Ceruminous Gland Hyperplasia
The lining of the external ear canal is stratified squamous epithelium with sebaceous and apocrine glands and hair follicles.10 The apocrine glands in this area are also referred to as ceruminous glands.
Springer Spaniels, Cocker Spaniels, and black Labrador Retrievers have an increased proportion of these ceruminous glands.11 This may explain the higher incidence of otitis externa in these breeds. Patients with chronic otitis externa develop hyperplasia of the ceruminous and sebaceous glands (Figure 19-12).12 Hyperplasia leads to decreased diameter of the ear canal as glandular tissue increases, and it also results in increased ceruminous secretions within the ear canal. Cocker Spaniels appear to develop primarily ceruminous gland hyperplasia with less fibrosis than other breeds.13 In another study the quantity of sebaceous glands was found to be similar in dogs with and without otitis externa. In this study dogs with otitis externa were found to have a higher population of ceruminous glands.14 It is important to remember that chronic otitis externa is usually not a primary disease. It is usually caused by some underlying allergy or unresolved chronic infection. As part of the therapy, it is important to address any underlying problem. Failure to resolve or at least control the underlying problem results in temporary palliation of the problem at best.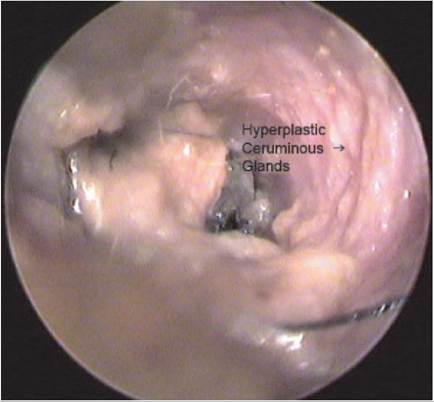
Figure 19-12
Hyperplasia of the ceruminous glands.
Before initiating treatment of the affected ear, swabs for cytology and bacterial culture should be obtained from just in front of the tympanic membrane (if present) or the middle ear if there is an obvious rupture of the membrane. Appropriate medications can then be prescribed and adjusted based on these results.
After the culture and cytology specimens have been obtained, the ear is thoroughly cleaned with a ceruminolytic agent and lavaged with copious amounts of saline. This should be done under direct visualization through the video otoscope. A complete evaluation of the ear canal may then be performed. Any hyperplastic areas within the ear canal should be easily visualized. Biopsies of the abnormal tissue should be taken for histopathology. The results of the histopathology may help to identify the underlying disease process. Hemostasis after the biopsy can be accomplished with the CO2 or diode laser. The diode laser may be more clinically useful in this situation because it can be used in a fluid environment (Figure 19-13). A 600-micron fiber is used to deliver the diode laser energy. A setting of 3 to 4 watts in continuous wave mode usually rapidly accomplishes hemostasis.
The CO2 laser may also provide hemostasis to the biopsy sites. The CO2 laser’s energy should be directed to the target site under direct visualization. This allows for accurate hemostasis and treatment with little iatrogenic damage to surrounding tissue. This is accomplished through a flexible, hollow waveguide. The CO2 laser’s energy must be directly applied to the hemorrhaging area. This means that adequate suction must be applied to the area for the laser energy to have the desired hemostatic effect. If sufficient suction cannot be obtained, the blood itself will be vaporized,

Figure 19-13
Diode laser coagulation. producing significant char and possibly resulting in inadequate hemostasis and peripheral thermal damage. CO2 laser hemostasis can usually be obtained with a power setting of 2 to 4 watts with a 0.8-mm focal size in a continuous-wave mode.
After hemostasis has been achieved, removal of the abnormal tissue can be accomplished; lasers are useful in this procedure.
