Clostridium difficile, Clostridium perfringens, and Clostridium spiroforme: Clostridial Enteropathy
For years, C. perfringens was regarded as the likely etiology of enterotoxemia in domestic rabbits. Type E iota toxin was demonstrated in fatal cases of enterotoxemia, and the disease was, therefore, attributed to C.
perfringens. Some of these diseases associated with C. perfringens may have been due to C. spiroforme, since antitoxin prepared against C. perfringens type E iota toxin will also neutralize similar toxins produced by C. spiroforme. Fatal colitis and enterotoxemia associated with overgrowth of C. difficile has occurred following prolonged treatment with penicillin or ampicillin. Subsequent experimental reproduction of the disease following treatment with lincomycin was attributed to C. difficile or C. perfringens. Spontaneous enterotoxemia due to C. difficile infection, with identification of A and B toxins, has been reported in specific-pathogen-free rabbits in the absence of prior antibiotic treatment. Clostridial enterotoxemia has similar features in rabbits, regardless of causative Clostridium spp.Epizootiology and Pathogenesis
Clostridium spiroforme is now recognized as the most common clostridial pathogen associated with enterotoxemia in young rabbits. In 1 survey of diarrheic rabbits, C. spiroforme was isolated from over 50% at necropsy, and 90% of the strains isolated were toxigenic. Although this organism is not a normal inhabitant of the alimentary tract in rabbits, it is often difficult to produce disease experimentally in healthy rabbits inoculated orally with C. spiroforme. The normal gut microbiome acts as a microbial barrier, and disruption of the normal gut microflora is an important predisposing factor. Changes in feed, weaning, previous antibiotic treatment, and concurrent infections appear to permit colonization with C. spiroforme and thus trigger an epizootic of enteric disease. The term “carbohydrate overload” has been associated with the syndrome.
Rabbits ingesting high- energy feed may fail to digest the majority of carbohydrates in the small intestine. Significant amounts of carbohydrate may then reach the level of the large intestine, promoting the overgrowth of organisms such as Clostridia. In outbreaks of the disease, the organism may be the sole identified pathogen. However, concurrent infections with other pathogens, such as rotavirus, E. coli, Eimeria spp., and Cryptosporidium spp. are often present. Following the multiplication of pathogenic strains of Clostridium spp. in the large intestine, enterotoxins may be produced, resulting in damage to enterocytes, impaired function, profuse diarrhea, subsequent depression, dehydration, and death.Pathology
In peracute cases, the carcass is usually in good condition, and perineal soiling with diarrheic feces is a variable finding. In subacute to chronic cases, carcasses are frequently thin and dehydrated. Staining of the perineum, belly, and rear legs with watery green to tarry brown feces is common. Internally, straw-colored fluid may be present in the peritoneal cavity. Extensive ecchy- moses are usually present in the cecal serosa, sometimes with involvement of the distal ileum and proximal colon. Epicardial and thymic ecchymoses may also occur. The cecum and adjacent areas are frequently dilated, with watery to mucoid, green to dark brown contents, and with gas formation. There may be marked thickening of affected areas due to submucosal edema, and mucosal changes vary from hemorrhage to ulceration and fibrinous exudation (Fig. 6.28).
Typical microscopic changes in the cecum of affected animals are those of a necrotizing typhlitis, with irregular denuding of the mucosa, ulceration, fibrinous exudation, and leukocytic infiltration, with heterophils predominating (Fig. 6.29). Changes observed in enter- ocytes vary, including swelling, vacuolation, flattening, denuding, and proliferation. The mucosa and submucosa are congested and edematous, frequently with focal hemorrhage, and thrombi may be present in adjacent vessels.
Gram-positive bacilli may be present in large numbers on the surface of affected areas of gut mucosa. The optimal lesion (for diagnosis) is selective necrosis of mucosal epithelium, with relative sparing of the crypt bases and lamina propria, submucosal edema, and mucosal/submucosal/serosal hemorrhage. All of these features relate to the effects of luminal toxin penetrating to various depths of the intestinal wall. In subacute to chronic lesions, necrotizing changes are replaced by hyperplasia as the mucosa undergoes repair.
FIG. 6.28. Cecum from a rabbit with clostridial enteropathy. Note the hemorrhage and the fibrinous exudate on the mucosal surface.
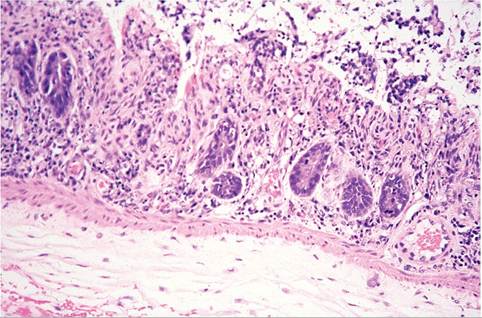
FIG. 6.29. Necrotizing typhlitis from a case of clostridial enteropathy due to Clostridium spiroforme. Note the selective loss of mucosal epithelium with relative sparing of crypts and submucosal edema.
In this stage, clinical signs of malabsorption and diarrhea continue. Clinical support of the rabbit has often been stopped at this stage, under the erroneous assumption that the rabbit was not improving. When rabbits are presented for necropsy following death, autolysis and postmortem bacterial overgrowth can obscure mucosal lesions. However, clostridial enteropathy would be a likely candidate based on the presence of submucosal edema and hemorrhage.
Diagnosis
The typical age (usually juvenile) and history of a change in feed, management, or environment may be helpful, particularly if coinciding with an explosive outbreak of diarrhea. The microscopic examination of Gram-stained smears from the terminal ileum and cecum is a useful procedure to make a provisional diagnosis. Typical curved and coiled Gram-positive organisms are associated with C. spiroforme infections (Fig. 6.30). Anaerobic cultures are recommended for positive identification of
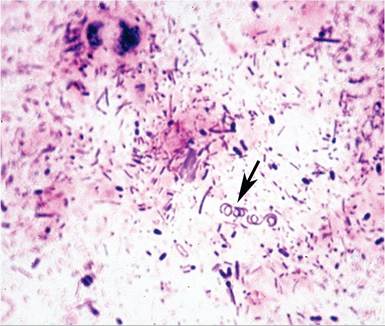
FIG. 6.30. Gram-stained smear of intestinal contents from a rabbit with clostridial enteropathy, demonstrating the typical coiled appearance of Clostridium spiroforme organisms (arrow).
the organism, and PCR protocols have been developed that identify the organism and its toxin-encoding genes. Several procedures are available for the identification of the clostridial toxin recovered from gut contents or bacterial culture. Semiquantitative aerobic bacterial cultures of small intestine and cecum provide a useful index of dysbiosis, since aerobic bacteria should be absent or minimal in the normal intestine. Fecal flotation and virology screening are procedures recommended in order to search for possible concurrent infections. Differential diagnoses include coccidiosis, E. coli infections, and Tyzzer's disease.