RHEUMATIC HEART DISEASE
Rheumatic heart disease (RHD) is the commonest sequel of RF, due to residual thickening, scarring and deformity of valvular anatomy after acute valvulitis in RF. Recurrent attacks increase the risk and severity of valvular damage.
Recent data suggests ~ 0.5-1.0% of Indian school children have evidence of rheumatic heart disease.Common organic valvular lesions in RHD are leftsided, i.e. MR, MS and AR in order of frequency, either alone or in combinations. Rheumatic AS is extremely rare before 20 years of age. Right-sided lesions are usually functional and regurgitant, due to back-pressure from left-sided lesions, though TR may be organic. Pulmonary valve is almost always spared in RF.
Mitral Regurgitation (MR)
Mitral regurgitation is the commonest valvular lesion in acute carditis as well as in established RHD (gt;90%), characterized by reverse leak from LV to LA during ventricular systole due to deformed and incompetently closed MV. Severity of MR is maximum during acute carditis and tends to diminish gradually, may even disappear in gt;50% cases by 1 year of acute attack.
Hemodynamics and consequent genesis of clinical signs in MR includes:
• Incompetent closure of MV leading to muffed S1.
• Regurgitation of LV blood in LA during ventricular systole due to defective MV closure, producing high pitched apical pansystolic murmur that radiates towards the axilla, with/without thrill.
• Dilatation of LA to accommodate regurgitant flow. However, as there is no obstruction to LA outflow, mean LA pressure does not rise significantly. Consequently, pulmonary venous hypertension and CCF due to back-pressure is uncommon (unlike MS) except in cases with associated severe MR or acute carditis, when LA could not dilate enough due to rapidity of lesion.
• Volume-overload over LV, as it: (a) receives more blood from LA during next cycle, and (b) has to contract more forcefully to maintain cardiac output, leading to LVH, i.e.
downward and outward shifting of apex beat with heaving character.• Increased LA gt; LV flow through MV in diastole due to additional LA volume, may produce III heart sound and/or a short diastolic flow murmur (functional) at apex in severe MR. Hence, presence of an apical middiastolic murmur in MR does not necessarily mean coexisting MS.
• LV pressure drops rapidly during systole due to MV leak, leading to mild water-hammer pulse and split S2 by early closure of AV in severe cases. Hence, widely split S2 in MR does not necessarily mean PH.
Clinical presentation: Unlike MS, MR is an early lesion in RHD, often in continuation of acute carditis (no latent period). While mild cases may be asymptomatic, moderate/severe cases present with signs of reduced cardiac output (exertional dyspnoea, easy fatigability) or compensatory cardiac overactivity, e.g. tachycardia/ atrial arrhythmia (palpitation).
CCF and PH is rare in MR and indicates possibility of acute carditis, severe lesion or co-existing MS.
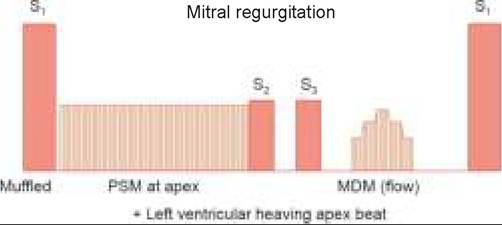
Important cardiac signs include—(a) LV heaving apex beat, shifted downward and laterally, (b) muffled FHS,
(c) apical PSM radiating to axilla, with/without (d) apical flow MDM, and (e) audible S3 (Fig. 17.20).
Complications include: (a) CCF/PH in severe disease,
(b) atrial arrhythmias, (c) infective endocarditis, and (d) development of supervening MS.
Diagnosis is supported by:
• X-ray chest suggestive of LVH,
• ECG suggestive of LVH and
Echocardiography suggestive of—(a) increased LV and LA dimensions, (b) hyperdynamic motion of septum,
(c) thickening/calcification of anterior MV leaflet, and
(d) regurgitant flow on pulse/color Doppler studies.
D/D includes other cause of MR (Table 17.26), commonest being mitral valve prolapse, discussed later.
