3 Myasthenia gravis in a dog
Initial presentation
Regurgitation, cough and weakness/exercise intolerance
Signalment: 2-year-old neutered male collie crossbred dog, body weight
19.8 kg
Case history
The dog had become progressively less exercise tolerant over the 2 months prior to presentation.
He had also initially begun to regurgitate his food and then began to regurgitate water. The regurgitation usually occurred within a few minutes after eating, but occasionally he brought up foam without having eaten anything. The food that he regurgitated was formed and undigested. He was still interested in eating and the owners had started feeding him very small amounts, as any larger amounts were regurgitated.He had become progressively less able to go for walks and would sit or lie down after several minutes of walking. He remained conscious during these times and he would usually be willing to walk again after a short rest. He had begun to cough during the previous week and his breathing was laboured. His faeces were formed and were passed normally and his urination was normal.
The dog had been in the owners’ possession about a year and was current on vaccinations and de-worming.
Physical examination
The dog was quiet but responsive and preferred to lie on the consulting room floor during the examination. He was reluctant to walk when taken outside and his gait was abnormal (Fig 3.1). His body condition score was 4/9. Mucus membranes were pink and capillary refill time was less than 2 seconds. Pulse quality was good.

Fig 3.1
Dog with myasthenia gravis showing weakness and abnormal stance
Thoracic auscultation revealed normal heart sounds but crackles over the left lung fields. Heart rate was 140 beats per minute (bpm) and the respiratory rate was 60 breaths per minute with some inspiratory effort.
There were no abnormalities detected and no evidence of pain on abdominal palpation. His rectal temperature was 39.1° C.
Problem list and discussion of problems
• Regurgitation
• Weakness and exercise intolerance • Cough
Regurgitation in this dog may have been due to:
• Megaoesophagus
• Oesophageal stricture
• Oesophagitis
• Oesophageal dysmotility
• Hiatal hernia
• An oesophageal foreign body was less likely because of the duration of the problem.
Weakness and exercise intolerance can by caused by many systemic disorders, including (but not limited to) cardiopulmonary diseases, metabolic disorders such as hypothyroidism or hypoadrenocorticism, neurological disorders such as polyneuropathies or myasthenia gravis, myopathies or pain due to other disorders.
Coughing can be due to upper respiratory disorders, lower respiratory disorders or cardiac disorders. As this dog had crackles on auscultation, a lower respiratory (lung) disorder was suspected. Crackles are discontinuous, non-musical sounds produced when airway pressures fluctuate or when air rushes through fluid- or mucus-filled alveoli, but can sometimes also be heard when there is fluid in the oesophagus.
Case work-up
Minimum data base
Haematology, serum chemistry and routine urinalysis were performed. The haematology results showed an increase in neutrophils with a slight left shift, consistent with the presence of inflammation. The serum chemistry results were unremarkable, as was the urinalysis. Basal serum cortisol was 132 nmol/l (reference range 20-230 nmol/l).
Clinical tip on use of basal serum cortisol
A serum basal cortisol concentration of 70 nmol/l or greater effectively rules out hypoadrenocorticism. If the value is less than 70 nmol/l, an ACTH stimulation test should be performed to definitively rule out or diagnose this disorder.
Imaging
Clinical tip on imaging in regurgitating cases
Plain thoracic radiographs help rule out megaoesophagus and screen for cardiopulmonary disorders.
A positive contrast study using barium mixed with dog food using fluoroscopy helps determine if there are oesophageal motility disorders or a hiatal hernia, but in cases like this dog, which have a cough, the risk of furthering an aspiration pneumonia is present.Thoracic radiographs showed the presence of a large oesophagus and a bronchial alveolar pattern especially affecting the left cranioventral lung lobes, consistent with aspiration pneumonia (Figs 3.2 and 3.3).
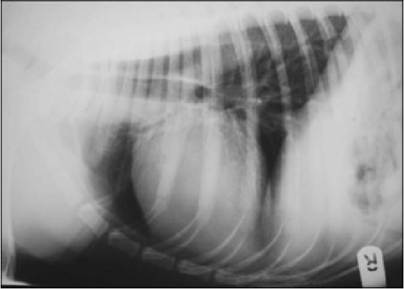
Figs 3.2

