Microbiology
Culture via standard microbiology techniques is rarely performed using lymph node aspirates and is generally limited to selected bacterial diseases. The main advantage is that these techniques can also provide data about antibiotic susceptibility, which is clinically useful.
Normal anatomy and cytology
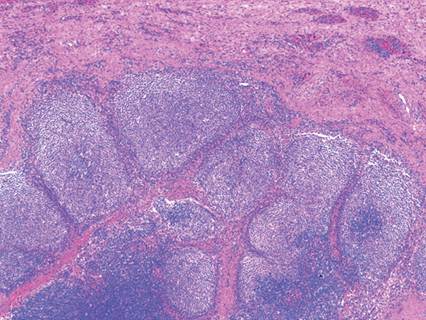
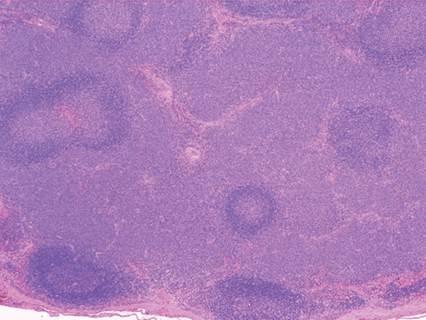
The lymph node parenchyma is surrounded by a connective tissue capsule extending inwards in fibrous septae. Subcapsular sinuses drain lymph from the periphery into the cortical sinuses and sinusoids. The cortex of a lymph node is formed by primary and secondary follicles. Primary follicles are mainly composed of small, resting B lymphocytes. The secondary follicles develop after antigenic stimulation (Figure 5.4). In histologic sections of lymph nodes, areas of B lymphocyte development can be identified by a central, pale-staining area, representing the germinal center where differentiation occurs, and a thin peripheral rim of more intensely basophilic cells where clonal expansion occurs. Low numbers of macrophages and dendritic cells are also present in germinal centers. The germinal center is surrounded by a dark layer of small B memory cells with clumped chromatin called the mantle cell zone. In the dog, there is a thin layer of light colored, medium-sized macronucleolated cells around the follicles termed the marginal zone. The paracortex is the interfollicular tissue and is composed mainly of small T lymphocytes, rare T immunoblasts, interdigitating cells, and macrophages. Lastly, the medullary cords are comprised mainly of plasma cells, mature lymphocytes, and macrophages, which are adjacent to sinus spaces.
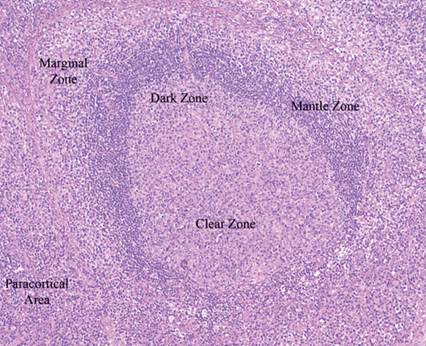
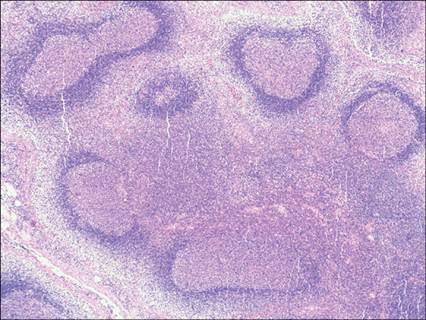
Figure 5.4 Dog, peripheral lymph node, histology. A secondary follicle with central germinal center (clear and dark zone) surrounded by an inner rim of mantle cells and an outer rim called the marginal zone (H&E, 100? magnification) (courtesy L.
Aresu).
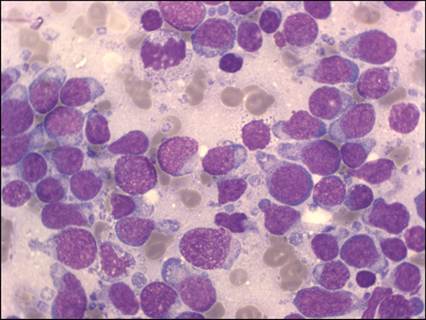
The main cytologic appearances of the different cells present in normal lymph node aspirates are described in Figure 5.5 and Table 5.2. Although these cell types can be identified, it is the ratio of small, intermediate, and large lymphocytes that is most important to assess cytologically. In a normal lymph node aspirate, approximately 80% of cells are small lymphocytes, 15% are intermediate-sized lymphocytes, and 5% are large lymphocytes. Small percentages of other cell types (plasma cells, macrophages/histiocytes, neutrophils, mast cells, and eosinophils) also may be observed in normal lymphoid tissue. Phagocytized cellular remains are often seen in the cytoplasm of lymph node macrophages (also named tingible body macrophages). Interspersed among the cells, a moderate number of small, round, gray–blue cytoplasmic fragments (lymphoglandular bodies) are normally recognized in cytologic smears. They may increase if cellular fragility is increased, particularly in lymphoma cases, but also in non-neoplastic conditions.
