Specific Laser Therapy Goals
A treatment plan for the individual patient is based on the anatomic location and the suspected underlying etiology. These variables influence both the type and delivery method for the laser energy.
In some cases multiple problems are present. These may require multiple wavelengths or delivery systems, which should be available in advance to facilitate the procedure.CO2 and diode laser energy allow for a more targeted removal or alteration of tissue. The ear canal is a confined space to work in and around, and the pinna has limited additional dermis with which to work. A laser can simplify a number of procedures, improve near-term recovery, and provide for more normal anatomy and return to function. This can be accomplished by incorporating laser-directed ablation (vaporization), incision, or excision of tissues. As discussed earlier, disease components in the ear that are predisposing to or perpetuating the disease can then be more efficiently removed with cleaning, medication, and evacuation.
The first step in the use of laser energy is to determine the way the energy is to be applied to the target tissue. Typically on the pinna, standard laser techniques can be used to accomplish the desired goals. Here the CO2 laser is clearly superior because of its reduced peripheral thermal tissue interaction and noncontact application. Surgery of the pinna can be provided by laser energy, similar to techniques for other areas of the dermis. In the external ear canal the video otoscopic or fiberoptic telescope can be used to facilitate visualization and direction of the laser energy. This is usually accomplished by extending the direction of the laser energy through special tips that fit into and through working channels in the otoscopic equipment. Diode laser fibers are usually between 400 and 1000 microns and easily fit most working channels.
This allows the clinician to visualize the area and provide treatment within the confined space of the external ear canal.Treatment of Aural Hematomas
Aural hematomas occur when a vessel within the pinna ruptures and blood accumulates under the skin. Aural hematomas occur on the inner (concave) surface of the pinna and can occur in both dogs and cats (Figure 19-6). Because the skin is so firmly attached to the auricular cartilage on the concave surface, the hematoma actually develops subparachondrally or intrachondrally, not subcutaneously.1 Most aural hematomas are lined by cartilage; this suggests that damage to this cartilage may play a role in their occurrence.2 The etiology of this condition is unknown. It may result from self-trauma or head shaking (secondary to otitis externa or media or to
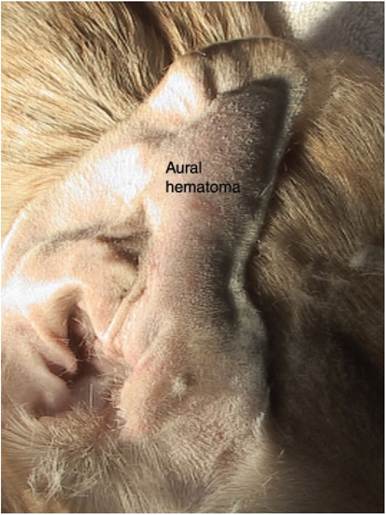
Figure 19-6
Canine aural hematoma. external parasites), trauma, increased vascular fragility, hemorrhagic diathesis, or some form of immune-mediated disease.3 Any underlying pathology should be addressed as part of the therapy. It may be wise to delay treatment in thrombocytopenic patients until any platelet abnormality has been corrected.
A variety of treatment methods have been published to repair aural hematomas. These treatments require various degrees of aftercare and some failures do occur. The CO2 laser is extremely useful in the treatment of this condition. It reduces postoperative discomfort and the amount of aftercare required.
After the induction of anesthesia or heavy sedation, the affected ear is fully evaluated. Any evidence of otitis externa or media should be addressed at this time. If there has been a history of chronic otitis, ear swabs for cytology and culture and sensitivity should be obtained and a complete video otoscopic ear examination performed in both ears. Ear disease in one ear may result in an aural hematoma in the other ear from the constant head shaking.
After the evaluation has been completed, the inner pinna of the affected ear is clipped and prepared for aseptic surgery. The patient is positioned in lateral recumbency with the affected side up.Three or more round, partial-thickness circular skin incisions of approximately 0.3 to 0.7 centimeters are made in a triangular pattern (Figure 19-7). The size of the opening depends on the size of the patient. After this pattern has been made, one of the proximal incisions is continued to full thickness to penetrate the hematoma. At this time the fluid within the hematoma is removed. This fluid is usually hemorrhagic to serohemorrhagic, depending on the length of time the hematoma has been present. After the fluid has been removed, the remaining incisions are continued to full thickness. At this time any fibrin clots should be removed from the subcutaneous

Figure 19-7
Ear pinna after creation of laser drain perforations. space. It may be useful to lavage the space gently with normal saline or lactated Ringer’s solution.
The skin is then sutured with stented 0 Prolene or nylon (3-0 Prolene for feline patients) to the underlying cartilage in a simple interrupted pattern. Only the inner pinna and the cartilage are sutured (Figure 19-8). The sutures should not penetrate the outer (dorsal) skin surface of the pinna. A taper needle is less likely to cause inadvertent bleeding and is preferred. The long axis of the individual sutures should be parallel to the long axis of the ear. This helps to preserve the normal blood supply to the pinna and avoid the three major branches of the auricular artery. After completion of the procedure, 0.006 mg/kg of buprenorphine (Buprenex) is given intravenously. Usually no additional pain control medication is required. An Elizabethan collar is placed to prevent self-trauma. Bandaging of the ear is not necessary or recommended. An alternative procedure that does not involve sutures has been published and may also be effective.4
Aftercare is performed at home by the client.
This consists of twice-daily hot compresses applied to the ear for 5 to 10 minutes each. Any scab that forms should be removed, and the drain holes should be kept open for as long as possible. Any reaccumulation of fluid should be gently expressed during the process of compressing. Follow-up visits should be encouraged on a weekly basis. The drain holes
Figure 19-8
Postoperative appearance of the ear. usually will close by the second postoperative week. Sutures should be left in place for approximately 7 days after they have closed. Any otitis that is discovered during the course of treatment must be fully and aggressively treated. It is recommended that the otitis be completely resolved for at least 5 days before suture removal.
This procedure is relatively easy to perform, has a low recurrence rate and a low degree of morbidity and mortality, and achieves excellent cosmetic results. Most patients have no noticeable deformity from the procedure and have excellent postoperative comfort.
More on the topic Specific Laser Therapy Goals:
- A Comparison of CO2 and Diode Laser Energy
- 19 Laser Ear Surgery
- As we have just seen, Plasmodium has specific mechanisms that enable it to live inside a red blood cell. When both a parasite and its host possess such specific mechanisms, that observation suggests that the strong selection pressure that hosts and parasites impose on each other has caused their populations to evolve.
- Laser Polypectomy (Aural Tumor Removal)
- Mission and Goals of CAMTS
- Mission and Goals of CAMTS
- Ecosystem management sets sustainable goals, implements policies, monitors effectiveness, and adjusts as necessary
- PARENTERAL FLUID THERAPY
- Specific Drug Treatment
- Like other organizations, transport teams require a clear vision to achieve objectives and enable managers and administration to meet important organizational goals
- Like other organizations, transport teams require a clear vision to achieve objectives and enable managers and administration to meet important organizational goals