Figs 3.2 and 3.3
Lateral and ventrodorsal thoracic radiographs showing
enlarged oesophagus
(courtesy of Dr Tobias Schwarz)
Neurological examination
A neurological examination was largely unremarkable, although after walking for a couple of minutes the dog developed a stiff, choppy and hunched gait. He then lay down and developed tremors of the hind legs and was unable to rise for a short period. Once given time to recover, the dog could walk and then this pattern would reoccur. As this is typical of dogs with myasthenia gravis, an edrophonium response test was performed.
The response to this test was dramatic, in that the dog immediately stood up and was willing to trot down the corridor. This response is consistent with a presumptive diagnosis of myasthenia gravis.
Clinical tip on tensilon test
The edrophonium chloride (Tensilon) response test is used to diagnose myasthenia gravis. The dog or cat is exercised (if necessary) until they sit or lie down or the gait becomes abnormal. A dose of 0.1 to 0.2 mg/kg of edrophonium chloride is administered intravenously. A positive test results in temporary improvement of locomotor signs within minutes. Oesophageal musculature does not improve with edrophonium. There are false positive and false negatives with this test, as well as equivocal results, so it should be used as an adjunct test and not for definitive diagnosis.
The primary criterion for diagnosis of myasthenia gravis is the presence of serum antibodies that react with alpha-bungarotoxin extracted ACh receptors; this test is highly specific, although about 15% of suspected myasthenics are seronegative (see Appendix 6).
Nursing aspects
As with other cases of megaoesophagus, this dog was fed frequent small meals from a height. Different patients do better on different types of food and this dog regurgitated less when fed meatballs of canned food. Water was also offered from a height.
For the aspiration pneumonia, in addition to antibiotic treatment (below), nebulization and coupage were carried out four times a day to help relieve pulmonary congestion.
Medical treatment
Pyridostigmine at 15 mg po q 8 hours was started. Some dogs with severe megaoesophagus are unable to take oral medications and treatment needs to initially be with injectable neostigmine (0.04 mg/kg im q 6 hours); however, this dog managed with the medication hidden in his dogfood meatballs.
Treatment for the aspiration pneumonia included antibiotic therapy with marbofloxacin (2 mg/kg po q 24 hours), clavulanate potentiated amoxicillin (15 mg/kg po q 12 hours) and clindamycin (7.5 mg/kg po q 12 hours). Antibiotic cover for aspiration pneumonia usually involves the use of multiple antibiotics to provide ‘four quadrant’ bacterial cover (i.e. Gram-negative and Gram-positive, aerobic and anaerobic bacteria).
Follow-up
A serum acetylcholine (ACh) receptor antibody test was submitted and these results came back with a high value of 2.8 nmol/l, confirming the diagnosis of myasthenia gravis. A value of greater than 0.6 nmol/l is consistent with myasthenia gravis.
The dog was seen 2 weeks later, when his gait was nearly normal and the cough was no longer present. He still occasionally had regurgitating episodes, but the frequency was decreased.
Discussion and epidemiology
Acquired canine myasthenia gravis is an autoimmune disease in which autoantibodies are directed against muscle postsynaptic nicotinic acetylcholine receptors (Fig 3.4).
In some cases there is a concurrent thymoma which is the stimulus for the antibody production; this is more common in cats than in dogs.Fig 3.4
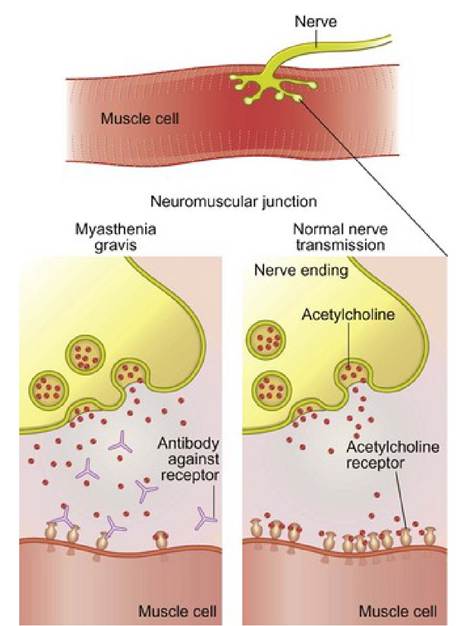
Anti-cholinesterase receptor and effects of antibodies against the receptor
Acquired myasthenia gravis is probably the most common neuromuscular disorder diagnosed in the dog. Studies have identified a high relative risk for acquired myasthenia gravis in the Akita, Scottish terrier, German shorthaired pointer and Chihuahua breeds of dogs and in Abyssinian and Somali cats. Familial myasthenia gravis has also been identified in Newfoundlands and Great Danes.
The typical signs include muscle weakness which can be generalized as in this case, focal, for example affecting only the oesophagus or the facial, pharyngeal or laryngeal areas, or can be acute, fulminant, and generalized which results in a very rapid onset of tetraparesis and dyspnoea. About 90% of the dogs with the generalized form have megaoesophagus. Acquired canine myasthenia gravis has a high mortality rate (approximately 50%) and according to one specialist in the field, this is due in part to a misdiagnosis of vomiting when actually the dog is regurgitating due to oesophageal dilatation. This delayed recognition of regurgitation usually involves inappropriate therapy with an increased risk of developing an aspiration pneumonia which in itself may be life threatening.
Treatment with anti-cholinesterase drugs like pyridostigmine prolongs the interaction of ACh with the receptors. The dose should begin low and be increased to effect. Oesophageal motility is minimally affected by this treatment. Some studies recommend using prednisolone, although this should not be initiated concurrently with anti-cholinesterase medications as it can exacerbate the weakness and should not be used in the presence of pneumonia. Low-dose alternate day oral prednisone therapy (0.5 mg/kg every other day) is suggested when anti-cholinesterase drugs are not effective.
Myasthenic female dogs and cats should be spayed as soon as possible after the signs of myasthenia gravis are under control as heat cycles and pregnancy can exacerbate the disorder. Vaccinations may exacerbate the clinical signs. It is generally best to avoid the use of drugs that may affect neuromuscular transmission such as ampicillin, aminoglycosides, anti-arrhythmic agents, phenothiazines, anaesthetics, narcotics and muscle relaxants. Also, organophosphate dips may result in a cholinergic crisis since they could be additive with pyridostigmine.
Prognosis
Many patients with myasthenia gravis have spontaneous remissions within a year of being diagnosed, although overall the prognosis is guarded as about 50% die or undergo euthanasia. Those that die usually
have succumbed to aspiration pneumonia. In this case the initial response was good and the early prognosis was cautiously optimistic (Fig 3.5).

Fig 3.5
Dog with myasthenia gravis after treatment showing improvement in strength
More on the topic 3 Myasthenia gravis in a dog:
- 1 Swallowing and regurgitation
- 14 Hypoadrenocorticism in a dog
- Haemorrhagic gastroenteritis in a dog