Treatment depends on the severity of disease and include—(a) rheumatic and infective endocarditis prophylaxis, (b) treatment of complications, e.g. CCF, infective endocarditis or arrhythmia, and (c) afterload reducing agents, e.g.
captopril, in selected cases to improve cardiac output and consequently, to reduce the regurgitant flow through MV.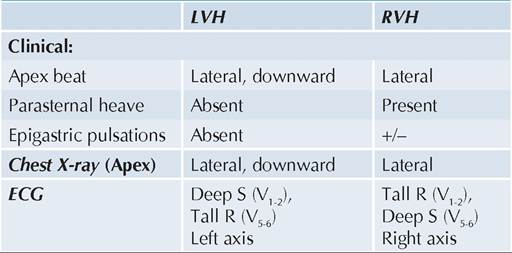
Fig. 17.20: Important cardiac signs in MR.
PSM: Pansystolic murmur; MDM: Mid-diastolic murmur
TABLE 17.26: Causes of MR
• Rheumatic MR
• Congenital
- Mitral valve prolapse (MVP)
- MR with/without osteum primum ASD.
- Collagen defects: Marfan syndrome, Hurler syndrome
• Acquired (due to LV dilatation)
- Cardiomyopathies, myocarditis, etc.
- Infective endocarditis, papillary muscle dysfunction
- Functional MR in AR (due to LV dilatation)
Surgical correction with valve repair (annuloplasty) or valve replacement is indicated in cases with—(a) refractory CCF, (b) progressive LV dilatation on ECHO, (c) severe pulmonary hypertension and (d) complications, e.g. ruptured chordae or recurrent infective endocarditis. Annuloplasty is preferred in children to avoid longterm anticoagulant therapy, essential after replacement surgery.
Mitral valve prolapse (MVP) is a common congenital abnormality, echocardiographically detectable in ~15-20% of population. It is characterized by billowing of one or both cusps into LA during ventricular systole.
MVP is more common in females and those with similar family history, Marfan syndrome, pectus excavatum, etc.
Clinically, most cases are asymptomatic and diagnosed accidentally due to presence of a typical musical late systolic murmur, sometimes preceded by a click.
MVP is non-progressive and no treatment is necessary in childhood after initial evaluation. Rarely, complications, e.g. arrhythmias, strokes, infective endocarditis and CCF may develop in later life.
Mitral Stenosis (MS)
MS is a late lesion in RHD due to fibrosis of valvular ring, commissural adhesions and thickening or calcification of valvular leaflets, restricting their mobility. Although develops much earlier in Indian than in western children, it takes at least ~2 years to develop established MS after an acute attack of RF.
MS accounts for ~10% of all pediatric RHDs, either alone or in combination with MR or other valvular lesions.Hemodynamics and consequent genesis of clinical signs in MS includes:
• Turbulence in LAgt;LV flow due to narrowed MV (Normal size: ~5 cm2), producing localized mid-diastolic murmur with presystolic accentuation at apex, best heard in expiration and left lateral position with bell of the stethoscope. MDM may disappear during CCF.
• Delayed but forceful closure of MV, leading to pathognomonic loud S1. Absence of loud S1 indicates very tight or calcified MS.
• LA dilatation (volume-overload) due to obstructed outflow with consequent increase in LA pressure. LA volume-overload necessitates early and forceful opening of MV during diastole, presenting as opening snap (OS) just after S2, which may be absent in tight or calcified MS.
• Rise in pulmonary venous pressure due to back pressure from LA, leading to pulmonary venous hypertension (PVH) and consequent pulmonary congestion/edema, which presents as progressive dyspnea, cough, frothy or rusty sputum and basal crepitations in lungs.
• Rise in pulmonary arterial pressure, first slowly and passively due to PVH and then rapidly and actively by pulmonary arteriolar constriction to maintain adequate PA-PV pressure gradient, leading to pulmonary arterial hypertension (PAH). PAH presents with—(a) loud P2 that may also be palpable (diastolic shock), (ii) wide-split S2 due to delayed PV closure, and (iii) early diastolic murmur at lower sternal border (Graham-Steel murmur) due to functional PR.
• Rise in RV pressure due to PAH with consequent RVH, presenting as left parasternal heave, tricuspid pansystolic murmur (functional TR) and CCF. RVH also lead to typical tapping apex beat in MS, as the posterior RV pushes the LV forward.
Clinical presentation depends on the severity of MS and includes signs of:
• Chronic pulmonary congestion, e.g.
progressive dyspnea, orthopnea, paroxysmal nocturnal dyspnea and recurrent chest infections, orthopnea and nocturnal dyspnea are early features in MS, due to pooling of blood in the lungs in lying-down position.• Acute pulmonary edema, e.g. cough, frothy and rusty (blood-tinged) sputum and respiratory distress.
