreased to 0.8 mg/kg po q 24 hours while maintaining the other medications and diet. A month after that he was seen for a re-visit appointment. After decreasing the prednisolone dose the owners reported that the dog’s appetite had decreased, he had become more lethargic and his faeces had become softer. He had also lost 0.3 kg in body weight. The prednisolone dose was increased to 1 mg/kg alternating with 0.5 mg/kg every other day.
A month after the increase in the prednisolone dose the dog was seen for a re-visit appointment and the owner reported that he was brighter, exercising well and his stool quality had improved again. His weight had increased to 5.7 kg. His serum albumin concentration was 24.9 g/l and his serum globulin concentration was 15.6 g/l.
A month later the prednisolone dose was decreased to 0.5 mg/kg po q 24 hours and the dog remained fairly stable on this (plus the other medications and diet) for a further 5 months.
When he was seen at that time, he was showing signs of corticosteroid side effects, with mild abdominal distension, a sparse hair coat and hyperpigmentation on his ventral abdomen. The owners reported that the dog did urinate and drink more than prior to corticosteroid administration, but not excessively. His stools were reported to be soft and his weight was slightly reduced at 5.5 kg.At this visit his haematology showed a mild neutrophilia 19.6 ? 109/l (reference range 3.6-12.0 ? 109/l), likely due to the corticosteroid administration. Serum albumin concentration was 16.9 g/l and serum globulin concentration was 14.9 g/l. Abdominal ultrasound showed an increase in the small intestinal wall thickness to 6.8 mm (previously 6.0 mm), suggesting that potentially the inflammation had increased. The prednisolone dose frequency was decreased to 0.5 mg/kg po q 48 hours. At a re-visit 1 month (month 11) later the owners reported that the dog’s appetite had decreased, he had became lethargic, his faeces were softer and he had lost a further small amount (0.2 kg) of weight. The prednisolone dose was again increased so that he received 1 mg/ kg one day alternating with 0.5 mg/kg po every other day. Four months later (month 15) the dose was again decreased to 0.5 mg/kg po per day.
The dog was maintained on these medications and diet for a further 6 months (to month 21 after diagnosis) with a relatively good quality of life. Further attempts to decrease the dose to every other day resulted in reoccurrence of clinical signs.
At the 21 month revisit, the dog was found to again have diarrhoea, weight loss and a variable appetite. On physical examination a 3/6 systolic murmur was detected over the tricuspid valve. His serum albumin concentration was still decreased at 19.6 g/l.
There were decreases in his serum concentration of calcium (2.0 mmol/l; reference range 2.2-3.0 mmol/l), phosphorus (0.7 mmol/ l; reference range 0.9-2.0 mmol/l) magnesium (0.55 mmol/l; reference range 0.69-1.18 mmol/l) and potassium 3.2 mmol/l; reference range 3.6-5.6 mmol/l).
Echocardiography confirmed the presence of mild pulmonary hypertension; which may have been due to pulmonary thromboembolism. None of the chambers of the heart were enlarged and there was no evidence of hypertrophy.
Additional treatment at this time included a vitamin and mineral supplement plus oral calcitriol daily (2.5 ng/kg po q 24 hour). Weekly serum calcium concentration tests were scheduled to ensure that hypercal- caemia did not develop.
Outcome
The dog did not respond well to treatment at this time and remained thin and lethargic. Unfortunately at the next visit 2 weeks later to the hospital the dog had a cardiac arrest and died. Post mortem revealed a very large thrombus filling the right ventricle and pulmonary artery, which were highly likely to be the cause of death.
Discussion
Protein losing enteropathy (PLE) refers to the excessive loss of proteins into the gastrointestinal tract, which, if severe enough, causes a decrease in the plasma albumin and globulins. When serum albumin concentration is decreased, there is an increased risk of ascites and pleural fluid accumulation due to the loss of oncotic pressure. Causes of PLE include IBD (lymphocytic-plasmacytic, eosinophilic or granulomatous), neoplasia, foreign bodies, intussusception, lymphangiectasia, immune- mediated and allergic diseases.