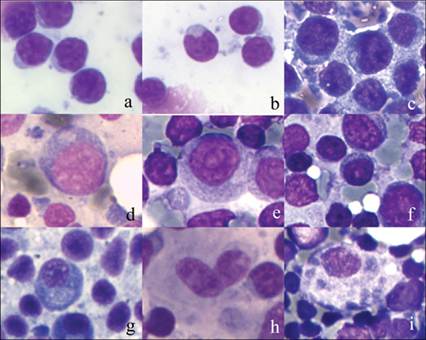
Figure 5.5 Dog, peripheral lymph node, FNA. Cell populations that may be found in a normal lymph node. a, small lymphocytes; b, centrocytes; c, lymphoblast; d, centroblast; e, immunoblast; f, medium-sized macronucleolated cells (marginal zone); g, plasma cells; h, interdigitating cells; i, macrophage with tingible bodies. See text for description (May–Grünwald–Giemsa, 1,000? magnification).
Table 5.2 Subtypes of cells that may be identified in cytologically normal canine lymph node samples
| Cell subtype | % expected | Cytologic description | Origin | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Small lymphocytes | >80% | Small lymphocytes; nuclear diameter 7–10 μm; scarce rim of basophilic cytoplasm; round or slightly indented nucleus; clumped chromatin; no visible nucleolus | B or T lymphocytes | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Centrocytes | 5–10% | Small to intermediate-sized lymphocytes; nuclear diameter 10–14 μm; moderate amount of clear cytoplasm; cleaved nucleus; dense, unclumped chromatin; no visible nucleolus | Follicular B cells | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Centroblasts | 1–5% | Intermediate to large lymphocytes; nuclear diameter 14–21 μm; moderate amount of deeply basophilic cytoplasm; occasional cytoplasmic vacuoles; eccentric, round nucleus; decondensed, finely stippled chromatin; multiple, often peripheral, nucleoli | Follicular B cells | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Immunoblasts | 1–5% | Large lymphocytes; nuclear diameter up to 28 μm; abundant, deeply basophilic cytoplasm; occasional cytoplasmic vacuoles; round nucleus; finely stippled chromatin; one central prominent nucleolus | B or T lymphocytes | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
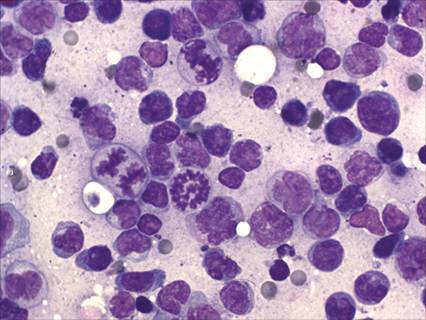
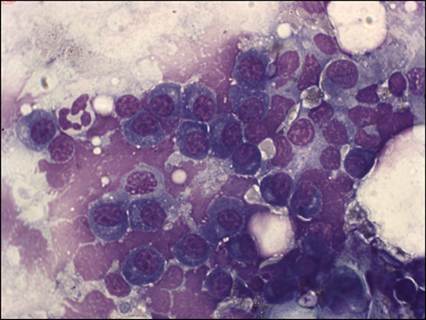
| Lymphoblasts | 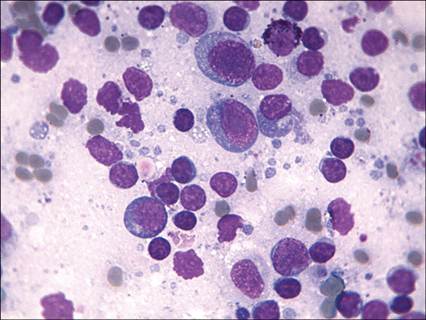 Figure 5.6 Cat, enlarged subcutaneous lymph node, FNA. Follicular hyperplasia. An admixed population of small lymphocytes, large blast cells, a plasma cell, and a mast cell. The presence of a continuum of lymphoid cells at different maturation stages and some plasma cells may help to differentiate follicular hyperplasia from an early phase of follicular lymphoma (May–Grünwald–Giemsa, 1,000? magnification).
