Kaposi's sarcoma
Among the first reported illnesses amongst homosexual men in the USA in 1981 was Kaposi's sarcoma (KS), with 20-40% of HIV-infected homosexual men suffering KS. Hitherto KS had been known in three forms.
In elderly Jewish or Eastern European patients as “classic” KS, in sub-Saharan Africa as “endemic” KS, and more recently in transplant and other immunosuppressed patients. KS currently remains the most frequent neoplastic condition in AIDS.Aetiology
The uneven geographical distribution of KS had long suggested that environmental factors were aetiologically important. Epidemiological observations that KS initially occurred in clusters in the HIV population and that it was 20 times more likely in homosexual men than other risk groups suggested a sexually transmitted cofactor. Work in the biological and statistical fields has gone on to establish causality. Whilst no biological pathway has yet been identified, there is now sufficient evidence to state that a DNA virus, Kaposi's sarcoma-associated herpes virus (KSHV) also known as human herpes virus 8 (HHV8), is an essential, although not necessarily a sufficient, cause of KS.
This evidence has primarily come from longitudinal studies showing that KSHV infection precedes KS. This is consistent with analogous evidence of other herpes viruses, for example Epstein-Barr virus (EBV) being oncogenic. KSHV has been detected in tissue biopsies taken from patients with African and classical KS as well as AIDS-related cases.

Figure 5.1 Classical Kaposi's sarcoma
KSHV can be sexually transmitted and seroconversion has been noted following renal transplantation. In endemic areas non-sexual horizontal and vertical spread are the proposed dominant modes of transmission. The evidence for this is the age-dependent increase in KSHV seroprevalence in prepubescent children in studies from Gambia and Uganda and the greater (29% compared to 0%) seropositivity rate in children born to KSHV seropositive women in South Africa.
Histopathology
The tumours have a characteristic appearance, consisting of groups of spindle cells separated by slits giving a sieve pattern. These spindle cells derive from primitive mesenchymal cells. Red cells are often seen in the slits and early lesions may consist almost entirely of bizarre endothelium-lined vascular spaces in the dermis with few spindle cells.
The tumour stains positive for factor VIII and smooth muscle-specific α-actin on immunocytochemistry staining.
The following cytokines have been shown to promote the growth of KS cells in vitro: interleukin 6 (IL-6), tumour necrosis factor (TNF), basic fibroblast growth factor (bFGF), vascular endothelial growth factor (VEGF), platelet-derived growth factor (PDGF), Oncostatin M and granulocyte colonystimulating factor (GCSF). It may be possible to exploit this therapeutically by inhibiting these cytokines.
Kaposi's sarcoma is a multifocal process rather than a metastatic one.
Clinical presentation
The classic form tends to follow a very indolent course producing large ulcerated plaques on the lower legs. It shows a strong male preponderance and as most affected individuals are elderly their KS causes significant morbidity but not mortality.
Endemic KS follows a more aggressive course in younger adults with more florid skin lesions and lymph node involvement. Death occurs due to widespread systemic involvement. In young children the lymphadenopathic variant is most commonly seen.
In the non-HIV immunosuppressed patient the lesions of KS may improve with reduction or cessation of the immunosuppression.
In the UK these forms are all rare and most cases of KS are AIDS related.
The presentation of KS in AIDS is variable but the disease tends to become increasingly aggressive and may be lethal. Mucocutaneous lesions begin as flat dusky red papules progressing over weeks or months to vary from a few scattered nodular lesions to large plaques. The legs, trunk, arms, face, hard palate and penis are common sites with associated “woody” oedema and ulceration predominantly affecting the lower limbs.
KS on the feet make walking difficult and painful. Other mucocutaneous lesions often cause distress because of their disfiguring appearance.All organs other than the central nervous system may be affected and the presence of visceral disease is predicted by mucocutaneous disease; one third of respiratory “episodes” in patients with cutaneous KS are due to pulmonary KS. The most common visceral lesions are pulmonary and gastrointestinal. Lymph node disease is also common and may cause venous compression resulting in gross peripheral oedema. Presentation of pulmonary KS is usually with exertional dyspnoea but may be with cough or haemoptysis. Chest radiograph changes are often non-specific with interstitial infiltrates, pleural effusions and mediastinal lymphadenopathy. Further information is gained by bronchoscopy and CT; if possible bronchial biopsy should be avoided as bleeding may be heavy (see chapter 6).
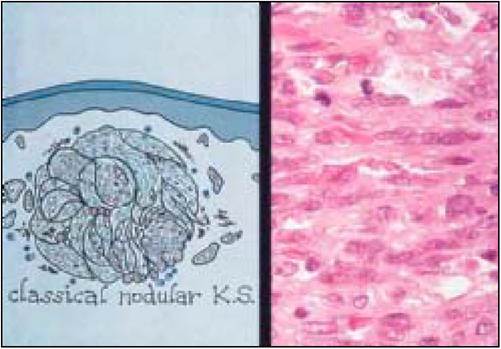
Figure 5.2 Classical nodular Kaposi's sarcoma
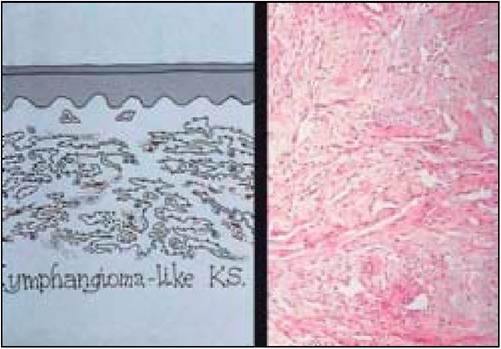
Figure 5.3 Lymphangioma-like Kaposi's sarcoma

