Persistent right aortic arch in a dog
Initial presentation
Regurgitating, especially food, since weaning
Signalment: 3-month-old uncastrated male Border collie, body weight 11 kg
Case history
The puppy had been obtained from a farm about a month prior to presentation.
Since then he had regurgitated frequently (several times a day), especially food but also occasionally water. The food he brought up was undigested with no bile present and the regurgitation occurred passively with no abdominal effort. Regurgitation usually occurred within minutes after eating, but recently it had occurred as long as an hour after meals. There was sometimes some retching after he regurgitated. He had no problem picking up his food and his initial swallowing appeared normal. He had been very bright, but was in poor body condition.His initial diet was a dry puppy food, free choice. The owners had tried adding water to the food, but this did not improve the clinical signs. When they first obtained him he had a good appetite, but during the week previous to admission he had been less interested in eating. The owners had been trying to tempt him to eat with a variety of foods. His faeces had usually been normal, although since the change in diet, they occasionally were soft.
Physical examination
The puppy was very bright and responsive, but not well grown. He was thin, with a body condition score of 2/9. His mucus membranes were pink and capillary refill time was less than 2 seconds. On oral examination his tonsils were slightly enlarged.
Thoracic auscultation revealed normal heart and lung sounds, with a heart rate of 140 beats per minute (bpm) and a respiratory rate of 24 breaths per minute. There was no evidence of pain on abdominal palpation and the only abnormality found was increased gas in the small intestines. Rectal temperature was 38.6° C.
Problem list and differential diagnoses
Regurgitation was the puppy’s primary problem.
Differential diagnoses for regurgitation for this puppy included:• Megaoesophagus
• Oesophageal stricture
• Oesophagitis
• Vascular ring anomaly (e.g. persistent right aortic arch (PRAA))
• Hiatal hernia
• Oesophageal dysmotility.
An oesophageal foreign body was unlikely (but not impossible) because of the duration of the clinical signs. Immune-mediated disorders (e.g. myasthenia gravis) and tumours were also unlikely in this young dog as they generally occur later in life.
Diagnostic aids
Diagnostic techniques that were indicated in this puppy included plain thoracic radiographs, which help diagnose megaoesophagus and foreign body. A positive contrast study using barium mixed with dog food would also help localize and characterize oesophageal disorders such as strictures, PRAA and dysmotility. Oesophageal endoscopy would also be useful to visualize the mucosa of the oesophagus.
Case work-up
Minimum data base
The dog was admitted to the hospital and a minimum data base including haematology, serum chemistry and routine urinalysis was performed. The results from these tests were unremarkable.
Imaging
Plain films indicated the possibility of a megaoesophagus in the cranial thoracic area. A positive contrast study with a barium meal revealed oesophageal constriction at the base of the heart and marked oesophageal dilatation extending cranially from that constricted area (Figs 7.1 and 7.2).

Figs 7.1

Figs 7.1 and 7.2
Lateral and ventrodorsal thoracic radiographs with contrast, showing enlarged oesophagus up to the level of the heart
(courtesy of Dr Geoff Culshaw)
Endoscopy
Oesophageal endoscopy showed a pinched area of the oesophagus and also inflammation of the oesophageal mucosa.
Diagnosis
A diagnosis of vascular ring anomaly and oesophagitis was made.
Treatment - surgical
The treatment consisted of transecting the bands forming the vascular ring. In this case a left thoracotomy was performed and a persistent right Iigamentum arteriosum was identified, dissected and divided. A thoracostomy tube was placed for immediate post-operative management.
Treatment - medical
Treatment for the oesophagitis included omeprazole (1 mg/kg po q 24 hours) and sucralfate suspension (1.5 ml po q 8 hours given 1 hour before feeding or other medications).
Clinical tip on sucralfate
Sucralfate binds to ulcerated mucosa forming a protective covering and stimulates repair mechanisms partially via stimulation of prostaglandin-mediated pathways. It has few side effects (constipation is reported in people but rarely seen in cats or dogs), but it can potentially affect the bioavailability of other medications and should probably be given separately. It may work best in the acid environment of the stomach, but does also work in a neutral pH and is therefore also indicated for use in oesophageal erosions or ulcers.