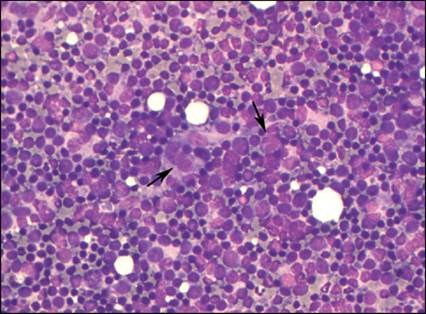
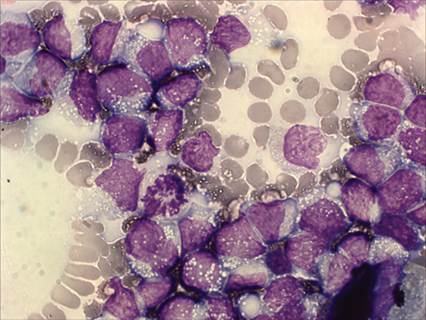
Figure 5.7 Dog, enlarged peripheral lymph node, FNA. Paracortical hyperplasia. Two large interdigitating cells (arrows) in a mixed lymphoid population are evident (May–Grünwald–Giemsa, 400? magnification).
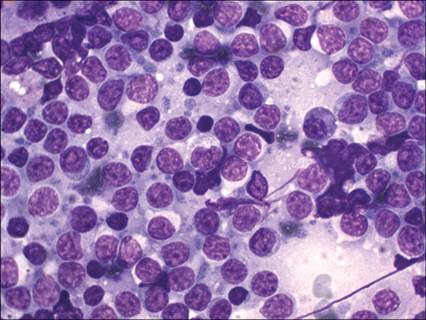
Figure 5.8 Dog, enlarged peripheral lymph node, FNA. Paracortical hyperplasia. A mixed population of lymphoid cells at different maturation stages and one interdigitating cell. Three ‘hand-mirror’-shaped cells, likely of T cell origin, are indicated by the arrows (May–Grünwald–Giemsa, 1,000? magnification).
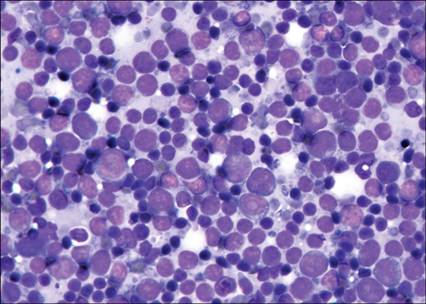
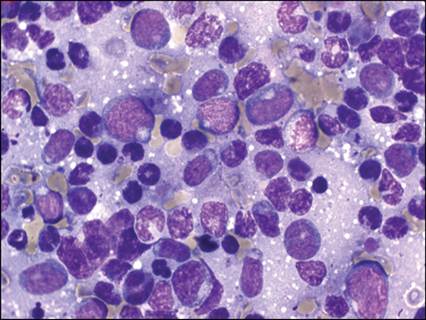
Figure 5.9 Cat, peripheral lymph node, FNB. Atypical lymphoid hyperplasia (distinctive peripheral lymph node hyperplasia). Increase of large blast cells mimicking lymphoma and residual small lymphocytes (May–Grünwald–Giemsa, 600 ? magnification).
