Clostridium difficile and Clostridium perfringens: Clostridial Enteropathy
Clostridial enteropathy is typically associated with stressors or situations that induce intestinal dysbiosis, allowing opportunistic overgrowth. Clostridial enteropathy occurs sporadically in the mouse due to infection with toxigenic C.
difficile and C. perfringens.Epizootiology and Pathogenesis
Clostridium difficile causes enteropathy in many species, including the laboratory mouse. Toxigenic C. difficile produces two exotoxins known as C. difficile Toxin A (TcdA) and Toxin B (TcdB). Clostridium perfringens may produce one or more major exotoxins that are associated with disease in many species. Exotoxins define C. perfringens into 5 major types (A through E). Type A is most often associated with production of enterotoxin, but any type can produce enterotoxin. Natural disease in laboratory mice has been associated with C. perfringens nontype A, type A, type B, and type D. Anecdotal observations have associated outbreaks with high carbohydrate diets, inadequate normal microbial flora in barrier-maintained pathogen-free colonies, reduced frequency of cage changing, and peak lactation.
Pathology
Enteropathy due to C. difficile has been common in mice from one commercial vendor. Lesions are similar to enteropathy associated with C. perfringens (below), and involve the small and/or large intestine. Clostrial enteropathy due to C. perfringens has been reported in mice ranging from 2 to 52 days of age and female mice of breeding age. Clinically affected mice have distended abdomens, soft feces, and sudden death. Both the small and large intestine may be dilated with gas and fluid, with mucosal hyperemia, petechiae, ulceration, and fibrinous pseudomembrane formation. Intestinal rupture and peritonitis may occur. In addition to inflammatory and hyperplastic changes in the mucosa of the small and/or large intestine (Fig. 1.53), multiple focal atypia were described in the duodenal mucosa of monocontaminated BALB/c mice, as well as atrial thrombosis and pulmonary inflammation.
Intestinal lumina contain large numbers of rod-shaped Gram-positive bacteria. Affected mice have generalized lymphoid apoptosis and renal tubular vacuolation. In the recovery phase, the intestinal mucosa may be diffusely or segmentally hyperplastic. Disease outbreaks have been reported among cesarean rederived mice that had been associated with a limited bacterial flora, recently weaned clean conventional mice, and C. perfringens-contaminated axenic mice.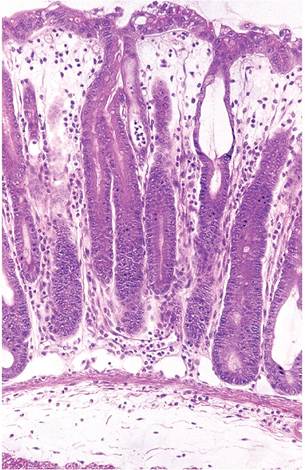
FIG. 1.53. Large intestine of a mouse naturally infected with Clostridium difficile. There is moderate hyperplasia of crypts with marked edema and leukocytic infiltration of the mucosa and submucosa.

FIG. 1.54. Postparturient lactating mouse with markedly dilated intestine filled with fluid and gas. The mouse has been skinned, and the intestine is visible through the unincised abdominal wall. This syndrome may be Clostridial in origin. (Source: Feinstein et al. 2008. Reproduced with permission from American Association for Laboratory Animal Science.)
A spontaneous disease, which has been termed “paralysis of peristalsis in lactating mice,” occurs in lactating dams of various genetic backgrounds, with mortality up to 40%. The syndrome is manifest as sudden death, usually during the second week of their first lactation. There may be fecal staining in the perineal region with distention of the abdomen. The stomach is usually slightly dilated and filled with watery fluid. The proximal small intestine is distended with fluid contents. Firm, conical fecal plugs may be present in the ileum and the tip of the cecum. Histological findings have been reported to be unremarkable, and pathogenic organisms were not recovered from the intestine or other tissues. More recently, similar syndromes have been described in which affected mice had segmental distention of the small intestine with fluid and gas (Fig.
1.54). Histology revealed widespread apoptosis of villus enter- ocytes, as well as surface epithelium in the large intestine. Clostridium perfringens A was incriminated in one report, in which mice had sudden death and necrohe- morrhagic enteropathy. These syndromes are likely to be Clostridial in origin, with the common feature of peak lactation.Diagnosis
A presumptive diagnosis can be based upon clinical history and intestinal lesions containing overgrowth of Gram-positive rods. Culture does not necessarily incriminate the bacterium, since they are often present without disease and may not be toxigenic. Although detection of exotoxins in the intestinal content is desirable, assays are generally not available, expensive, or insensitive due to lability of toxins. PCR can be used to speciate organisms and determine presence of toxin genes. Differential diagnoses include Tyzzer's disease and (in the recovery phase) causes of hyperplastic enteritides (Citrobacter, Helicobacter, E. coli, etc.).
More on the topic Clostridium difficile and Clostridium perfringens: Clostridial Enteropathy:
- Clostridium difficile, Clostridium perfringens, and Clostridium spiroforme: Clostridial Enteropathy
- Clostridium perfringens: Epizootic Rabbit Enteropathy
- Clostridium difficile Infection
- Clostridium piliforme Infection: Tyzzer’s Disease
- Clostridium botulinum Dysautonomia: Grass Sickness
- CHAPTER 36 CLOSTRIDIUM SPECIES AND BOTULISM
- Clostridium piliforme Infection: Tyzzer’s Disease
- Clostridium piliforme Infection: Tyzzer’s Disease
- Clostridial Diseases
- OTHER CLOSTRIDIAL DISEASES IN WILDLIFE