Non-Hodgkin's Lymphoma
The occurrence of non-Hodgkin's lymphoma (NHL) was known to complicate immunodeficiency states before the advent of HIV. Up to 20% of HIV positive people may ultimately develop NHLs and it is the presenting diagnosis in 3% of patients.
In immunodeficiency NHLs are commonly extranodal.Aetiology
Both HIV itself and its related opportunistic infections may cause polyclonal B-cell expansion which is probably cytokine and antigen driven. Patients with AIDS have impaired immunity to EBV when compared to HIV negative EBV-infected individuals and EBV is itself likely to cause polyclonal B-cell proliferation. AIDS lymphomas have modified immunoglobulin variable regions which are consistent with antigen drive as an important factor in lymphomagenesis. Macrophages, acting as antigen-presenting cells, also appear to be clonally expanded. When CD4+ T-cell levels fall, antigen levels rise and the risk of lymphomagenesis increases. Such proliferation allows for sequential genetic errors leading to a monoclonal and hence malignant transformation.
Pathology
Systemic lymphomas in AIDS are pathologically diverse. A diffuse small non-cleaved subset is unique to HIV patients and is associated with elevated IL-6 and soluble CD23 levels. It is less frequently associated with EBV than the diffuse immunoblastic or diffuse large cleaved cell subtypes. Histological type does not currently affect prognosis although the different subtypes are clinically separate. All these subtypes are high grade.
Immunohistochemistry reveals positive staining for CD20 in 90% of B-cell lymphomas.
Box 5.2 Summary of malignancies
AIDS-defining malignancies
• Kaposi's sarcoma
• High/intermediate grade non-Hodgkin's lymphoma including primary
CNS lymphoma
• Cervical carcinoma
Other malignancies with increased incidence
• Hodgkin's disease
• Ano-genital squamous cell carcinoma
• Testicular germ cell tumours
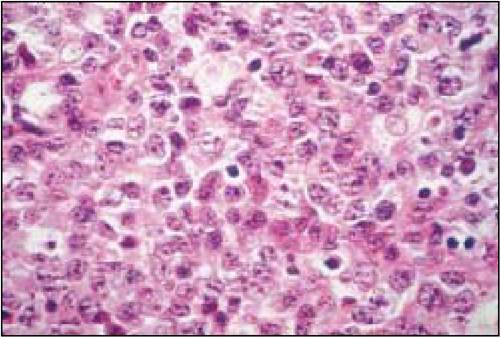
Figure 5.8 HIV-related non-Hodgkin's lymphoma
Clinical presentation
NHL can occur at any stage of immunodeficiency with approximately one-third of patients with AIDS-related NHL having a previous AIDS diagnosis.
Stage III or IV disease accounts for 70%-80% of cases (see Box 5.3) with a majority of patients presenting with extranodal disease. Common sites are the gastrointestinal tract, liver and bone marrow. Bone marrow involvement occurs in 20%-30% of cases and exacerbates chemotherapy-induced bone marrow toxicity.NHL is associated with B symptoms of sustained fever greater than 38°C, weight loss (greater than 10% of body weight) and night sweats. All of these symptoms may occur in an HIV positive patient without NHL and so are of limited diagnostic and prognostic use in this clinical setting.
Box 5.3 Ann Arbor: classification of lymphoma
Stage I Single lymph node region +/- local spread to extralymphatic tissue (E)
Stage II Two or more node regions on same side of diaphragm +/- local spread to extralymphatic tissue (E)
Stage III Involved nodes both sides of the diaphragm
Stage IV Diffuse or disseminated involvement of one or more extralymphatic organs
Prognosis is poor with a median survival of 4—6 months in spite of an often good early response to treatment. A previous AIDS-defining illness, a CD4 count is usually with bulky or advanced stage disease and 50% have bone marrow involvement. Most patients have B symptoms. In the HIV negative population Hodgkin's disease is typified by contiguous spread, this is not the case in HIV patients. Histologically tumours are usually high-grade mixed cellularity (41-100%) and lymphocyte-depleted subtypes (20%) and behave aggressively. Between 80% and 100% of Hodgkin's disease tissue from HIV-infected individuals is associated with EBV infection and this is probably relevant in pathogenesis. Treatment is with combination chemotherapy using standard regimens such as ABVD (doxorubicin, bleomycin, vinblastine and dacarbazine) and antiretrovirals. Bone marrow toxicity makes GCSF and dose reductions frequent necessities. If patients can continue their antiretroviral therapy throughout
chemotherapy they suffer less immunosuppression.
Complete responses following chemotherapy are seen in 45—70%.Median survivals are 12—18 months and whilst not being an AIDS-defining condition 94% of patients progress to AIDS by 2 years. Good prognosis is associated with no prior AIDS diagnosis, CD4 >250 ? 106∕l and complete response to treatment.
Ano-genital squamous cell carcinoma
Anal cancer like cervical cancer is related to human papillomavirus. HIV positive patients are two to six times more likely than HIV negative persons to have anal human papillomavirus infection. Persistence of infection is inversely related to CD4 count. Low-grade anal intraepithelial neoplasia is more likely to progress to high grade anal intraepithelial neoplasia in HIV positive patients. However it remains unclear whether HIV directly affects the development of anal carcinoma.
There is a threefold increase in incidence in testicular germ cell tumour s in homosexual HIV positive men. Seminoma is much more common than teratoma. Lung cancer of all histological types, non-melanomatous skin cancers, angiosarcomas and paediatric leiomyosarcomas may all be increased in HIV infection. Lung cancers occur at an earlier age and have a poorer prognosis in the HIV positive population.