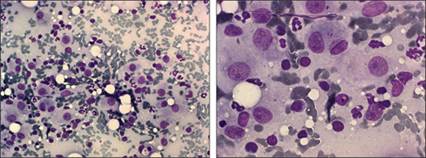
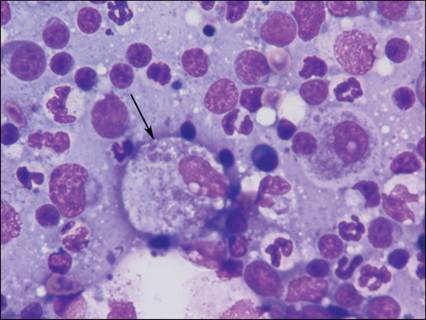
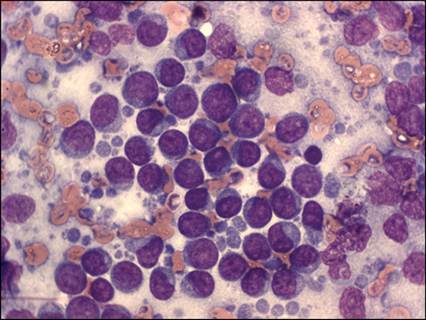
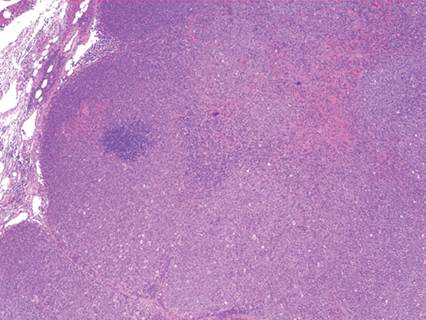
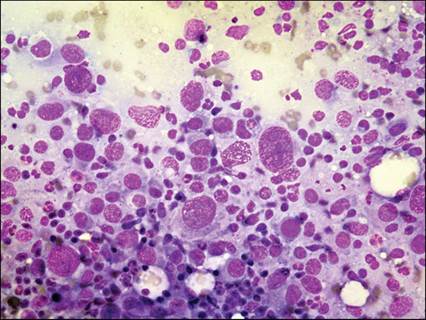
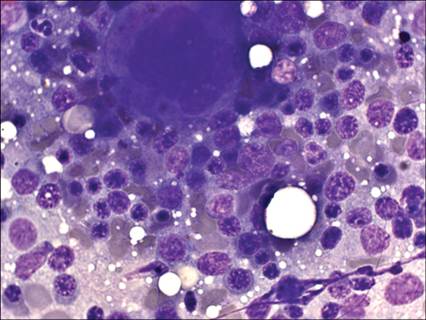
Lymphoid reactivity Lymphoid reactivity is a common cause of lymphadenopathy. Histologically, there is an expansion of secondary follicles with increased numbers of plasma cells (Figure 5.10). Cytology samples from reactive lymph nodes are predominated by small lymphocytes, with mildly increased numbers of intermediate-sized lymphocytes and lymphoblasts, and increased numbers of plasma cells (>2% of the overall cell population) (Figures 5.11, 5.12). There may also be increased macrophages with tingible bodies. Plasma cell hyperplasia linked to cutaneous diseases with scaling and skin damage may be classified as dermatopathic lymphadenopathy (Figure 5.13). Dermatopathic lymphadenopathy is further characterized by several macrophages and abundant brown–black pigment (melanin granules) phagocytized by macrophages or scattered in the background. Scattered eosinophils, neutrophils, and mast cells also may be present. Figure 5.10 Dog, peripheral lymph node, histology. Reactive hyperplasia. Follicles are characterized by expansion of germinal centers, uniform mantle zones, and a well-defined marginal zone hyperplasia (H&E, 50? magnification) (courtesy L. Aresu).
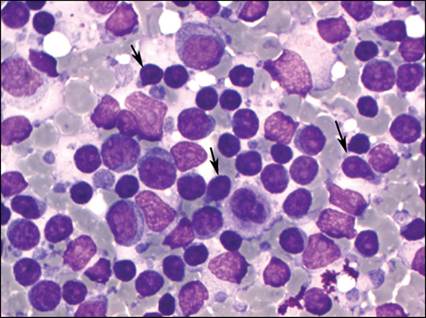
Figures 5.11,5.12 Dog, peripheral lymph node, FNA. Plasma cell hyperplasia. Increased numbers of plasma cells are admixed with lymphocytes. A Mott cell with large clear vacuoles (Russell bodies) is indicated by the arrow (May–Grünwald–Giemsa, 1,000? magnification).
Figure 5.13 Dog, axillary lymph node, FNA. Dermatopathic lymphadenopathy. In the context of a plasma cell hyperplasia, small black melanin granules are found free in the background or phagocytized by macrophages. This feature is suggestive of the retention of melanin pigment from a cutaneous lesion (May–Grünwald–Giemsa, 1,000? magnification).