Nursing care
A liquid food was fed to try to ensure that adequate nutrition was maintained. The puppy’s caloric requirements were determined and food provided in four meals per day. The initial amount of food on the first day provided one-third of his energy requirements and was increased to full feeding by day 3. The meals were provided from a height as with other megaoesophagus patients. Another option for nutritional support would have been placement of a gastrostomy tube.
Clinical tips on nutrition in puppies
Puppies need more calories per kilogram of body weight than do adult dogs or around 2.5 to 3 times resting energy requirements (RER). They also have higher protein requirements of 22 to 32% of dry matter and increased calcium requirements of 0.7 to 1.7% dry matter; these concentrations would be provided in a good puppy food.
For this 11 kg underweight puppy, initial RER was estimated to be 70 ? body weight (kg)0∙[75] or 70 ? 110∙75 = 443 kcal.
At 3 months of age he needs three times RER or about 1330 kcal. His initial feeding should be for his existing body weight, with increased amounts over time to increase his body condition score.A typical puppy food contains around 3.8 kcal/g, so this puppy would need about 350 g of food per day.
Follow-up
The puppy was seen again 2 weeks after the surgery. He was still regurgitating, but it had decreased to once or twice per week. The puppy was still very bright and his body condition had improved to 3/9 and he had gained 2 kg. The owner was still feeding gruel.
Discussion and epidemiology
All patients with regurgitation are at risk for aspiration pneumonia and should be monitored for signs consistent with it. Poor body condition is consistent with inadequate food intake in many patients with oesophageal disorders.
The most common vascular ring anomaly is the persistent right aortic arch (PRAA). In normal embryonic development, the aortic arch develops from the left fourth aortic arch and left dorsal aortic root and the adult aortic arch is to the left of the oesophagus. There are other variations of abnormal development, for example retention of both arches or origination of the left subclavian artery from the right aortic arch. When the vessels develop abnormally, they may constrict the oesophagus (Fig 7.3).
Fig 7.3
Oesophagus
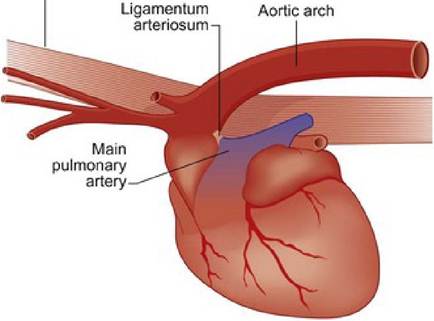
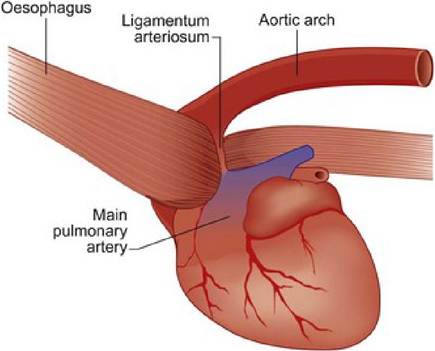
The normal heart and a heart with persistent right aortic arch
The presence of oesophagitis in this case may have been due to the prolonged presence of food material irritating the oesophagus.
It is likely that vascular ring anomalies have an inherited basis, as there are breed predispositions in German shepherd dogs, Great Danes, Irish Setters, Boston terriers and greyhounds. The disorders are much less common in cats, but have been reported.
Prognosis
It is estimated that only 10% of affected dogs will develop completely normal oesophageal function after surgery and up to 50% of affected dogs will continue to show occasional signs of regurgitation. Permanent oesophageal dilation cranial to the constriction is common due to irreversible degenerative changes. As many as 40% of these cases have been reported to have a short survival time due to malnourishment and/or aspiration pneumonia. This puppy’s initial improvement in signs and body condition was encouraging, although he was still at risk for aspiration pneumonia.