34 Corticosteroid induced gastrointestinal ulceration in a dog
Initial presentation
Weakness, lethargy, muscle wasting, soft dark faeces
Signalment: 7-year-old neutered female Labrador retriever, body weight
21.8 kg
Case history
This dog had a history of immune mediated thrombocytopenia the previous year, which had responded to oral methylprednisolone.
Two months prior to admission her platelet count had dropped to 136 ? 109/l (reference range 200-500 ? 109∕l) and the referring veterinary surgery had again initiated oral methylprednisolone at 1.5 mg/kg body weight divided into two treatments per day. She had been maintained on this dose. Serum chemistry performed by the referring veterinary surgery had documented increased alanine aminotransferase (ALT) and alkaline phosphatase (AP), although the values were not recorded.The owner was concerned that the dog was very lethargic and had very poor exercise tolerance. She reported that the dog had increased urination and thirst and a very good appetite. She was not vomiting, although had had several episodes of diarrhoea with soft, dark faeces.
The dog’s usual diet was a low calorie dry food and she was normally fed twice a day. She had previously been on glucosamine and chron- droitin sulphate for arthritis, but these had not been administered during the previous 2 months. She was on no other medications or supplements. She was current on her vaccinations but had not been de-wormed for about a year.
Physical examination
The dog was quiet but responsive. Her body condition score was approximately 5/9, although this was hard to determine as she had moderate muscle wasting with retention of body fat.
Her capillary refill time was less than 2 seconds. Her mucous membrane colour was pale pink and her membranes were tacky. She was estimated to be about 6% dehydrated.
Thoracic auscultation revealed normal heart and lung sounds, with a heart rate of 76 beats per minute and a respiratory rate of 14 breaths per minute.
There was no evidence of pain on abdominal palpation, but the abdomen was pendulous and felt soft. Her rectal temperature was 38.4° C. Her coat was dry and showed evidence of seborrhoea.Problem list and discussion of problems
The dog’s problems included:
• Lethargy and poor exercise tolerance
• Pale, tacky mucous membranes
• Muscle wasting
• Pendulous abdomen
• Possible polyuria and polydipsia • Elevated liver enzymes
Differential diagnosis
Many of this dog’s problems may have been due to the administration of corticosteroids, but they were still explored as this assumption can result in missing a disorder.
Lethargy and exercise intolerance have many differential diagnoses, but for this dog the list included anaemia, hepatopathy, electrolyte disturbances, hypoglycaemia, corticosteroid induced myopathy, cardiopulmonary disorders and renal disease.
The slightly tacky membranes were likely indicative of mild dehydration due to the polyuria.
The pale mucous membranes may have been due to poor perfusion or anaemia. The heart sounds were regular and on palpation her pulses felt normal, making anaemia the more likely diagnosis. Anaemia may be divided into non-regenerative or regenerative, which is determined by performing a reticulocyte count. Non-regenerative anaemias are due to systemic diseases suppressing bone marrow function or primary bone marrow disorders. Regenerative anaemias are due to blood loss or haemolysis. Gastrointestinal blood loss is always a potential problem in animals on corticosteroid treatment.
The muscle wasting was typical of that induced by corticosteroids, but can also be caused by myopathies or weight loss due to illness, where muscle loss can be more prominent than fat loss.
The pendulous abdomen on this dog may have been due to the administration of corticosteroids, which cause muscle weakness and abdominal deposition of fat. Other causes for the abdominal enlargement included ascites or organomegaly.
The polyuria and polydipsia are common side effects of corticosteroids, but other common or concurrent disorders like renal disease, urinary tract infection, endocrine disorders or electrolyte disturbances were also included in the differential diagnoses list.
The elevation in liver enzymes may be due to corticosteroids or primary or secondary liver disorders.
Dark faeces can indicate melaena (the presence of digested blood in the faeces). Usually the stools are described as being dark and tarry. The black colour is a result of the oxidation of haemoglobin and the tarry appearance is from the bacterial breakdown of haemoglobin. Generally melaena is thought to be from bleeding from the upper intestinal tract or from the ingestion of blood (e.g. from epistaxis or oral lesions). Blood must be present in the gastrointestinal tract for several hours (8 hours in humans) before the colour turns black, so a rapid transit time of blood may not show melaena and a very slow transit time may show as melaenic faeces from a bleed in the lower gastrointestinal tract.
