Clostridium piliforme Infection: Tyzzer’s Disease
Tyzzer's disease was first recognized and characterized by Ernest Tyzzer in 1917. He described an epizootic that decimated a colony of Japanese waltzing mice. The organism is now recognized to produce disease in a wide variety of other species, including rats, gerbils, hamsters, guinea pigs, and rabbits, but there is evidence for some degree of species specificity among different isolates.
For decades, the causative agent was called Bacillus piliformis. However, based on 16S rRNA gene sequence analysis, it is now classified as C. piliforme. The organism is a spore-forming, Gram-negative, filamentous bacterium that can only be propagated in living cells.Epizootiology and Pathogenesis
Infection occurs by ingestion of spores. Shed in the feces, spores can survive in contaminated bedding for at least 1 year, and in the natural environment for at least 5 years. Vertical transmission does not occur under natural conditions, although intrauterine transmission has been produced experimentally in mice inoculated intravenously. Based on serological assessment, up to 80% or more of clinically normal mice from known infected colonies may have detectable antibodies to the organism. Outbreaks of Tyzzer's disease in mice are usually characterized by low morbidity and high mortality in affected animals. Mouse strain, age, and immune status are factors in susceptibility to the disease. For example, DBA/2 mice are susceptible, and B6 mice are resistant to Tyzzer's disease. Depletion of NK cells in resistant adult B6 mice, but not DBA mice, rendered them more susceptible, and neutrophil depletion rendered both juvenile DBA and B6 mice more susceptible to disease. Macrophage depletion did not appear to influence susceptibility to disease. Infected DBA and B6 mice develop elevations in IL-12, and neutralization of IL-12 renders infected mice more susceptible to disease.
Disease resistance also appears to be due, at least in part, to B-lym- phocyte function. CBA/N and C3.CBA/N mice, which are B-cell-deficient, have been found to be more susceptible than immunocompetent or T-cell-deficient nude mice. T-cell-deficient nude mice were shown to be as resistant to the disease as immunocompetent mice. However, in one report of a spontaneous outbreak of Tyzzer's disease in a colony of nude mice, homozygous nude mice were particularly susceptible to high mortality compared with heterozygous mice. These apparent differences in nude mouse susceptibility may be related to the C. piliforme isolate, as the virulent isolate proved to be the first toxigenic isolate recovered from mice. In outbreaks of Tyzzer's disease, predisposing factors include overcrowding, poor sanitation, and experimental procedures that may compromise the immune response.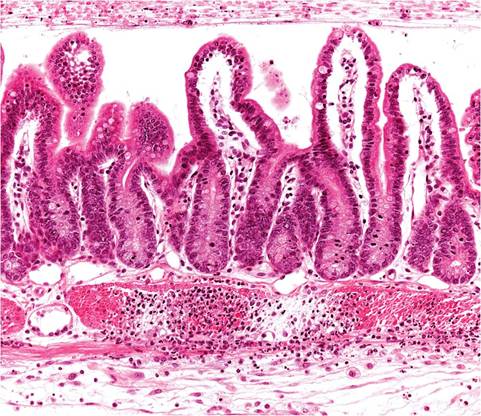
FIG. 1.55. Small intestine of a mouse with acute Tyzzer's disease due to Clostridium piliforme. Villi are blunted and there is acute necrosis of the muscularis mucosae.
Pathology
Infection is often subclinical, but sudden death and diarrhea may occur in immunodeficient mice. The primary lesion arises in the mucosa of the intestine, with grossly visible reddening of the ileum and cecum. Microscopically, foci of degeneration, inflammation, edema, and necrosis are evident in the intestinal mucosa and muscularis mucosae (Fig. 1.55). Clusters of organisms are apparent in enterocytes, but also in the smooth muscle and neurons of Auerbach's plexus. Lymphatic vessels and sinuses of mesenteric lymph nodes may contain cellular debris. Miliary pale foci or larger umbilicated foci are usually visible throughout the parenchyma of the liver (Fig. 1.56), and foci can be particularly large and umbilicated in immunodeficient mice. Lesions are characterized by multifocal coagulation to caseation hepatic necrosis, with polymorphonuclear leukocyte infiltration.
Gray foci in the ventricular myocardium may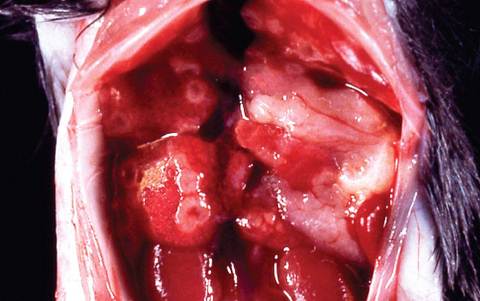
FIG. 1.56. Liver of a mouse with Tyzzer's disease. Note the multiple pale umbilicated lesions on the capsular surface. (Source: R. Bunte. Duke University, Singapore. Reproduced with permission from R. Bunte.)
also be present, with myocyte degeneration, myocarditis, and intracellular bacteria. In tissue sections stained with the Warthin-Starry, Giemsa, or PAS methods, typical intracytoplasmic bundles of bacilli are usually readily found in enterocytes, hepatocytes adjacent to necrotic foci, and myocardial cells (see Gerbil Chapter 4, “Clostridium piliforme Infection”).
Diagnosis
The diagnosis of Tyzzer's disease can be confirmed by demonstration of the pathognomonic clusters of intracellular bacilli in tissue sections, using the appropriate stains. The typical bacilli may also be visualized in impression smears prepared from liver lesions and stained using the Giemsa method. Serologic assays are available and utilize whole bacterial lysates as antigen, but have proven to be inaccurate due to the antigenic diversity among C. piliforme isolates. Clostridium piliforme can be isolated by inoculation of embryonated hen's eggs, primary mouse or chick embryo cell cultures, primary mouse or chick liver cells, and several continuous cell lines. PCR amplification of C. piliforme in feces is an effective method of detection. The cortisone provocation test may be warranted to test for subclinical carrier animals. Differential diagnoses include diseases such as MHV infection, mousepox, salmonellosis, pseudomo- niasis, corynebacteriosis, infections with Helicobacter spp., and Clostridial enteropathy.
More on the topic Clostridium piliforme Infection: Tyzzer’s Disease:
- Clostridium piliforme Infection: Tyzzer’s Disease
- Clostridium piliforme Infection: Tyzzer’s Disease
- Clostridium difficile Infection
- TYZZER'S DISEASE
- Clostridium difficile, Clostridium perfringens, and Clostridium spiroforme: Clostridial Enteropathy
- Clostridium difficile and Clostridium perfringens: Clostridial Enteropathy
- Characteristics of Infection and Disease
- Characteristics of Infection and Disease
- Fusobacterium necrophorum Infection: Schmorl’s Disease, Necrobacillosis
- Corynebacterium bovis Infection: Coryneform Hyperkeratosis; Scaly Skin Disease
- Immunology of Paratuberculosis Infection and Disease
- EVIDENCE FOR AN INFLUENCE OF APOPTOSIS IN DISEASE PROGRESSION IN LENTIVIRUS INFECTION
- CONTRIBUTION OF VITAMIN D ON PROTECTION/RISK TO HIV INFECTION AND DISEASE PROGRESSION TO AIDS