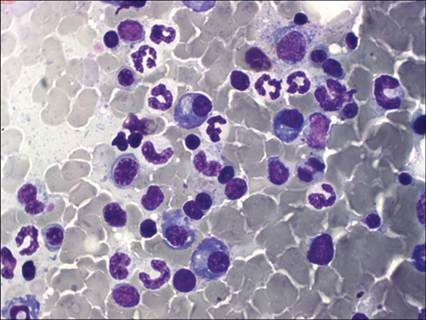
If plasma cell hyperplasia is severe, plasma cell neoplasms should be considered as a differential. Typically, neoplastic plasma cells will have characteristics of malignancy, including bi- and multinucleation, marked anisocytosis and anisokaryosis, and immature chromatin patterns. Ancillary tests, such as serum protein electrophoresis and radiographic screening for bony lysis, may be useful to differentiate between marked lymphoid reactivity and plasma cell neoplasms. Lymphadenitis Lymphadenitis is characterized by a conspicuous number of inflammatory cells, although the lymphoid population is generally prevalent, and may be associated with some degree of lymphoid hyperplasia or reactivity. Three different lymphadenitis types are defined according to the main characteristic inflammatory population. Neutrophilic lymphadenitis Suppurative (purulent) lymphadenitis is diagnosed when more than 5% of cells in the sample are neutrophils, which may be degenerate and/or contain bacteria (Figure 5.14). Occasionally, the lymphoid population is almost completely substituted by neutrophils. Bacterial infections are the most common cause, but neoplastic or immune-mediated diseases may lead to such a feature. In severe cases, necrosis may be present. As the disease process becomes more chronic, increased numbers of macrophages will infiltrate the lymph node and a diagnosis of pyogranulomatous lymphadenitis should be made. Chronic bacterial and fungal infections are commonly associated with the development of pyogranulomatous lymphadenitis. Figure 5.14 Dog, mandibular lymph node, FNA. Neutrophilic lymphadenitis. Numerous mildly degenerated neutrophil granulocytes in a background of residual lymph node (May–Grünwald–Giemsa, 600? magnification).
Eosinophilic lymphadenitis In cases of eosinophilic lymphadenitis, more than 3% of cells are eosinophils (Figure 5.15). Diseases associated with eosinophilic lymphadenitis include parasitic infections (endoparasites or ectoparasites), hypersensitivity reactions (particularly allergic dermatitis), and paraneoplastic inflammation. Feline eosinophilic granuloma complex or hypereosinophilic syndrome could also cause eosinophilic lymphadenitis. Peripheral blood should be evaluated to rule out the possibility that the eosinophils in the aspirate are a component of blood contamination, rather than an infiltrating cell population in the lymphoid tissue. Figure 5.15 Cat, peripheral lymph node, FNA. Eosinophilic lymphadenitis. Several eosinophils are evident in a background of resident lymphoid cells. Neutrophils and a plasma cell are also present (May–Grünwald–Giemsa, 1,000? magnification).
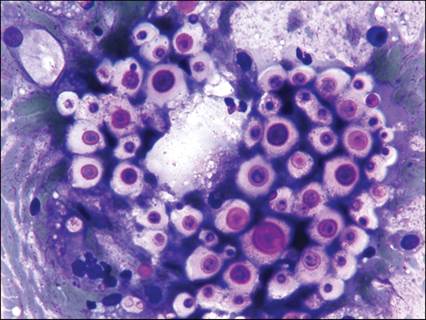
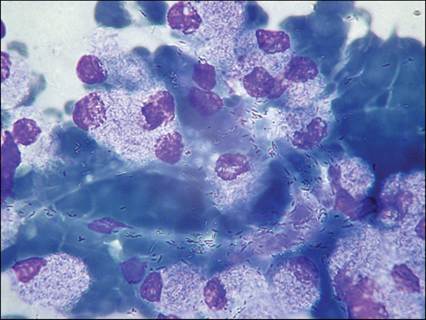
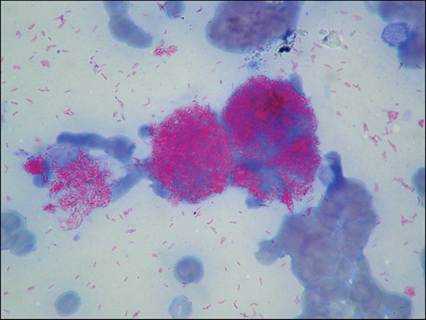
