Laser Polypectomy (Aural Tumor Removal)
Tumors can occur within the ear canals and middle ears of both dogs and cats. Tumors occur more frequently in dogs than in cats. The tumors that occur in dogs are usually less malignant than those that occur in cats.15 Malignant tumors should be treated by total ear canal ablation and lateral bulla osteotomy.
Both favorable and unfavorable long-term results from surgery alone have been reported.16 The most common tumor found in the external ear canal of both dogs and cats arises from the ceruminous gland. Ceruminous gland adenomas are more common than ceruminous adenocarcinomas in the dog. In cats the tumors are more likely to be adenocarcino- mas.17 These masses can be an underlying cause or a result of chronic otitis.In feline patients, inflammatory polyps can arise from the epithelium of the tympanic cavity or the eustachian tube.18 Feline polyps can grow distally into the ear canal (Figure 19-15) or proximally into the retropharynx. It is therefore extremely important to evaluate the middle ear in cases of feline retropharyngeal polyps. Failure to remove this tissue from the middle ear may result in recurrence. Canine polyps can occur anywhere in the ear canal (Figure 19-16). These are usually cerumen gland adenomas and may occlude the entire ear canal. They may also grow into the middle ear. True retropharyngeal polyps in dogs are rare.
Before the advent of video otoscopy, complete excision of polyps within the ear canal often required a lateral ear canal resection to obtain the necessary access to the mass. This procedure, followed by laser excision of the mass(es) within the auditory canal, may still be necessary. The video otoscope allows improved identification and evaluation of these masses. Once identified and evaluated, they can usually be successfully removed by traction and/or laser vaporization.
Lasers offer significant improvements in the treatment of these lesions. The treatment of benign polyps in the ear canal is best accomplished as a two-step procedure. It is in the patient’s best interest that the clinician obtain a biopsy and a definitive diagnosis before attempting to ablate any mass. As previously stated, malignancies

Figure 19-15
Feline polyp arising from the middle ear.
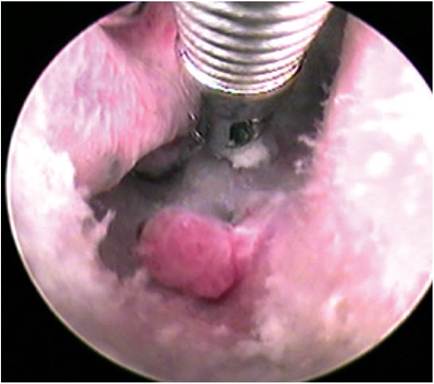
Figure 19-16
Canine polyp.
are best treated by resection of the entire ear canal. In addition, antibiotics can be started based on culture and sensitivity before mass removal.
In the first step cultures and biopsy specimens can be obtained through the operating channel of the video otoscope. Hemostasis is achieved with the CO2 or diode laser, as explained in the previous section.
After the masses are identified, both CO2 and diode lasers can ablate these masses within the ear canal. Diode laser energy may be superior in the removal of larger polyps. Diode lasers do not create carbonized tissue, and they operate in a fluid environment. This allows increased visualization of the target tissues and precise application of laser energy. In addition, simultaneous lavage prevents hemorrhage or plume from interfering with visualization. In most cases, any source of hemorrhage can be readily identified, and the diode laser can provide hemostasis.
When the diode laser is used, irrigation with saline is provided continuously. Irrigation is vital to visualization and essential to the prevention of peripheral thermal damage. Normal saline (0.9%) is currently the solution of choice. Depending on the size of the patient and the size of the mass, a 600- or 1000-micron fiber is used. The fiber is introduced into the center of the mass, and energy is provided until a majority of the abnormal-seeming tissue has a blanched appearance.
This devitalized tissue is then removed with a biopsy forceps. It is often necessary to repeat this process in larger masses.In some cases the tumor may be large enough to fill the entire auricular canal. It is possible to remove these masses with a laser and a video otoscope. To expedite the removal it may be useful to debulk the mass with a larger-diameter biopsy forceps placed alongside the endoscope. These forceps can then be positioned under direct visualization. Blakesley or Takahashi nasal forceps are well suited for this