Clinical tips for diagnosing gastrointestinal bleeding
In dogs 350 to 500 mg of haemoglobin per kilogram of body weight must enter the gastrointestinal tract before melaena is seen, so gastrointestinal bleeding without the overt presence of melaena is very possible. A faecal occult blood test is useful to rule out melaena.
With chronic gastrointestinal bleeding, iron is lost from the body and an iron deficient anaemia may develop. Iron deficiency anaemias become microcytic and hypochromic. More acute bleeding can cause a significant drop in the packed cell volume (PCV), even within hours.
The serum urea nitrogen to creatinine ratio increases with upper gastrointestinal bleeding due to the absorption of blood protein. An increased serum urea with a creatinine within the reference range (or other similar disproportionate changes) should prompt the clinician to check for gastrointestinal bleeding.
The use of diuretics can also cause this change.Faecal occult blood tests using orthotolidine or guaiac tablets are qualitative and only moderately sensitive. It is recommended to feed a meat-free diet (e.g. cottage cheese and rice) for 3 days prior to collecting the faecal sample as the myoglobin from meat in the diet may interfere with the test, causing a false positive.
Case work-up
The dog was admitted to the hospital and rehydrated with intravenous crystalloid fluids.
Minimum data base
Haematology, serum chemistry and routine urinalysis were performed. Haematology showed a regenerative anaemia with a PCV of 0.277 l/l (reference range 0.39-0.55) and an uncorrected reticulocyte count of 2%. The reticulocyte corrected to 1.23% as determined by correction for her PCV and indicated a mild degree of regeneration. The platelet count was within the reference range at 218 ? 109 (reference range 200-500 ? 109∕l).
Clinical tip on correcting reticulocyte counts
Reticulocyte counts are necessary for an objective assessment of the degree of RBC regeneration, but the count should be assessed with consideration of the degree of anaemia. One way to ‘correct’ the reticulocyte count is with the following formula: 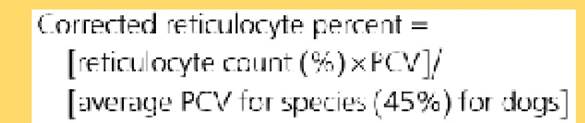
Results: 1 to 4%: Slight regeneration
5 to 20%: Moderate regeneration
>20%: Marked regeneration
Another way to assess the degree of regeneration is to multiply the % reticulocytes ? RBC ? 10. This is greater than 60,000 cells∕μl in regenerative anaemias.
Serum chemistry confirmed the elevation in liver enzymes, with AP of 1454 IU∕l (reference range 20-60 IU∕l) and ALT of 815 IU∕l (reference range 21-102 IU∕l). Serum fasting bile acid concentration was also increased to 43.9 μmol∕l (reference range 0-7 μmol∕l) and serum bilirubin was increased to 10.9 mmol∕l (reference range 0-6.7 mmol∕l).
Total calcium was decreased to 1.9 mmol∕l (reference range 2.3-3.0 mmol∕l) with albumin just below the reference range at 25.2 g∕l (reference range 26-35 g∕l).
The true albumin value may have been lower than this as haemoconcentration could have increased the apparent serum albumin concentration. The serum ionized calcium was normal at 1.1 mmol∕l (reference range 1.1-1.5 mmol∕l). Although serum amylase and lipase were within the reference ranges, a canine-specific lipase test was submitted. This result, which was available about 2 weeks later, was 271 μg∕l (reference range 0-200 μg∕l), indicating a mild to moderate pancreatopathy. Clotting times (activated partial thromboplastin time and prothrombin time) were within the reference ranges.Urinalysis was unremarkable other than a urine specific gravity of 1.011, which was inappropriately low for a dog with dehydration. This again was likely to have been affected by the administration of corticosteroids, but could also have been caused by renal disease or other disorders affecting urine concentrating ability. Urine culture was negative.
Coombs test
A Coombs test, which was run to help rule out immune mediated haemolysis, was negative, although corticosteroid administration can cause false negative results. The increase in bilirubin can be consistent with haemolysis, but also with liver disorders. There was no haemoglobin- uria, which can occur with haemolysis, but haemolysis was still a possibility.
Faecal analysis
Faecal analysis for parasites was negative and faecal culture for enteropathogens was also negative. A faecal occult blood test was performed after feeding the dog cottage cheese and rice for 3 days and this was positive for occult blood. A positive faecal occult blood test is indicative of either gastrointestinal bleeding or swallowed blood. As there was no evidence of nasal or oropharyngeal bleeding in this dog, gastrointestinal blood loss was most likely.