Granulomatous lymphadenitis Granulomatous lymphadenitis is characterized by an increased number (>3%) of histiocytic cells or macrophages (Figures 5.16, 5.17). Epithelioid macrophages or multinucleated giant cells may also be present. In some cases, the causative agent may be detected. Systemic fungal infections, including aspergillosis (Figure 5.18), blastomycosis (Figure 5.19), cryptococcosis (Figures 5.20, 5.21), histoplasmosis (Figure 5.22), coccidioidomycosis, mycobacteriosis (Figure 5.23), salmon fluke poisoning disease (Neorickettsia helminthoeca; Figure 5.24), protothecosis (Figure 5.25), cytauxzoonosis (Figure 5.26), and toxoplasmosis (Figure 5.27) may be accompanied by granulomatous or pyogranulomatous lymphadenitis. Leishmaniosis may also lead to granulomatous or pyogranulomatous lymphadenitis and concurrent plasma cell hyperplasia is commonly seen (Figure 5.28). Organisms may be identifiable by standard stain or may appear as negative impressions in the cytoplasm of phagocytes, as with Mycobacterium spp. (Figure 5.23). Cytological diagnosis of certain organisms may be improved using special stains such as Ziehl–Neelsen for Mycobacterium spp. (Figure 5.29), periodic acid–Shiff or silver stains for fungi and Prototheca spp., and ink stain for Cryptococcus spp. Figures 5.16,5.17 Cat, intestinal lymph node, FNA. Granulomatous lymphadenitis. (5.16) Several large epithelioid macrophages and some neutrophils are found among lymphoid cells (May–Grünwald–Giemsa, 400? magnification). (5.17) Particularly large epithelioid cells and a binucleated cell (May–Grünwald–Giemsa, 1,000? magnification).
Figure 5.18 Dog, peripheral lymph node, FNA. Aspergillosis. A septated hypha is indicated by the arrow (May–Grünwald–Giemsa, 1,000? magnification) (courtesy U. Bonfanti).
Figure 5.19 Dog, peripheral lymph node, FNA. Blastomycosis. Yeast structures (arrows) are surrounded by a pyogranulomatous inflammation (Wright–Giemsa, 1,000? magnification). Inset: a budding yeast is recognizable at high magnification (Wright–Giemsa, approximately 3,000? magnification) (courtesy A. Barger).
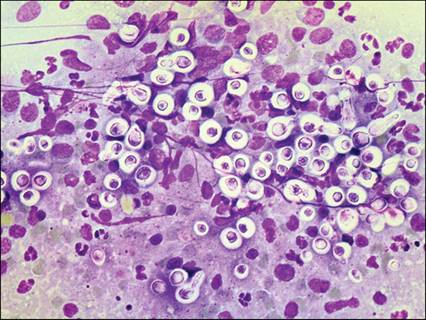
Figure 5.20 Dog, lymph node, FNA. Cryptococcosis. Several yeast forms surrounded by a thick clear halo representing the capsule, in a background of necrotic debris (May–Grünwald–Giemsa, 1,000? magnification) (courtesy U. Bonfanti).
Figure 5.21 Dog, peripheral lymph node, FNA. Cryptococcosis. An islet of pleomorphic yeasts at different maturation stages and occasionally showing budding (Wright–Giemsa, 1,000? magnification) (courtesy A. Barger).
Figure 5.22 Dog, peripheral lymph node, FNA. Histoplasmosis. Numerous yeast forms are found in the macrophages or in the background (Wright–Giemsa, 1,000? magnification) (courtesy A. Barger).
Figure 5.23 Cat, peripheral lymph node, FNA. Mycobacteriosis. Several negatively stained rods are found in the macrophages, and more rarely, free in the background (May–Grünwald–Giemsa, 1,000? magnification) (courtesy W. Bertazzolo).
Figure 5.24 Dog, peripheral lymph node, FNA. Salmon fluke poisoning disease. Several small gray to pink granules (arrow), referable to Neorickettsia helminthoeca within macrophages, in a background of a pyogranulomatous lymphadenitis (Wright–Giemsa, 1,000? magnification) (courtesy A. Barger).
Figure 5.25 Dog, intestinal lymph node, FNA. Protothecosis. Two oval structures with thin clear walls, referable to endospores of Prototheca (arrow), are identifiable in the background of a necrotic lymph node (May–Grünwald–Giemsa, 1,000? magnification) (courtesy C. Masserdotti).
