1 Swallowing and regurgitation
The oesophagus and swallowing
The oesophagus is divided into the cervical, thoracic and abdominal parts.
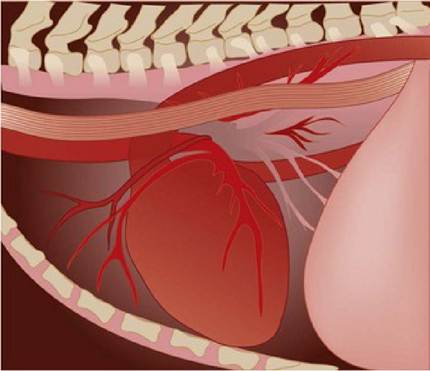
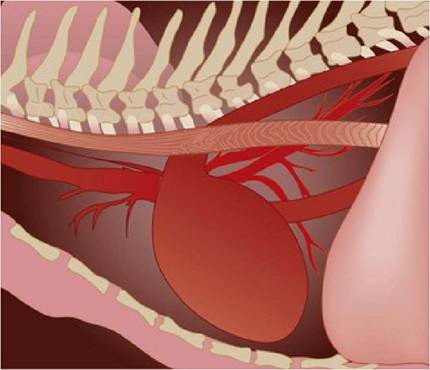
The cervical oesophagus runs ventral and to the left of the trachea, and thoracic oesophagus runs to the left of the trachea until the tracheal bifurcation, where it is dorsal to it, and then moves to the right of the aortic arch.
There is a short abdominal oesophageal segment between the diaphragm and the stomach. The oesophageal muscularis in the dog is striated throughout the oesophagus; whereas in the cat the caudal oesophagus (thoracic and abdominal sections) contains an increasing amount of smooth muscle until the final 2 to 3 cm which is entirely smooth muscle.The gastro-oesophageal sphincter (GES) is important in maintaining a high pressure zone between the oesophagus and the stomach so that gastric contents are less likely to be refluxed into the oesophagus. The type of food eaten affects the GES pressure. Protein meals increase the pressure, likely due to an increase in gastrin. Fat decreases GES pressure due to cholecystokinin stimulation and also inhibition of gastrin mediated pressure increases.
The GES relaxes transiently to allow for eructation of gas; during this relaxation fluid may also be refluxed into the oesophagus. This is a normal event, but in some dogs it may occur excessively or the rate of clearance of the acid from the oesophagus may be delayed, resulting in oesophagitis.
Swallowing involves three coordinated phases: oropharyngeal, oesophageal and gastro-oesophageal. Pharyngeal contact with food stimulates pharyngeal peristaltic contractions that push the food from the base of the tongue to the laryngopharynx and into the oesophagus. In the oesophagus, the bolus is initially carried by the primary peristaltic wave generated by the pharynx. If the primary peristaltic wave does not result in the bolus reaching the stomach, a secondary peristaltic wave is initiated by local oesophageal distension.
The swallowing reflex in the dog requires sensation of the bolus within the oesophagus. Oesophageal peristaltic speed is faster in the dog than in the cat; in dogs, water moves at 80 to 100 cm/second compared to 1 to 2 cm/second in the cat.Dysphagia
Dysphagia means difficulty in swallowing and may be due to either functional disorders or physical obstruction disorders. The disorders may be oral, pharyngeal or oesophageal.
Regurgitation
Regurgitation is expulsion of food or saliva from the pharynx or oesophagus and most often is caused by oesophageal disease.
Regurgitation must be differentiated from vomiting, although there are animals that present with both problems. Regurgitation is generally a passive action with no evidence of nausea. Some animals will retch due to the presence of food in the pharynx, which may be confused with an active action.
Regurgitated food is undigested and may be cylindrical in shape from having been formed in the oesophagus. The pH should not be acidic, although as gastric contents are not always acidic this may not be a useful way to distinguish between regurgitation and vomiting. Regurgitated material rarely contains bile, unless there has been gastro-oesophageal reflux prior to regurgitation. Regurgitation may occur immediately after eating or may occur several hours later, especially if the disorder is in the lower cervical or thoracic part of the oesophagus.
Dysphagia may occur in some animals with regurgitation and repeated swallowing attempts may be seen. Aspiration pneumonia is a serious risk in animals that are regurgitating and if present they may present with concurrent cough, respiratory distress or fever. Some animals with oesophageal disorders may also show nasal discharge due to ingesta entering through the nasopharyngeal opening.
In addition to aspiration pneumonia, common sequelae to chronic regurgitation are weight loss or poor growth as the animal is unable to assimilate sufficient nutrients.
