Clostridium difficile Infection
Unlike other species covered in this text, C. difficile enterotoxemia is rare in rats. Nevertheless, germ-free rats that were experimentally monoassociated with toxigenic C. difficile developed pseudomembranous colitis.
Thus, laboratory rats may, under certain circumstances, develop enterotoxemia.Clostridium piliforme Infection: Tyzzer's Disease
The Tyzzer's bacillus, C. piliforme, was previously named Bacilluspiliformis, which gave rise to the sometimes used, but inappropriate name of Clostridium piliformis. It has a wide host range, but C. piliforme isolates tend to be hostspecific, with minimal antigenic cross-reactivity among isolates. Infection involves the vegetative form, and spores are shed in the feces, which may remain infectious in contaminated bedding for up to 1 year (for additional information on epizootiology and pathogenesis, see Rabbit Chapter 6, “Clostridium Piliforme Infection”). Outbreaks in laboratory rats usually occur in young rats during the postweaning period. Transmission is achieved through oral ingestion of spores. Transplacental transmission has been demonstrated in seropositive rats treated with prednisolone during the last week of pregnancy. Subclinically infected rats can transmit the organism to naive rats via contaminated bedding, but the organism can be eliminated from immunocompetent rats by cesarean section and appropriate disinfection techniques. Tyzzer's disease is typically an enterohepatic disease, with variable involvement of the heart. In naturally occurring outbreaks, clinical signs may include depression, ruffled hair coat, abdominal distension, low morbidity, and high mortality in clinically affected animals. Clinical disease with low mortality has also been reported. Clinically normal seropositive rats have been identified in colonies, indicating that inapparent infections may occur.
Pathology
Rats with Tyzzer's disease may develop necrohemorrhagic ileitis, with pronounced dilation of the terminal small intestine (megaloileitis) (Fig. 2.27). The flaccid ileum may be distended up to 3-4 times the normal diameter, with variable involvement of the jejunum and cecum. Megaloileitis does not always occur in rats with Tyzzer's disease. Enteritis may be evident only at the microscopic level. The mesenteric lymph nodes are swollen and edematous. Disseminated pale foci of necrosis up to several millimeters in diameter are scattered throughout the parenchyma of the liver. They may also be circumscribed to linear pale foci present on the heart (Fig. 2.28). Microscopic changes are confined primarily to the ileum, liver, and myocardium. In the intestine, there is frequently a necrotizing transmural ileitis, with segmental involvement of affected areas. There is necrosis and sloughing of enterocytes and edema of the lamina propria and submucosa, often with fragmentation and hypercellular- ity of the muscular layers. Infiltrating inflammatory cells are primarily mononuclear cells, with a sprinkling of neutrophils. In the liver, the histological characteristics vary from foci of acute coagulation necrosis to focal hepatitis, with polymorphonuclear and mononuclear leukocyte infiltration (Fig. 2.29). Hepatic lesions of some duration are characterized by fibrosis, with
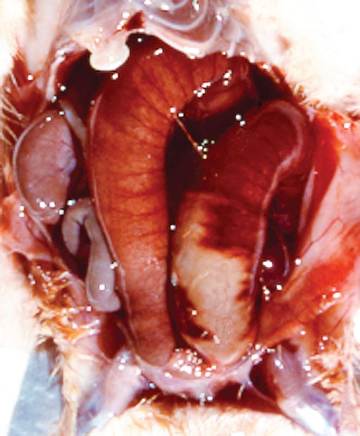
FIG. 2.27. Tyzzer's disease, manifesting as necrotizing and hemorrhagic ileitis with adynamic ileus (megaloileitis) in a young rat infected with Clostridium piliforme.
multinucleated giant cells and mineralized debris in reparative foci. In the heart, lesions may vary from necrosis of isolated myofibers to destruction of relatively large segments of myocardium. There is vacuolation to fragmentation of the sarcoplasm, with interstitial edema and mononuclear and polymorphonuclear leukocyte infiltration.
Giemsa, Warthin-Starry, or PAS stains may used to demonstrate bundles of slender bacilli in the cytoplasm of enterocytes in ileal lesions, in hepatocytes surrounding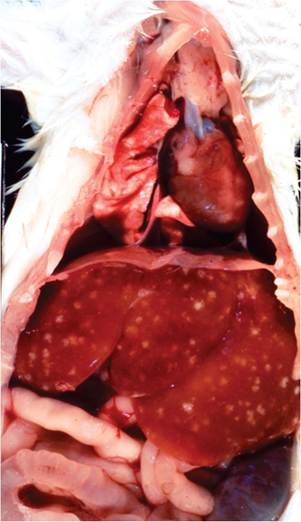
FIG. 2.28. Tyzzer's disease in a young rat. Note the multifocal
hepatitis and the multifocal to coalescing myocardial lesions.
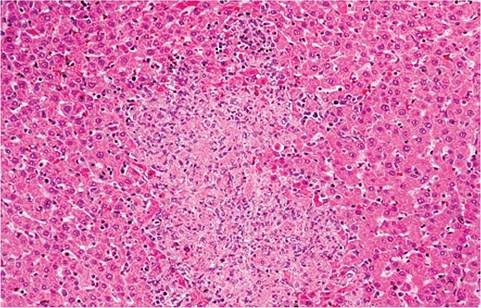
FIG. 2.29. Tyzzer's disease in a juvenile rat. There is acute focal necrosis of hepatocytes with polymorphonuclear cell infiltration.
necrotic foci, and scattered in the sarcoplasm in myocardial lesions (Fig. 2.30).
Diagnosis
Diagnosis is achieved by the demonstration of the organisms in tissue sections. Visualization of diagnostically typical fascicles of intracytoplasmic bacilli, particularly in liver, may require arduous searching. The triad of organs usually affected in Tyzzer's disease (intestine, liver, and heart) are also useful diagnostic features, if present. Serologic tests are now widely used, but use of a single isolate as antigen may not detect seroconversion among different host species (including between mice and rats) due to significant antigenic heterogeneity. PCR has also been developed for detection of the organism in feces. Differential diagnoses include salmonellosis and ileus following the intraperitoneal administration of chloral hydrate for general anesthesia.