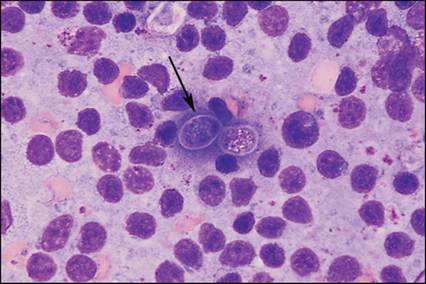
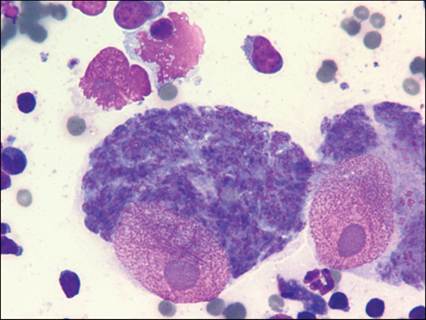
Figure 5.26 Cat, peripheral lymph node, FNA. Cytauxzoonosis. Two large schizonts engulfing mononuclear phagocytes. The schizonts are composed of several small merozoites (small piroplasms), which are released with the rupture of the schizont and represent the infective form for the erythrocytes (Wright–Giemsa, 1,000? magnification) (courtesy A. Barger).
Figure 5.27 Cat, peripheral lymph node, FNA. Toxoplasmosis. Macrophage containing several ‘banana-shaped’ tachyzoites (arrow) in a necrotic background (May–Grünwald–Giemsa, 1,000? magnification) (courtesy C. Masserdotti).
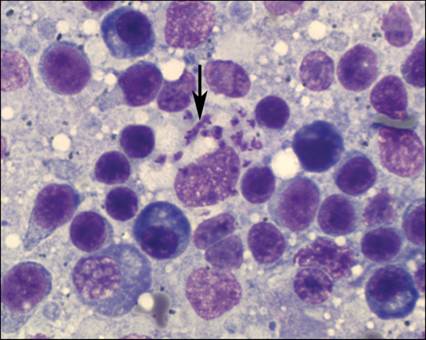
Figure 5.28 Dog, peripheral lymph node, FNA. Leishmaniosis. Several Leishmania amastigotes (arrow) in the cytoplasm of a macrophage in the context of a plasma cell hyperplastic lymph node. Note the mixed population composed of plasma cells, small lymphocytes, and hand-mirror-shaped T-lymphoid cells (May–Grünwald–Giemsa, 2,000? magnification).
Figure 5.29 Same case as Figure 5.23. Mycobacteriosis. The free and intracellular rods stain intensely with Ziehl–Neelsen, supporting acid resistance (courtesy W. Bertazzolo).
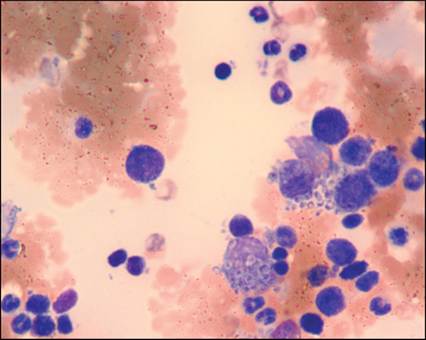
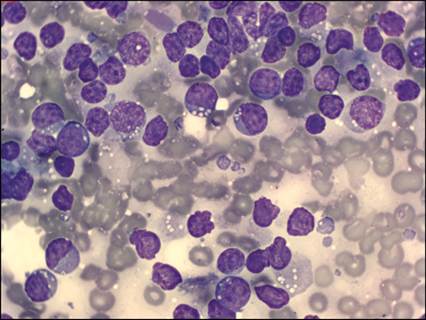
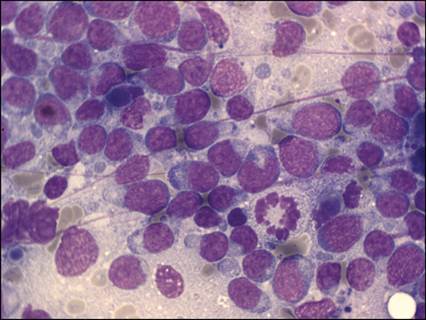
Extramedullary hematopoiesis Extramedullary hematopoiesis (EMH, myeloid metaplasia) limited to one hematopoietic lineage or to a mixture of erythroid, myeloid, and megakaryocytic lineages may occur within lymphoid tissues. Strong regeneration due to hemolytic anemia, leukemoid reactions, or megakaryocytic hyperplasia may induce EMH. Immature hematopoietic cells at all stages of maturation may be identified and are often associated with plasma cell hyperplasia. The presence of hematopoietic precursors in multiple stages of maturation enables cytologists to differentiate EMH from infiltration of acute myeloid leukemia (AML). In AML, the majority of myeloid cells are myeloblasts. If myeloblasts are the predominant non-lymphoid cell in the sample, cytologic evaluation of a peripheral blood smear and a bone marrow aspirate is recommended. Lymphoma Lymphoma (previously also called ‘lymphosarcoma’ or ‘malignant lymphoma’) occurs in approximately 20 out of 100,000 dogs and accounts for 50–90% of hematopoietic neoplasms in cats, but the overall incidence of lymphoma in cats is unknown (Vail, 2013). The etiology of lymphoma is likely multifactorial (environmental exposure to carcinogens, immunologic causes, genetic factors). In cats retroviral infections (FeLV and FIV) and passive exposure to tobacco smoking have been demonstrated as possible predisposing factors. Genetic factors are thought to include germline and somatic mutations, altered oncogene and tumor suppressor gene expression, epigenetic changes, and disrupted signal transduction and apoptosis pathways (Thomas et al., 2001). The role of cytology in the diagnosis of canine lymphoma has been considered crucial due to: (1) the high prevalence of diffuse, overtly nodular lymphomas in dogs, thus increasing the accuracy of cytologic aspiration; (2) the minimal invasiveness of cytologic sampling compared with histologic biopsies, that encourages owner compliance; and (3) the limited use of subtype-specific therapeutic protocols, which discourages the use of invasive techniques in the diagnostic work up. On the other hand, the role of cytology in feline