Pulmonary Neoplasia
Primary pulmonary adenomas and adenocarcinomas are among the most common tumors found in mice. A strain mice are highly susceptible, with tumors arising by 3-4 months of age and reaching 100% prevalence by 18-24 months.
Pulmonary tumors are also common in somewhat less susceptible strains, such as outbred Swiss, FVB, BALB/c, 129, and B6;129 hybrids. The uniquely high susceptibility of A strain mice is related to their K-ras allele, with activation of K-ras in the tumors. The onset and prevalence of pulmonary tumors can be enhanced with viral infections, such as Sendai virus, or chemical carcinogens. Most spontaneous pulmonary tumors are believed to originate from type II pneumo- cytes or a common precursor cell for type II and Clara cells. Most GEM models for pulmonary neoplasia develop pulmonary tumors that resemble spontaneous or chemically induced tumors. The recent MMHCC consensus classification has attempted to align mouse pulmonary tumors with those that arise in humans. For this reason, the terms "bronchioloalveolar” or "alveolar/ bronchiolar” that have been used for mouse tumors in the past have been dropped. Spontaneous or carcinogen- induced tumors are now simply diagnosed as pulmonary adenomas or carcinomas with appropriate qualifications (solid, papillary, or mixed). Other types of tumors are included in the new classification, such as papilloma, squamous cell carcinoma, adenosquamous carcinoma, neuroendocrine carcinoma, and others, but these are rarely encountered as spontaneous tumors in the mouse.Pulmonary tumors are often encountered as incidental findings, but those that grow expansively can result in clinical signs of dyspnea. They appear as circumscribed, firm to resilient, pearl-gray nodules located in the sub- pleural regions or deep within the parenchyma of the lung. Tumors may be large, with bulging contours (Fig.
1.130). There may be evidence of pleural invasion, with seeding of the visceral and parietal pleura. On microscopic examination, adenomas display compression of
FIG. 1.130. Pulmonary adenoma in an aged laboratory mouse. There is a large, raised, circumscribed mass in the cranial region of the right lung.
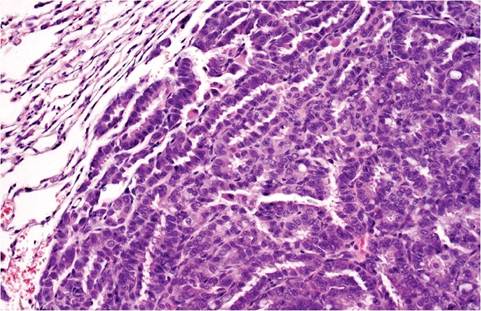
FIG. 1.131. Pulmonary adenoma. Cuboidal epithelial cells are lining alveolar septa. There is a distinct line of demarcation between the tumor and the adjacent compressed normal lung tissue.
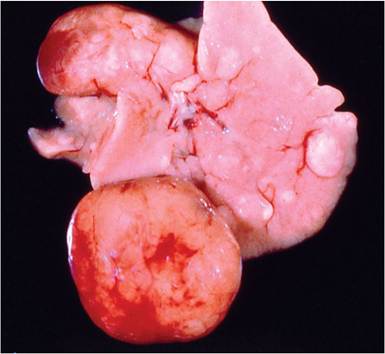
FIG. 1.132. Hepatocellular tumors in a DBA mouse. Note the multicentric nodules of varying size.
the adjacent structures (Fig. 1.131). They are composed of closely packed cuboidal to columnar cells lining remnants of alveolar septa, with a sparse stroma of collagenous tissue. Tumor cells are relatively uniform in size, with round, hyperchromatic nuclei and acidophilic cytoplasm. Cells are nonciliated, and mitotic figures are rare. Those that are adjacent or protruding into bronchioles may consist of tubular to papillary patterns composed of columnar epithelial cells with convoluted to folded basal nuclei. There is compression of the adjacent alveolar structures. Pulmonary carcinomas tend to invade the adjacent parenchyma, including the pleura; frequently form papillary structures; and consist of large, pleomorphic epithelial cells with irregular, polygonal, hyperchro- matic nuclei. There may be extensive invasion of the adjacent pleural surface and occasionally extension into the intercostal muscles. Occasionally, pulmonary tumors are encountered with mucinous differentiation. Differential diagnoses include metastatic tumors from sites such as mammary gland, liver or Harderian gland, and focal alveolar epithelial cell hyperplasia, as seen occasionally in older mice.