• CCF, e.g. pedal edema, hepatomegaly, raised JVP, etc.
• Systemic venous stasis, e.g. malar flush (Mitral facies)
• Reduced cardiac output, e.g. easy fatigability, syncopal attacks, etc.
Important clinical signs in MS include-(a) loud first HS, opening snap, (b) mid-diastolic murmur with late accentuation and (c) loud second HS after development of pulmonary hypertension (Fig. 17.21).
Severity of MS may be judged by-(a) absence of S1 or opening snap due to calcified valve, (b) lesser time distance between opening snap and aortic component of S2, and (c) severe PAH.
Complications of MS include—(a) pulmonary edema, (b) CCF, (c) infective endocarditis, (d) arrhythmia, and
(e) thromboembolic complications due to LA hemostasis and thrombus formation.
Diagnosis is supported by:
• X-ray chest suggestive of—(a) RVH, i.e. outward shifting of apex beat, (b) straightening of left cardiac
St MiLnSl i#8539;#8719;#8739;5#8539;rt S#8739;
-i- KL,#8729;,err#8739;#953;cua#953; lapping aptx onl
Fig. 17.21: Important cardiac signs in MS.
OS: Opening snap; MDM: Mid-diastric murmur
border due to enlarged LA appendages (mitralization), and (c) pulmonary venous congestion (Kerley B lines) or pulmonary edema (diffuse haziness).
• ECG suggestive of—(a) RVH with Rt axis deviation, and (b) P mitrale-wide-notched P wave of LA dilatation.
• Echocardiography suggestive of—(a) decreased MV leaflet movements (E-F and D-E slope) on M-mode, (b) LA dilatation with decreased MV size on 2-D echo, and (c) increased transmitral pressure gradient on Doppler studies.
Echocardiography also help to assess severity of PAH and exclude complications, e.g. infective endocarditis and LA thrombus.D/D includes other rare causes of MS, e.g. congenital MS, endomyocardial fibroelastosis and Lutembacher syndrome (acquired MS with ASD) or conditions mimicking MS hemodynamics, e.g. LA myxoma, ball-valve LA thrombus or Cor triatriatum.
Treatment includes—(a) restricted physical activity,
(b) rheumatic and infective endocarditis prophylaxis,
(c) treatment of complications, e.g. CCF, infective endocarditis or arrhythmia, and (d) surgery.
Surgical intervention in MS depends on the type of lesion, as follows:
• Transcutaneous balloon valvuloplasty is the treatment of choice for non-calcified valves, as early as possible before significant PAH develops. Due to lesser risk, cost and duration of hospitalization, it has nearly replaced the need for closed mitral commissurotomy, practiced earlier.
• Open valvotomy or valve replacement is indicated in children with—(a) calcified MV, (b) critical MS with MV size lt;1 cm2, (c) co-existing MR, and (d) complications, e.g. LA thrombus.
Aortic Regurgitation (AR)
AR is rarely an isolated rheumatic lesion, usually seen along with MV disease in ~5-8% RHDs. It is characterized by reverse leak from aorta to LV during ventricular diastole through incompetent AV.
Hemodynamics and consequent genesis of clinical signs in AR include:
• Backward leak from aorta to LV during ventricular diastole, leading to high-pitched blowing early diastolic (decrescendo) murmur.
• LV volume-overload due to reverse aortic-flow, leading to LVH with outward and downward shift of apex beat that is hyperdynamic (ill-sustained heave) in character. Anginal chest pains are common in severe AR due to relative ischemia of hypertrophic myocardium.
• Dilated AV ring and regurgitant aortic flow may prevent MV to open fully, leading to a functional apical diastolic murmur (Austin-flint murmur).
TABLE 17.27: Peripheral signs in AR
• Wide pulse pressure gt;40 mm Hg
• Collapsing (water-hammer) pulse
• Corrigan's sign (dancing carotids)
• de Musset's sign (head-nodding during systole)
• Quincke's sign (Tcapillary pulsations on nail bed)
• Traube sign (pistol-shot sound over femoral artery)
• Duroziez murmur (murmurs over femoral artery)*
• Hill's sign (lower limb BP gt;20 mm higher than in UL) *Diastolic murmur on pressing the femoral artery distal to stethoscope and systolic murmur on pressing proximally.