Figure 19-17
Nasal biopsy forceps.
procedure (Figure 19-17). In this manner, large masses can be rapidly reduced. Biopsy forceps of 3.5 to 5.0 Fr can also be introduced through the operating channel to debulk these masses (Figure 19-18). With this method, moderate hemorrhage is encountered. It is essential to provide adequate irrigation to allow visualization; irrigation is provided through the biopsy channel of the video otoscope. After debulking, hemostasis and removal of the remaining abnormal tissue is performed with the diode laser, as described previously. Rapid debulking can also be accomplished with an arthroscopic shaver. A hooded debrider blade provides rapid debulking while protecting the normal auricular canal. This system offers improved visualization because suction is provided by the shaver. Because irrigation is provided via the video otoscope, simultaneous irrigation and suction can occur.
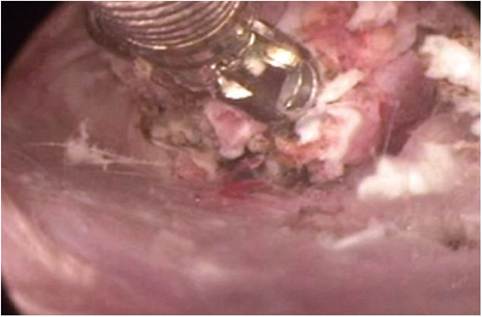
Figure 19-18
Debulking of a polyp with biopsy forceps.
By prepositioning the diode fiber in the operating channel of the video otoscope, hemostasis can be rapidly achieved, minimizing any blood loss. These debulking techniques can help to markedly reduce the surgical time required to remove larger masses. By using the laser to provide hemostasis and remove the final layer of abnormal tissue, the advantages of laser surgery can be preserved.
Patients treated in this manner have minimal postoperative discomfort, edema, or hemorrhage. Power settings for the diode laser depend on the size of the fiber, the size of the mass, and whether ablation or hemostasis is desired. In general, a 600-micron fiber requires 6 to 12 watts of power for ablation (Figure 19-19) and 2 to 4 watts for hemostasis. A 1000-micron fiber requires 10 to 20 watts for ablation and 3 to 5 watts for hemostasis. As previously stated, the energy is delivered in a continuous wave, and exposure times should be limited to prevent the irrigant solution from reaching the boiling point. Bubbles will begin to form around the fiber if the solution is overheated. Overheating the irri- gant increases the risk of peripheral thermal damage. Peripheral thermal damage markedly increases the patient’s postoperative discomfort.CO2 lasers can also be used to remove large masses (Figure 19-20). In this procedure the mass is ablated in layers (Figure 19-21). Relatively high power is applied in a continuous-wave manner. Char must be removed between layers. Failure to remove this char will result in peripheral thermal damage. In some cases it may be possible to reduce the size of the mass by debulking. The hemorrhage that results from debulking can be difficult to control. In order to provide hemostasis, the CO2 laser’s energy usually must contact the end of the bleeding vessel. Due to the confined area of the auricular canal, blood can often fill the area, making it difficult to visualize the source of the hemorrhage. This limitation can sometimes be overcome by the use of a suction trap in the smoke evacuation line. The suction trap allows the smoke evacuator to function as a suction unit. The smoke evacuator should be directly connected to the otoendoscope; this may require a T or Y adapter so that both the laser and the suction unit can be active at the same time. In most CO2 laser units, a

Figure 19-19
Treatment of a polyp with a diode laser.
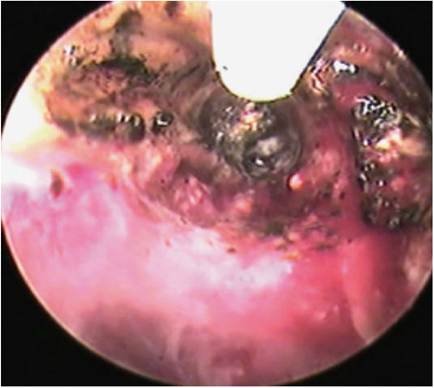
Figure 19-20
CO2 laser ablation of a large mass.
column of air is produced and exits the laser aperture. This air is designed to keep the aperture free of debris, but it may also help in visualizing the source of the hemorrhage. In some cases the amount of hemorrhage is great enough to prevent laser coagulation. In these cases, hemostasis must be achieved in another manner before the procedure is continued; direct pressure or electrocautery is usually effective. Electrocautery should be used with caution. It may cause peripheral damage and can greatly reduce the potential benefits of laser surgery.
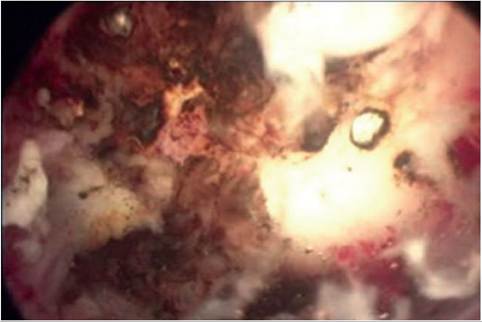
Figure 19-21
Middle ear after laser mass removal.
More on the topic Laser Polypectomy (Aural Tumor Removal):
- Aural Hematoma
- WILMS TUMOR
- Specific Laser Therapy Goals
- A Comparison of CO2 and Diode Laser Energy
- Removal
- 19 Laser Ear Surgery
- 3 Fixtures and Buildings – Right of Removal
- 4 Removal of fruit trees, bushes, etc
- C REMOVAL OF SECURITY: THE CASES FOR POSSESSION
- 6.57 Farming being capital intensive in nature, it is of central importance that the rights and liabilities of landlord and tenant as to the provision, repair, maintenance and removal of fixed equipment are clearly defined.
- Lateral Ear Canal Resection and Ear Canal Ablation
- Conclusion
- Cosmetic and Therapeutic Otoplasty
- Testicular Cancer and Germ Cell Tumors
- Neoplasia of the Pinna