Lipid
Hepatic intracytoplasmic lipid accumulation appears as clear cytoplasmic vacuoles with a distinct margin or punched out appearance (Figures 9.11a, b). The lack of staining is due to solubilized lipid being washed away during Romanowsky staining protocols.
This clear vacuolar material can often be seen in the background adjacent to ruptured hepatocytes. Oil red O or Sudan black stains can be used to confirm the presence of lipid, if needed.Although hepatocyte lipid vacuolation is easily identified with cytologic preparations, vacuolar lipid hepatopathy is not synonymous with hepatic lipidosis. The disease entity hepatic lipidosis is a set of systemic pathologic metabolic changes and not solely lipid accumulation. Lipid vacuolation is a common secondary change associated with many different pathologic processes. A case series of four cats with cytologically diagnosed vacuolar hepatopathy had a different diagnosis which eclipsed the lipid accumulation made by subsequent histology (lymphoma, inflammation, or cholestasis) (Willard et al., 1999). Ingestion of aflatoxin-contaminated commercial feed can cause hepatic failure and has been confirmed to cause lipid accumulation by histopathology and EM (Newman et al., 2007). When hepatic lipid vacuolation is encountered, any pathologic process that leads to lipid accumulation, including hepatic lipidosis, must remain on the differential list until excluded.
Glycogen/hydropic degeneration
Glycogen accumulation and hydropic degeneration associated with loss of water regulation are two vastly different processes. Cytologically, however, both are noted as a fine, often foamy and indistinct cytoplasmic rarefaction (Figures 9.12, 9.13). Although glycogen accumulation is commonly referred to as a vacuolar hepatopathy, because glycogen is free in the cytosol and not within a limiting membrane it is not technically within a vacuole.
The presence of glycogen can be confirmed with periodic acid–Schiff (PAS) staining which is abrogated by diastase digestion. Hepatocyte size is often markedly increased with a more rounded rather than polygonal shape. The background of the slide does not reveal the vacuolar material seen with lipid. Glycogen accumulation is more commonly seen in dogs than cats and is a fairly nondescript change. It is associated with altered glucose/glycogen metabolism, which is commonly caused by naturally occurring hyperadrenocorticism and iatrogenic glucocorticoid administration. Less frequently, insulinoma or other hormonal dysregulation can lead to hepatic glycogen accumulation (Goutal et al., 2012). Most liver aspirates from aged dogs will contain a minimal amount of glycogen accumulation, a finding that has an unknown significance. 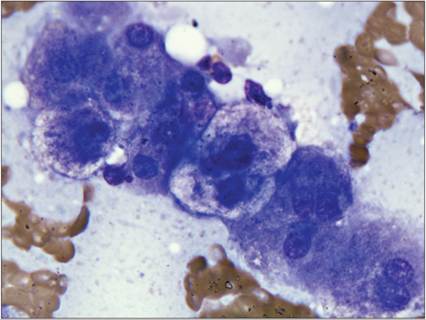
Figure 9.13 Contrast the cytoplasm of the center two hepatocytes with those flanking them. The center hepatocytes have foamy cytoplasmic rarefaction, consistent with glycogen or hydropic degeneration (Wright–Giemsa, 1,000? magnification).
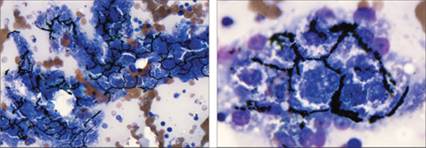
Marked cholestasis, noted as tubular accumulations of coarse green-black granular pigment, highlights the canalicular system normally present between hepatocytes
Figure 9.14 Wright–Giemsa, 500? magnification.
Figure 9.15 Wright–Giemsa, 1,000? magnification.
Hydropic degeneration is the result of loss of cellular control of free water, which leads to organelle swelling. Toxic injury, hypoxia, and metabolic or other insults have been associated with this ballooning degenerative process.
Pigmentary changes
Bile pigment
This green to blue to black coarse granular pigment is a normal product of the liver; however, visible quantities of bile pigment are suggestive of cholestasis.
Bile pigment may be observed as a fine cytoplasmic dusting or as smaller aggregates inside the hepatocytes with intrahepatic cholestasis. With extrahepatic cholestasis, bile pigment will be in larger aggregates and forming tubular casts within the biliary canaliculi (Figures 9.14, 9.15). Occasionally, bile pigment can be present in lamellated light-brown to amber globular crystals. Hall’s stain can be used to confirm the presence of bile (Figures 9.16a–d). 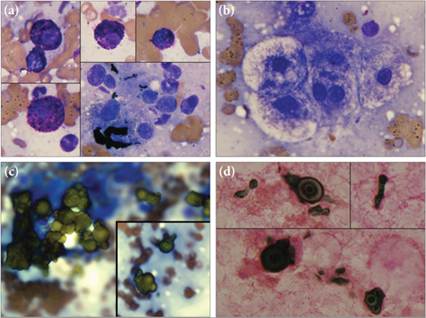
Figures 9.16a–d Liver aspirate from a dog with cutaneous mast cell tumors that had metastasized to multiple organs. (a) Dark green–black tubular structures (lower right panel), consistent with the more commonly seen form of bile casts are very rarely seen. Well-granulated mast cells make up just over 1% of the cellular population. Multiple individualized mast cells were imaged and included along the left and upper edge of the image to display the minimal to moderate anisocytosis and anisokaryosis in this population. With knowledge of the clinical history and multiple metastatic foci, this is consistent with mast cell tumor metastasis to the liver. (b) Most hepatocytes display moderate to marked cytoplasmic rarefaction, consistent with glycogen or hydropic degeneration. (c) Globular light brown to amber round, layered crystals are found. These are occasionally present within hepatocyte clusters (not shown). (d) The globular crystals displayed in 9.16c were positive with Hall’s stain, demonstrating that they are a rarely seen form of bile crystals and supporting the diagnosis of cholestasis (a–c, Wright–Giemsa, 1,000? magnification; d, Hall’s bilirubin stain).