Diagnosis of regurgitation
While oesophageal disorders may be suspected based on clinical signs, diagnosis usually requires radiological studies and endoscopy. Haematology and serum chemistry parameters are often not affected by regurgitation unless there is dehydration present due to insufficient fluid intake.
Radiography
The normal oesophagus is collapsed except during swallowing, so it not visualized on plain radiographs as it is of a similar density to the adjacent structures in the neck and mediastinum. The canine oesophagus has parallel longitudinal lines in the mucosa (Fig 1.1) whereas the caudal feline oesophagus has more oblique mucosal folds (Fig 1.2).
Fig 1.1
Fig 1.2
Normal canine oesophagus
Normal feline oesophagus
If air is seen in the oesophagus, it may be due to aerophagia, megaoesophagus, oesophagitis or an oesophageal obstruction. An increased radio-opacity in the oesophagus may be due to obstruction or food retention, or, less likely, oesophagitis.
Positive contrast studies utilizing fluoroscopy may be required to confirm oesophageal dysfunction and to evaluate oesophageal motility. Positive contrast studies are indicated when there is acute gagging, retching or acute or chronic regurgitation, dysphagia or known swallowing of a foreign body.
Clinical tips
Swallowing contrast studies
Ideally the patient should not be fed for 4 to 6 hours prior to the examination. If fluoroscopy is available, it should be performed prior to the administration of the contrast agent to ensure that the patient is in the correct position to clearly see the oesophagus. Plain radiographs are also usually taken at this time. It is recommended to use no sedation if possible, as sedation increases the risk of aspiration pneumonia and may affect oesophageal motility.
A small dose of acetylpromazine (0.01 mg/kg slow iv or im) may be useful in some cases and should not affect motility. Liquid barium may be administered slowly orally or mixed with food to assess swallowing of solids. Barium injected into marshmallows has also been suggested to assess intramural oesophageal disease that cannot be detected with a liquid swallow. (This is unlikely to be useful in cats.) Iodine-containing contrast solutions are recommended over barium if a perforation is possible as they cause less tissue reaction.Enlargement of the proximal oesophagus with normal function of the distal oesophagus suggests a vascular ring anomaly or oesophageal stricture. Other causes of megaoesophagus generally result in an enlargement of the entire oesophagus. Once a diagnosis of generalized megaoesophagus is confirmed, diagnostic testing should be performed to establish an underlying aetiology if possible.
A normal dog or cat restrained immediately in lateral recumbency after oral barium may retain some of it in the caudal cervical and cranial
thoracic areas of the oesophagus (Fig 1.3), but reverse peristalsis should not occur (i.e. food moving backwards up the oesophagus or from the stomach back into the oesophagus). The first phase of swallowing usually can be seen to move the bolus and barium into the oesophagus, with a second phase sometimes needed to move it all the way into the stomach. Linear streaking of the oesophagus with barium after swallowing is normal.

Fig 1.3
Normal oesophagram showing streaking of barium in the oesophagus
(courtesy of Dr Tobias Schwarz)
Endoscopy of the oesophagus can be used to rule out underlying causes of megaoesophagus such as oesophagitis, neoplasia and radiolucent foreign bodies although it can be difficult to assess the size of the oesophagus in an animal under anaesthesia. The normal feline oesophagus contains rings due to transverse oesophageal folds (Fig 1.4).
Fig 1.4

Endoscopic view of normal feline oesophagus
(courtesy of Prof Danielle Gunn-Moore)
Other tests should be done to look for underlying causes if generalized megaoesophagus is diagnosed. These tests could include: a complete blood count, biochemical panel, urinalysis, blood lead level, creatine kinase concentration, acetylcholine receptor antibody test (evaluation for myasthenia gravis) and evaluation of adrenal and thyroid gland function. Additional diagnostic procedures that may be performed based on the animal’s signalment, history and neurological examination, include an EMG study, nerve conduction velocities and muscle biopsies.
More on the topic 1 Swallowing and regurgitation:
- FEEDING AND SWALLOWING PROCESSES AND DISORDERS
- Persistent right aortic arch in a dog
- Table of Contents
- ESOPHAGEAL DISORDERS
- Urgent vs non-urgent gastrointestinal cases
- Oesophageal foreign body in a dog
- Dysphagia and Odynophagia
- GASTROESOPHAGEAL REFLUX DISEASE (GERD)
- Nutritional Management
- DISORDERS OF ORAL CAVITY
- 3 Myasthenia gravis in a dog
- Autoimmune Myasthenia Gravis
- Revolutionary Changes
- RHEUMATIC HEART DISEASE
- Mitral Stenosis
- 4 Oesophageal stricture in a cat
- THE KALA-KUTA POISON
- Acute Rejection, Heart
- 2 Idiopathic megaoesophagus in a dog
- Multiple choice questions