Differentials for a positive faecal occult blood in this dog included:
• Clotting disorders, although this dog had normal coagulation parameters and platelet count, a platelet function disorder was possible.
• Gastrointestinal ulcers, which can be caused by drugs, especially nonsteroidal anti-inflammatory or corticosteroid administration, inflammation, neoplasia such as adenocarcinoma or lymphoma, sharp foreign bodies, gastrointestinal ischaemia (e.g. volvulus, shock), abnormal vasculature.
• Gastrointestinal parasites may also cause GI blood loss and although the faecal parasitology was negative, she was treated with 3 days of fen- bendazole at 50 mg/kg/day po.
Imaging
Abdominal ultrasound examination showed a large hyperechoic homogeneous liver, an enlarged right pancreatic lobe and free peritoneal fluid (Figs 34.1 and 34.2). The adrenals were both small (Fig 34.3). The stomach appeared hypomotile. A sample of the fluid was obtained and a Tru-Cut liver biopsy was taken.

Fig 34.1
Ultrasound picture of the liver and spleen, showing a mottled hy
perechoic appearance to the liver
(courtesy of Carolina Urraca del Junco).
Fig 34.2

Ultrasound picture of the pancreas, showing an enlarged right pan
creatic lobe (R = right)
(courtesy of Carolina Urraca del Junco).

Fig 34.3
Ultrasound picture of the left adrenal gland, which is very small in size (as was the right adrenal gland)
(courtesy of Carolina Urraca del Junco).
Abdominal fluid and liver biopsy analysis
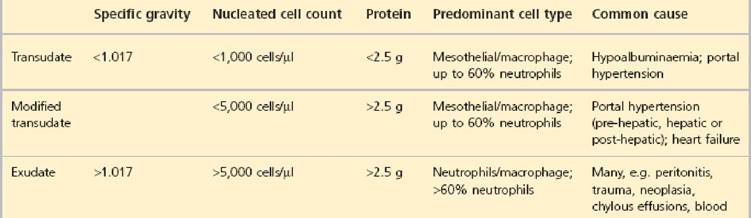
The abdominal fluid had a low specific gravity of 1.015, low protein content of 2.4 g/l and moderate cellularity with a count of 6.1 ? 109/l. Neutrophils were predominant, comprising 80% of the cells, with 20% macrophages and the rest lymphocytes and mesothelial cells. The neut-
rophils were hypersegmented. The poor correlation of the cellularity and the low protein content made it impossible to classify the fluid into a distinct category (Table 34.1). The fluid was cultured and was negative for bacterial growth.
Table 34.1 Clinical tip: determining the type of ascites
The liver biopsy results showed severe diffuse, midzonal to periportal hepatocellular swelling and clearing consistent with a corticosteroid hepatopathy.
Gastrointestinal endoscopy
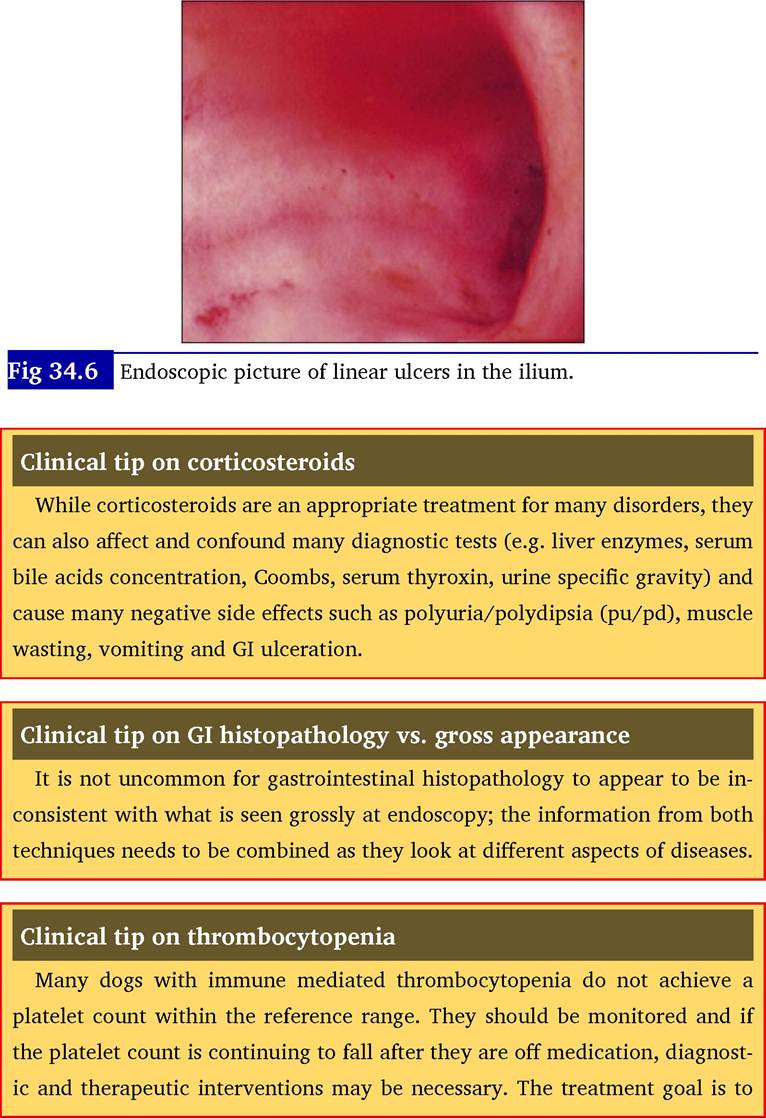
At endoscopy the lower oesophagus was found to be inflamed (Fig 34.4) and there were multiple areas of ulceration within the stomach (Fig 34.5), duodenum and ileum (Fig 34.6). Histopathology of pinch biopsies of the stomach, duodenum, ileum and colon all showed signs of inflammation.
