Pituitary Gland Adenoma
Pituitary adenomas are very common tumors that arise in older animals, particularly in Sprague-Dawley and Wistar rats. In addition to age, genetic factors, diet, and breeding history may play a role.
Reduction in food intake reduces the incidence of spontaneous pituitary tumors, and mated females have been shown to have a lower incidence of pituitary tumors than did virgin females. In some studies, there is a slightly higher incidence in females, but this is not a consistent finding. Clinical signs vary, from animals that are subclinical to animals with severe depression, frequently with incoordination. The majority of pituitary tumors are interpreted to be chromophobe adenomas. Acidophil and basophil tumors have also been described. Immunohistochemical techniques are required for positive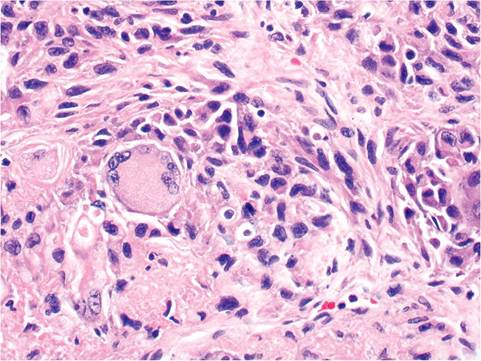
FIG. 2.90. Histiocytic sarcoma in the liver of an aged rat, illustrating multinucleated giant cell formation, which is common in this type of neoplasm.
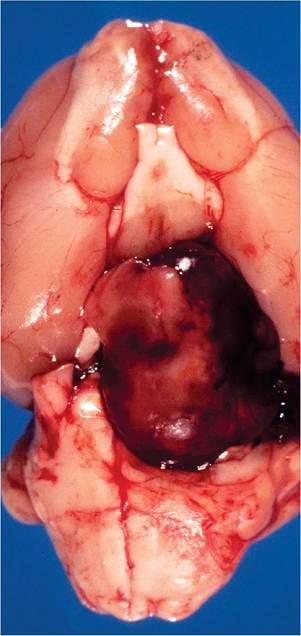
FIG. 2.91. Pituitary gland adenoma in an aged female Wistar rat. Note the hemorrhagic appearance of the large fleshy mass.
identification of cell type. In pituitary tumors studied by immunocytochemistry, prolactin-producing tumors are the most common type. Most tumors are interpreted to arise from the pars distalis, although tumors of the pars intermedia have also been described. Pituitary carcinomas are relatively uncommon.
Pathology
The pituitary is enlarged, frequently with prominent lobulations. Tumors are often dark red to brown and hemorrhagic in appearance (Fig. 2.91). In larger tumors, there may be minimal to marked compression of the overlying mesencephalon. On microscopic examination, the anterior pituitary consists of cords or nests of glandular cells bound by strands of connective tissue, with an abundant cavernous vascular capillary network.
The cells typically have large nuclei and prominent nucleoli, with abundant, lightly basophilic to amphophilic cytoplasm consistent with a chromophobe adenoma (Fig. 2.92). Giant nuclei may be present in the mass. Mitotic figures are occasionally observed. A pseudocapsule composed of a fine band of connective tissue separates the tumor from the adjacent pituitary tissue. More than 1 tumor may be present in an affected gland. Nodules of hypertrophic or hyperplastic cells may be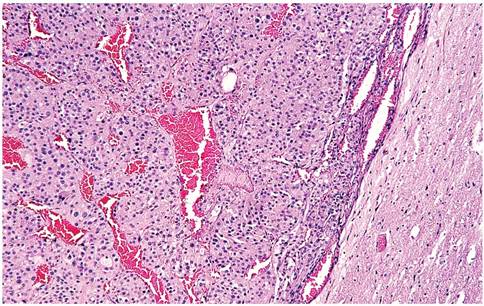
FIG. 2.92. Pituitary adenoma, with prominent cords of epithelial cells interspersed within a vascular stroma.
present in glands and must be differentiated from adenomas. They occur as islands of large cells, sometimes with mitoses, but there is no evidence of pseudo-encapsulation or compression of adjacent tissue.
Testicular Interstitial Cell Tumors
Interstitial cell tumors occur frequently in male F344 rats, reaching a prevalence of 100%. Tumors are often multicentric and involve one or both testes. On gross examination, they appear as circumscribed, lobulated, light yellow to hemorrhagic (Fig. 2.93). Microscopic changes are consistent with tumors of Leydig cell origin, with a spectrum of lesions ranging from small microscopic nodules to large tumors. Masses are composed of cells of 2 types: polyhedral to elongated cells with granular to vacuolated cytoplasm and smaller cells with hyperchromatic nuclei and scanty cytoplasm (Fig. 2.94). Interstitial cell tumors have been associated with concurrent hypercalcemia.
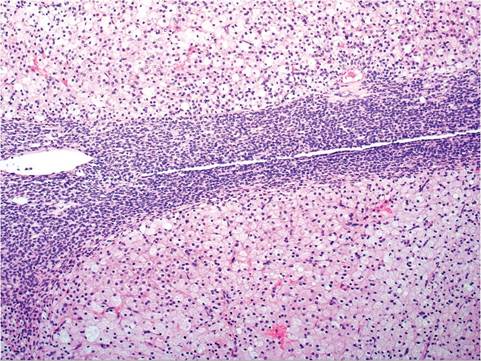
FIG. 2.94. Interstitial cell tumor from an aged Fischer 344 rat. These tumors are typically composed of 2 morphologically distinct cell types, consisting of cells with minimal cytoplasm, which are usually at the periphery of nodules, and cells with abundant cytoplasm that are more centrally located. Both cell types are of Leydig cell origin.
More on the topic Pituitary Gland Adenoma:
- Pituitary Gland Adenoma
- Pituitary Adenomas and Hypopituitarism9,12
- Zymbal's Gland and Preputial Gland Tumors
- Bulbourethral Gland Cysts
- Mesenchymal Neoplasms Rhabdomyosarcomas
- BIBLIOGRAPHY FOR NEOPLASMS