2 Idiopathic megaoesophagus in a dog
Initial presentation
Vomiting and regurgitation every 1 to 3 days for at least 6 months; concurrent weight loss and recent (2 to 3 weeks) cough
Signalment: 2-year-old neutered male German shepherd dog, body weight 23.1 kg
Case history
The dog had been obtained from a rescue centre 6 months earlier.
The owner said that he was de-wormed regularly with a product from the grocery store and had been vaccinated at the time they obtained him.He was usually bringing up food that appeared undigested and did not contain bile, although occasionally he also did bring up digested food and bile. There was no abdominal effort and he would bring up the food from minutes to about an hour after eating. It was determined that he was usually regurgitating, although sometimes there was an episode of true vomiting.
He was coughing occasionally during the previous 2 weeks and his exercise tolerance had decreased. The dog’s stools had been normal and his water intake and urine output had not changed. The owner estimated that the dog had lost about 8 kg over the last couple of weeks.
His usual diet was a mixture of dry and canned dog food and he was normally fed twice a day. He was not fed table scraps and did not scavenge. His appetite had decreased over the past 2 to 3 weeks, but had been good prior to that time.
His prior treatment included oral cimetidine and metoclopramide, which the owner thought may have slightly helped decrease the frequency of the vomiting or regurgitation.
Physical examination
The dog was bright and responsive. He had a body condition score (BCS) of 2/9. His mucous membranes were pink and his capillary refill time was less than 2 seconds. Thoracic auscultation revealed normal heart and lung sounds, with a heart rate of 90 beats per minute (bpm) and a respiratory rate of 36 breaths per minute. There was no evidence of pain on abdominal palpation.
Rectal temperature was 38.8° C.When the dog was observed eating, it was found that he could pre- hend the food, appeared to form a normal bolus and could initiate swallowing without a problem. This made a pharyngeal disorder less likely to be the cause of the regurgitation.
Clinical tip
Differentiating vomiting from regurgitation can be a challenge and in some cases both are occurring. The time after eating does not always provide a clue, as some animals may vomit immediately after eating and others, especially those with megaoesophagus, may regurgitate hours after eating (Table 2.1).
Table 2.1 Differentiating regurgitation from vomiting
| Clinical sign | Regurgitation/oeso- phageal disorders | Vomiting | |
| Abdominal effort | None | Present |
| Time of food ejection after eating | Immediate to delayed, possibly for hours | Delayed, possibly for hours, but may also happen immediately |
| Appearance of food | Undigested | Partly digested, may have bile present |
| pH of contents | Should not be acidic | Acid pH implies vomiting, but alkaline material may also be vomited |
Problem list and discussion of problems
• Vomiting
• Regurgitation
• Weight loss
The dog’s primary problem appeared to be regurgitation, although he also appeared to vomit occasionally as well. The weight loss was likely due to inadequate assimilation of food due to the regurgitating.
Differential diagnosis
For the regurgitation
• Oesophagitis
• Megaoesophagus, which can be idiopathic or due to an underlying cause
• Oesophageal obstructive disorders, e.g.
stricture, neoplasia, foreign body• Hiatal hernia
• Vascular ring anomalies - unlikely due to the dog’s age (usually present in puppies)
• Granulomas due to Spirocerca lupi: unlikely as this parasite is not endemic in the UK and he had not travelled out of the UK
• Oesophageal diverticula
For the vomiting
• Disorders of the stomach
• foreign body
• gastritis
• ulceration
• chronic partial dilation-volvulus
• neoplasia
• Disorders of the small intestine
• foreign body
• inflammatory bowel disease
• neoplasia
• parasites
• intussusception
• Disorders of the large intestine (unlikely as there were no signs consistent with colonic disorders)
• colitis
• obstipation
•Systemic disorders
• Pancreatopathy
• Hypoadrenocorticism
• Diabetes mellitus
• Liver disorders
• Peritonitis
• Renal disease/uraemia (unlikely)
•Dietary causes
• Adverse reaction to food (allergy or intolerance)
• Dietary indiscretion
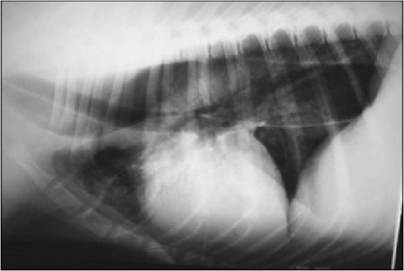
Case work-up [1] [2] sign (Fig 2.1). There was an increase in pulmonary opacity with an interstitial-alveolar pattern over the cardiac apex and cranial to the heart on the lateral radiograph, which was consistent with aspiration pneumonia. Fig 2.1 Radiograph of thorax showing dilated oesophagus (courtesy of Dr Tobias Schwarz). Diagnosis Megaoesophagus with aspiration pneumonia. Megaoesophagus can have an underlying cause or may be idiopathic; differential diagnoses for the more common underlying causes include: • Myasthenia gravis • Polymyopathy • Dysautonomia • Oesophageal obstructive disorders (foreign body, stricture, neoplasia, extra-oesophageal compression) • Lead toxicity • Hypoadrenocorticism • Hypothyroidism (possibly) Further testing This dog had no other signs consistent with a polymyopathy or dysauto- nomia. Further diagnostic tests included serum creatinine kinase and AST