The laser is used to ablate the abnormal tissue. Removal of this tissue helps to increase the diameter of the ear canal and decrease the amount of secretions within the ear. Diode laser energy may be used for this procedure. The size of the fiber depends on the size of the operating channel in the video otoscope or therapeutic telescope or the size of the targeted area. Generally, fibers of 600 to 1000 microns are used. Because the laser is being used in a contact mode, the energy is precisely directed into the target tissue. Another advantage of the diode laser is its ability to operate in an aqueous environment. Continuous irrigation of the ear canal improves visualization by removing any blood or debris from the surgical field. It also diminishes or eliminates peripheral thermal damage. Power settings vary depending on the size of the fiber used and the size of the target. It is important to provide sufficient power to ablate the target tissue without causing peripheral damage. Diode laser energy penetrates more deeply than CO2 laser energy, and care must be taken to avoid damaging the deeper structures. In general, a 600-micron fiber requires 6 to 12 watts of power to obtain the desired effect. A 1000-micron fiber requires 10 to 20 watts for a similar effect. The energy is delivered in continuous wave, and exposure times should generally be less than 3 seconds. The irrigant solution should not reach the boiling point. Bubbles will begin to form around the fiber if the solution is overheated. Prolonged exposure times increase the risk of peripheral thermal damage by overcoming the cooling effect of the irrigant and the thermal relaxation time of the tissue.CO2 laser energy can also be directed at the abnormal tissue as described previously (Figure 19-14). This energy vaporizes the abnormal tissue. CO2 lasers cannot currently be used immersed in a fluid environment. Evacuation of the smoke (plume) produced during vaporization is vital.
This allows for better visualization of the target tissue and is an important factor in the safety of operatory personnel. During the course of therapy a layer of char may form on the targeted tissue. It is essential to stop and remove this substance. If the carbonized layer is not removed, it absorbs the CO2 laser energy and results in inadvertent peripheral thermal damage. The amount of carbonization and peripheral thermal damage is generally greater if an insufficient power density is used. A spot size of 0.8 mm with 8 to 14 watts of power in continuous- wave mode usually results in adequate vaporization with good hemostasis.After the abnormal tissue has been removed, the ear canal should be lavaged with copious amounts of irrigant and any carbonized tissue gently removed. The ear is gently dried with suction and an appropriate topical antimicrobial with steroid instilled. It is important to evaluate fully the tympanic membrane because some medications may be ototoxic if the tympanic membrane is not intact. A myringotomy should be considered in cases of chronic otitis externa (see the section on Myringotomy later in this chapter). The short-term use of parenteral steroids may be indicated in some cases. Postoperatively most patients receive 0.006 mg/kg of buprenorphine (Buprenex) intravenously during the recovery period. Additional pain medication is usually

Figure 19-14
CO2 ablation of hyperplastic ceruminous glands.
not required. Most patients seem markedly more comfortable postoperatively and are usually less resistant to the continued treatment of their ears.
Laser ablation often greatly improves the clinical outcome for cases of chronic otitis with ceruminous gland hyperplasia. Removal of the hyperplastic tissue increases the diameter of the ear canal, decreases the amount of discharge, helps remove some of the bacteria, and allows the owner to clean and maintain the ears more thoroughly. Postoperatively, most patients are very comfortable and readily allow the owner to treat the ears. Weekly follow-up visits that include otoscopic evaluation and ear swabs for cytology are imperative. Treatment should continue until the ears look normal and for 1 week after a negative swab is obtained. After healing, the ablated glandular areas are replaced with fibrous tissue covered by epithelium.
It is extremely important to use antibiotics based on culture and sensitivity in cases of bacterial infection. Many of these cases are a result of multidrug-resistant bacteria. Oral antibiotic or antifungal agents may be useful in the management of these cases. In addition, any underlying food allergy, inhaled allergy, contact dermatitis, or endocrinopathy should be properly evaluated and addressed.
More on the topic Ceruminous Gland Hyperplasia:
- Zymbal's Gland and Preputial Gland Tumors
- Etiolog y of Ceruminous Otitis
- Environmental and Conformational Causes of Ceruminous Otitis
- Harderian Gland Neoplasia
- 1O Ceruminous Diseases of the Ea
- Biliary Hyperplasia
- CONGENITAL ADRENAL HYPERPLASIA
- SEBACEOUS GLAND DISORDERS
- SWEAT GLAND DISORDERS
- Pituitary Gland Adenoma
- Bulbourethral Gland Cysts
- Renal Papillary Hyperplasia