Fig 34.4

Endoscopic picture of oesophagitis, showing reddening of the distal
oesophagus at the junction with the gastro-oesophageal sphincter.
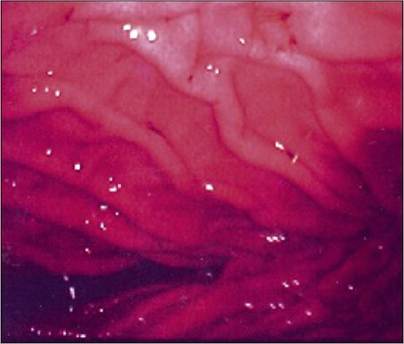
Fig 34.5
Endoscopic picture of pinpoint ulcers in the cardia of the stomach.
The retroflexed endoscope can be seen in the lower left of the picture.
prevent clinical signs of thrombocytopenia, not achieve a number within the reference range.
Medical treatment options
Two aspects of the treatment of the case were addressed: the oesophagitis and gastric bleeding, and the hepatopathy.
The oesophagitis and gastric bleeding were treated with ranitidine (2 mg/kg po q 12 hours) for its antacid and promotility effects and liquid sucralfate (3 ml po q 8 hours) for its ulcer binding and prostaglandin secretion effects. A short course of clavulanate-amoxicillin (16 mg/kg po q 12 hours) was administered, as gastrointestinal bleeding can predispose to bacterial translocation.
The dose of oral methylprednisolone was decreased over about a 1-month period while monitoring the platelet count, which continued to be stable. As soon as the dose was approximately 0.5 mg/kg, every other day dosing was administered, as this allowed the animal to have a ‘recovery’ day from the effects and usually markedly decreases the side effects. The hepatopathy was treated with ursodeoxycholic acid (10 mg/ kg po q 24 hours), S-adenosyl methionine and vitamin E (Hepatosyl™) at three capsules twice a day po for their positive effects on the hepatocytes.
Outcome
The dog recovered very well, with the PCV rising to 0.33 l/l and the liver enzymes dropping to approximately half the values at presentation within 6 weeks. The owner reported an improvement in energy, muscle mass, pu/pd and coat quality.
Discussion
Drugs are a very important cause of gastrointestinal ulceration in the dog. While there is some controversy whether all corticosteroids are severely ulcerogenic, most clinicians agree that high doses of dexamethasone have the potential for significant gastric erosion. Prednisolone by itself is not generally severely ulcerogenic unless it is used in high doses (e.g. >1-2 mg/kg/day) or for long terms; however, some individual dogs are especially sensitive to the effect. Many clinicians feel that larger breeds of dogs are more at risk. Any dog which becomes anaemic, has melaena or an increased serum urea, should be investigated for potential gastrointestinal bleeding, especially if it is on corticosteroid treatment.
Prognosis
The prognosis for dogs with gastrointestinal ulceration depends upon the severity of the ulcers. Some cases can rapidly develop perforating ulcers which can cause a fatal peritonitis and some resolve with cessation of the inciting drug. In any patient on corticosteroids or non-steroidal anti-inflammatory medications gastrointestinal signs, pale mucous membranes or a decrease in PCV should be addressed promptly.