Neoplasia of the Pinna
Tumors of the ear may originate from the skin, adnexa, or connective tissue. These tumors include papilloma, fibropapilloma, mast cell tumor, cutaneous hemangioma, cutaneous hemangiosarcoma, melanoma, histiocytoma, fibrosarcoma, apocrine gland cyst, rhabdomyoma, and plasma cell tumors.2,5,6,7 Tumors can occur on either side of the pinna.
Growths that occur on the outer (convex) surface of the ear are more likely to be centrally located and rarely penetrate the underlying cartilage. Excision of these masses is readily accomplished due to the loose attachment of the skin to the underlying cartilage. When removing these masses, it is important to identify the three main branches of the auricular artery (Figure 19-9). The CO2 laser is useful in these cases. In cases where the mass is a small papilloma, the laser may be used to ablate the mass (Figure 19-10). In all other cases the laser should be used to excise the mass completely. The skin should be closed with 3-0 to 5-0 monofilament nonabsorbable suture. Even in cases that require removal of auricular cartilage, only the skin should be sutured. Deficits that cannot be closed without causing deformity to the ear should be allowed to heal by secondary intention or repaired by the use of a pedicle flap.8 The excised tissue should undergo histopathologic evaluation. Malignant or incompletely excised neoplasia requires additional treatment, up to and including amputation of the pinna. Use of the CO2 laser in these cases increases hemostasis and postoperative patient comfort, thus helping to prevent surgical complications.Sharp excision with the CO2 laser should be performed with a focal size of 0.4 mm or smaller and usually 7 to 9 watts of continuous-wave power. The power density should be great enough to incise the skin cleanly while controlling hemorrhage and causing minimal carbonization.
Superpulse delivery of energy is ideal for excision but may have a decreased hemostatic effect. Any small bleeding vessels can usually be controlled by decreasing the power density. This may be accomplished by defocusing the laser or diminishing the power output. The hemostatic effect is usually better in a continuous-wave modality without superpulse.Ablation of papillomas with the CO2 laser may be accomplished with a larger focal size, usually 0.5 mm or larger (Figure 19-11). In order to ablate tissue effectively, a sufficient power density must be applied. In most cases a power setting of 8 to 15 watts is appropriate. If an insufficient power density is used, peripheral thermal damage may occur. Multiple passes are usually required to ablate the abnormal tissue.
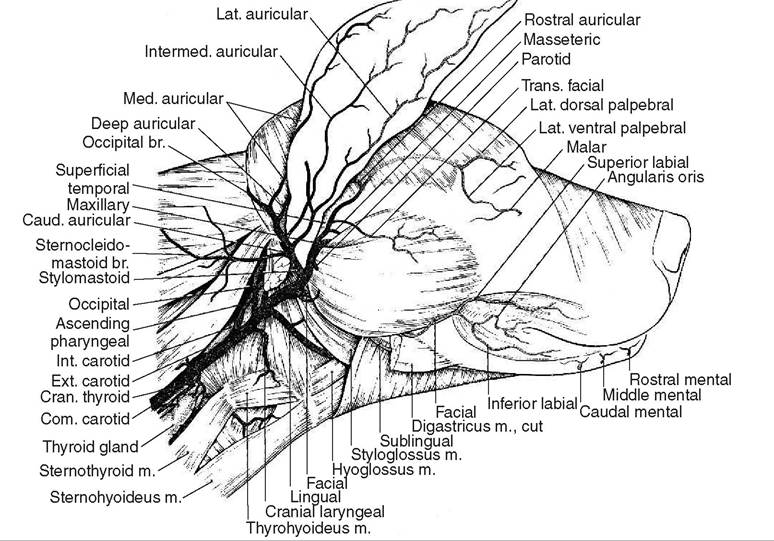
Figure 19-9
The vasculature of the canine ear. (From Evans: Miller’s Anatomy of the dog, ed 3, Philadelphia, 1993, Saunders.)

Figure 19-10
Mass on the pinna (feline).

Figure 19-11
CO2 treatment of a mass on the pinna (feline).
It is important to remove any carbonized tissue (char) that occurs between passes. Failure to remove char results in thermal injury to the surrounding tissue. If hemorrhage occurs during the ablation process, it can usually be controlled by decreasing the power density delivered to the tissue. This may be accomplished by decreasing the power setting (wattage) or defocusing the laser beam.
The diode laser may also be used. Diode laser energy is absorbed by hemoglobin, oxyhemoglobin, and melanin. This selective absorption results in excellent hemostasis and may help in the selective treatment of only the abnormal tissue. When the diode laser is used in an incisional mode, the tip of the fiber should be carbonized.
Incision with the diode laser occurs through a thermal effect on the tissue. The carbonization of the tip ensures efficient thermal transfer. Caution must be used to prevent peripheral (unintended) thermal damage. The fiber delivery system of the diode laser becomes extremely hot when energized for a prolonged period. This depends on the fiber size, the energy setting (wattage), and the vascularity of the target tissue (thermal diffusion). If the fiber becomes overheated, peripheral thermal damage will result. It is vital to keep the fiber cool. This can be accomplished by limiting the exposure time (pulse duration) and by cooling the fiber with sterile saline. Pigmented lesions may be treated in a noncontact mode. Ablation of masses in this manner may be extremely effective because of the selective absorption of diode laser energy. It is imperative to rule out malignancy before treatment. Malignant masses should be treated by complete excision with an appropriate surgical margin. Peripheral thermal damage is still a concern in the noncontact mode, and cooling of the fiber is still important. Because the fiber is not in contact with the tissue, there is no thermal diffusion of the heat that is generated. If the fiber is not properly cooled, it will rapidly become white hot. This may damage tissue as well as the plastic sheath that surrounds the fiber.