Figure 5.4 Kaposi's sarcoma
Lesions may occur along the length of the gastrointestinal tract from the palate to the anus and diagnosis is by endoscopy. KS in the oral cavity and oesophagus may cause pain but is usually asymptomatic. Bleeding may occur from lesions throughout the gastrointestinal tract and patients may also suffer protein-losing enteropathy and diarrhoea.
KSHV is also found in two rarer malignancies, primary effusional lymphoma (a subset of B-cell non-Hodgkin’s lymphoma) and multicentric Castleman’s disease, a lymphoid malignancy which also has an increased incidence in AIDS.
Incidence
KS was the AIDS-defιning diagnosis in 30% of patients in the 1980s but this has now fallen.
The reduction may be attributed to changes in sexual practices as well as the advent of antiretroviral therapy. KS commonly precedes opportunistic infections and with improvements in treating such infections KS is increasingly common as the cause of death for AIDS patients. Hence whilst the incidence of KS is falling the prevalence is increasing. The deaths of almost 30% of AIDS sufferers are now accounted for by visceral and particularly pulmonary KS.Treatment
Treatment must be tailored to the site and extent of KS and to the patient’s underlying clinical condition. The aim of treatment is resolution of symptoms and prolongation of life. Cure is currently impossible due to the disseminated nature of the condition and its poorly understood pathogenesis as well as the underlying AIDS. HAART has reduced the need for second-line therapies by increasing median time to treatment failure as well as reducing the incidence of KS. There are reports of KS regression with HAART and no other treatment.
Local treatment is important for cosmesis of cutaneous lesions. Superficial radiotherapy is given using 100kV X-rays applied directly to the skin or palate. A dose of 8Gy in a single fraction achieves good palliation in 70% of lesions, particularly in early KS with little haemosiderin staining. The area of the lesion is treated with a margin using a lead cutout to protect surrounding tissues. The dose should be given in divided doses on consecutive days (fractionation) to sensitive areas such as the soles or face. Radiotherapy can be repeated if further regression is required or relapse occurs. Alternative treatments include camouflaging with cosmetics and intralesional injection with vinblastine or interferon.
Palatal, bronchial and oesophageal KS can also be treated with radiotherapy. It is particularly useful to stop bleeding.
For extensive mucocutaneous disease or visceral involvement chemotherapy is the preferred option. Several regimens are available and choice of regimen depends on coexistent pathologies and, in some countries, availability and price.
Sadly many of the newer treatments with better side-effect profiles are prohibitively expensive for the developing nations where KS is prevalent. In patients with relatively well preserved immune function interferon-α is a useful treatment.Bleomycin and vincristine in combination was initially the commonest regimen giving a response rate of 50—60% with acceptable side-effects. This has now largely been superseded by the liposomal preparations of doxorubicin and daunorubicin (anthracycline antibiotics) following trials which showed comparable efficacy and reduced toxicity. A liposome is a sphere made of phospholipid bilayers which can be selectively distributed to tumours allowing local drug deposition when the liposome breaks down. Liposomal packaging allows higher doses of these drugs to be delivered with fewer side-effects.

Figure 5.5 Kaposi’s sarcoma on the chest

Figure 5.6 Cutaneous Kaposi’s sarcoma

Figure 5.7 Palatal Kaposi’s sarcoma
Cumulative doses of non-liposomal anthracyclines are limited at 450-550mg∕m2 by cardiotoxicity and in a chronic condition like KS long or repeated courses of chemotherapy may be required.
More recently there has been increased interest in the use of antiangiogenics and trials are currently underway on the tyrosine kinase receptor inhibitor SU5416 and thalidomide. This has been fired by studies showing the presence of vascular endothelial growth factor and basic fibroblast growth factor in KS tissues. Paclitaxel, a newer cytotoxic, is also undergoing trials. Common side-effects are those shared with many other cytotoxics including nausea, vomiting, myelosuppression and mucositis. In the AIDS patient, with concomitant diseases and multidrug therapy including HAART, it can be difficult to find the root cause of such symptoms.
More on the topic Kaposi's sarcoma:
- Associated Neoplasms Kaposi Sarcoma
- Sarcoma
- Histiocytic Sarcoma
- Common HIV Therapies and the Heart
- Malignancies
- Box 1.1 Early history of the epidemic
- Cardiovascular Malignancy
- Cardiac Malignancy
- SKELETAL MALIGNANCIES
- Intracerebral, Subarachnoid Hemorrhages and Subdural Hematoma