Inflammation of the bowel increases the permeability, causing loss of proteins from the plasma and interstitium. In this dog’s case, there was also evidence of lymphangiectasia, which in adult animals is usually associated with obstructive lesions in the lymphatic vessels. The lymphatic stasis causes lymphatic hypertension, which causes interstitial fluid to leak into the abdomen and into the intestinal lumen. Lymphocytes are also lost into the intestinal lumen and dogs with lymphangiectasia often have a low lymphocyte count, although this finding is not very specific as stress or illness often causes lymphopenia.
Treatment of inflammatory bowel disease in small animals is somewhat empirical as there is a poor understanding of the underlying cause of the disorder, which may indeed be a collection of disorders with a commonality of histopathological changes. The mainstays of treatment include dietary therapy, corticosteroids, azathioprine, ciclosporin, antibiotics (e.g. tylosin or metronidazole) and possibly pre- or probiotics, in varying combinations. Where the side effects of corticosteroids become severe enough to decrease the dog’s quality of life, other medications (e.g. azathioprine or ciclosporin) should be added to try to decrease the corticosteroid dose without losing remission of disease.
As in this case, hypocalcaemia has been reported in protein losing enteropathies, which can be due to the low albumin; however, these changes can also occur due to malabsorption of vitamin D. Unabsorbed fatty acids can also bind dietary calcium to form insoluble salts which are not absorbed. Treatment with the calcitriol form of vitamin D was initiated in this case to try to increase intestinal calcium absorption.
Epidemiology
Most dogs with lymphocytic plasmacytic enteritis are middle aged to older, although it can occur in younger dogs. Breed related immunopro- liferative enteropathy is recognized in Basenjis and breed related protein losing enteropathies have been reported in soft coated wheaten terriers and Lundenhounds. Sharpei dogs also have an increased risk for inflammatory enteritis, likely related to IgG or IgA deficiencies. Many German shepherd dogs also have IgA deficiency which likely plays a role in chronic enteropathies. Anecdotally, some clinicians do believe that Jack Russell terriers may also be at risk for enteritis.
Prognosis
Inflammatory bowel disease can be difficult to control; in one study only 26% of dogs with IBD were considered to be in remission at a 6 month follow-up check. The presence of hypoalbuminaemia is a negative prognostic indicator and an elevated canine pancreatic lipase concentration is also associated with a negative outcome.
The long-term prognosis for dogs with PLE due to inflammatory causes is also guarded and most require long-term therapy. The prognosis for lymphangiectasia is also guarded.
As with other causes of protein loss, there can be loss of antithrombin, which has a similar molecular weight to albumin. This loss, along with vascular damage from immune complexes, may predispose these cases to the formation of thrombi. In this dog’s case, he had an additional risk factor due to the formation of a large thrombus in his jugular vein, which could have seeded other thrombi.
More on the topic 25 Protein losing enteropathy in a dog:
- Mucoid Enteropathy
- Subunit Protein-Based Vaccines
- Clostridium perfringens: Epizootic Rabbit Enteropathy
- Interference of the Nef Protein of HIV-1 with Pro- and Antiapoptotic Pathways of T Cells
- LOSING VALUE THE OLD-FASHIONED WAY
- ON LOSING YOUR CHILDREN IN THE VATICAN
- Enterococcus spp. Infection: Enterococcal Enteropathy
- 38 Colorectal neoplasia in a dog
- Post-modernism: Losing Philosophy
- The rate at which Earth is losing species is accelerating
- Clostridium difficile and Clostridium perfringens: Clostridial Enteropathy
- 14 Hypoadrenocorticism in a dog
- 16 Ingestion of glue by a dog
- 33 Intestinal leiomyoma in a dog
- VIRAL PROTEIN R (VPR): STRUCTURE AND FUNCTION IN THE VIRAL LIFE CYCLE