• Increased LV outflow due to volume overload, may lead to—(a) functional ejection systolic murmur at aortic area, and (b) delayed AV closure with narrow split of S2.
• A combination of increased LV outflow, followed by immediate reverse leakage from aorta (aortic runoff) is responsible for sudden drop in aortic pressure during ventricular diastole, leading to wide pulse pressure and other peripheral signs (Table 17.27).
• Absence of wide pulse pressure or water-hammer pulse in AR indicates co-existing MS or AS.
• Pulmonary hypertension is uncommon except in severe AR, caused by back-pressure (LV gt; LA gt; PVH gt; PAH).
Clinically, mild cases may be asymptomatic, though severe cases present with palpitations (due to forceful LV contractions) and progressive exertional dyspnea. Anginal chest pain may be precipitated by exercise. Excessive sweating and heat intolerance is common due to peripheral vasodilatation.
On examination, collapsing pulse with wide pulse pressure along with other peripheral signs of aortic runoff (Table 17.27) are useful indicator of AR.
Important cardiac signs include—(a) LV heaving apex impulse, and (b) high pitched decrescendo ejection diastolic murmur over pulmonary area that radiates towards apex and aortic area and best audible in full expiration with patient leaning forward, (c) a functional diastolic murmur at apex (Austin Flint murmur) and/or ejection systolic murmur at aortic area may be present (Fig. 17.22).
Diagnosis is confirmed by:
• X-ray chest suggestive of LVH and prominent aortic knuckle due to higher LV outflow gt; aortic dilatation.
• ECG suggestive of LVH.
• Echocardiography suggestive of—(a) dilated LV on M-mode, (b) diastolic flutter of anterior MV cusp due to regurgitant aortic flow on 2-D echo, (c) abnormal LV-aorta pressure gradient with aortic run-off on Doppler studies.
D/D of AR includes:
• Other causes of wide-pulse pressure, e.g. PDA, large AV fistulae, ruptured sinus of valsalva, severe anemia, thyrotoxicosis, etc.
• Other causes of AR, e.g. congenital AR, bicuspid AV, Marfan syndrome, aortic aneurysms, etc.
Management: Mild/moderate lesions are well tolerated though unlike MR, AR does not regress with time. Treatment includes: (a) rheumatic and infective endocarditis prophylaxis, (b) treatment of complications, e.g. CCF, infective endocarditis and arrhythmia and (c) surgery.
Surgery with valve replacement is indicated in - (a) progressive LV enlargement or deteriorating LV ejection fraction (lt;40%), (b) development of CCF and angina.
Tricuspid Regurgitation (TR)
Although TR is present in 20-30% cases of RHD with CCF, it is rarely organic, usually caused by RV dilatation in severe left-sided lesions. Hence, the signs of TR are generally evident only during CCF due to primary RHD and disappear once it is controlled.
Important clinical signs of TR include - (a) prominent jugular venous pulsations, (b) pulsatile liver, (c) blowing pansystolic murmur over tricuspid area, best audible in inspiration; along with features of primary RHD. Valvuloplasty is rarely needed in these cases.
Diagnostic Approach to RHD
Diagnostic approach in a suspected case of RHD aims to: • Identify the valvular lesion/s on the basis of clinical and investigational criteria (Table 17.28).
TABLE 17.28: Common differentiating signs in various valvular lesions in RHD
• Exclude congenital lesions on the basis of age, past history of RF, absence of other congenital anomalies and other features (Table 17.22).
• Exclude active RF and clinical carditis (Table 17.24) or sub-clinical carditis on the basis of echocardiography.
• Exclude or confirm the presence of complications CCF, infective endocarditis and arrhythmia on the basis of features discussed in respective chapters.
• Assess the severity of valvular defect and presence/ severity of PAH to decide the need and time of surgery, as discussed earlier.
17.8
More on the topic RHEUMATIC HEART DISEASE:
- Preconceptional evaluation of women with heart disease
- Heart Failure
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- Mitral Stenosis
- Chapter 22 Cardiovascular and Respiratory Disorders
- 1 Swallowing and regurgitation
- Peripheral Vascular Disease
- Tanzania
- Deceit and Coercion