concentrations, which were within the reference range and also made a myopathy less likely. Physical examination, Schirmer tear test and pilocarpine response tests were also not consistent with dysautonomia. Clinical tip Pilocarpine response test In an animal suspected to have dysautonomia, if the pupils are affected, one drop of dilute pilocarpine ophthalmic solution (0.05%) should be placed in one eye and the diameter of the pupil observed every 15 minutes for 1 hour. Most normal dogs will not usually respond to this concentration and those that do show only minimal response at 60 minutes. Miosis of the treated eye demonstrates denervation supersensitivity as expected with dysautonomia. However, not all affected dogs will respond to the dilute pilocarpine, which could be a function of the time required for denervation supersensitivity to develop. The pilocarpine test is useful to rule out anticholinergic toxicity, which could cause many of the signs of dysautonomia. An anticholinergic drug would block the response of the pupil to pilocarpine (see Chapter 8). Blood lead concentration was within the normal reference range at 0.02 μmol∕l. Values greater than 1.21 μmol∕l indicate probable toxicity. An adrenocorticotrophin hormone stimulation test showed pre-stim- ulation serum cortisol of 89 mmol/l and a post-stimulation test of 321 mmol/l; which rules out atypical hypoadrenocorticism (i.e. hypoadrenocorticism where only the corticosteroid concentrations are insufficient and mineralocorticoid concentrations are sufficient to maintain normal serum potassium and sodium concentrations). The dog’s serum acetylcholine receptor antibody titre was 0.02 nmol/ l, which is considered normal. A value greater than 0.6 nmol/l is diagnostic of myasthenia gravis, although 15% of affected dogs may not show an increased titer. The dog’s total serum thyroxine concentration was just below the reference range at 12.9 nmol/l (reference range 13-52 nmol/l) and his TSH concentration was 0.13 ng/ml, with a reference range of less than 0.41 ng/ml. Endoscopy At endoscopy, the oesophagus was found to be very large, flaccid and contained fermenting food and fluid within the folds. There was evidence of mild oesophagitis at the distal aspect of the oesophagus. There was also evidence of gastritis and inflammation of the duodenum. Histopathology of the gastric and duodenal mucosa showed mild lymphocytic plasmacytic inflammation. Discussion The cause of this dog’s vomiting was likely the mild inflammatory condition of his stomach and small intestine. This was treated successfully with metronidazole at 10 mg/kg twice a day for a month and a change to a novel protein, highly digestible diet. The regurgitation was probably an unrelated condition. Reflux oesophagitis may cause regurgitation and even some dilation of the oesophagus, but not to the degree of dilation present in this dog. Underlying conditions were ruled out as far as possible, leaving the diagnosis as a probable idiopathic megaoesophagus. Treatment for idiopathic megaoesophagus Medical Treatment for idiopathic megaoesophagus is supportive and includes providing food and water from elevated containers to allow the aid of gravity for swallowing (Fig 2.2) and feeding a high calorie food. Some dogs cope better with liquid or soft food and some do better with ‘meatballs’ of dog food, so the diet has to be tailored for the individual. Fig 2.2 Example of feeding a dog from a height. Many promotility drugs have been tried unsuccessfully in an attempt to improve oesophageal motility in dogs with idiopathic megaoesophagus. Drugs such as anticholinergics that decrease the gastro-oesophageal sphincter tone could theoretically be beneficial; however, these have not shown any benefit and could be detrimental in dogs with inhalation pneumonia or reflux oesophagitis. Surgical Myotomy has been attempted for megaoesophagus, similar to the surgical approach for achalasia; however, dogs which had surgery had a worse outcome than those without surgery, so this is not recommended. Epidemiology Oesophageal dilation is a common cause of regurgitation and congenital idiopathic megaoesophagus is the most common form in the dog. Idiopathic megaoesophagus is inherited in the wirehaired fox terrier by simple autosomal recessive gene and in miniature schnauzers by simple autosomal dominant of a 60% penetrance autosomal recessive pattern. A breed predisposition exists in the German shepherd dog, Great Dane, Irish Setter and Chinese Shar Pei and it likely has a hereditable basis in these dogs also. Pathophysiology Idiopathic megaoesophagus is likely due to a lesion in the afferent limb of the swallowing reflex resulting in a loss of peristaltic function in the oesophageal body. Sensory stimulus from the presence of food or liquid in the oesophagus is necessary to stimulate the oesophageal phase of swallowing and it is this sensory reinforcement of the swallowing reflex that appears to be affected. Prognosis The prognosis for patients with idiopathic megaoesophagus is guarded, although some young patients recover with time. Once chronic dilation is present there may be irreversible damage to the oesophagus. Many of the dogs will eventually die from aspiration pneumonia or undergo euthanasia due to debilitation from chronic malnutrition.