lymphoma is more challenging since: (1) feline lymphomas are often limited to internal organs or lymph nodes, thus sampling may be difficult and often requires sedation; (2) lymphoma classification schemes used in dogs are not easily applicable to cats; and (3) the presence of lymphoma subtypes composed of small lymphocytes and of hyperplastic conditions that strongly resemble lymphoma. In a survey among veterinarians (Regan et al., 2013), the use of cytology in the diagnostic algorithm for lymphoma widely exceeded that of histologic biopsy (88% versus 28%). In the authors’ opinion, cytology plays a central role in the diagnostic approach to canine lymphadenopathy since it allows veterinarians to easily differentiate lymphoid reactivity from lymphoma in the great majority of cases. In a recent study, cytology had a 92.6% sensitivity and 89.4% specificity in distinguishing lymphoma vs. non-lymphoma in dogs (Martini et al., 2021). The immunophenotype of the lymphoma can also be determined from a cytologic sample if flow cytometry or ICC is added (Comazzi & Gelain, 2011). However, cytology alone shows variable diagnostic performances in immunophenotyping and grading, ranging from more than 80% sensitivity and 95% specificity for low-grade T-cell lymphoma to less than 20% sensitivity for low-grade B-cell lymphoma and about 60% specificity for high-grade B-cell lymphoma (Martini et al, 2022). Immunophenotyping via flow cytometry or immunocytochemistry likely improve these performances but histology and immunohistochemistry of a whole lymph node are suggested to definitively diagnose subtype and grade or to solve differentials in selected, challenging cases. Cytological criteria used in dogs to predict immunophenotyping are not useful in immunophenotyping feline nodal lymphoma (Gambini et al., 2021). Classification of lymphoma Classification of lymphomas has been widely revised during the last 50 years both in human and in veterinary medicine. Until recently, the most suitable classification schemes were the modified Kiel classification (Fournel-Fleury et al., 1997), which is based on morphologic abnormalities in lymphoid cells and was partially linked to specific biological behavior of lymphomas in dogs (Ponce et al., 2004), and the World Health Organization (WHO) classification (Valli et al, 2011), which is focused on histopathology and immunophenotype. Some attempts to identify correlations among the two different classification schemes have been made (Ponce et al., 2010; Table 5.4), but we are still far from a definitive classification scheme. The ability to predict WHO classification subtype via cytology alone has been evaluated in a recent study (Martini et al., 2022) and results showed variable accuracy depending on the subtype with the higher in T zone lymphoma and the lower in peripheral T-cell lymphoma (PTCL). The main diagnostic issues were differentiation among B-cell lymphoma subtypes and overestimation of PTCL with inclusion of many B-cell lymphoma subtypes. Addition of immunophenotyping via flow cytometry likely increases the accuracy of cytological diagnosis but research on this aspect is still ongoing. More recently, gene expression profile analysis was used to group specific morphologic subtypes into three different entities, which may have prognostic relevance in canine lymphomas (Frantz et al., 2013); however, additional studies are needed to confirm these results. Table 5.4 Classifications and cytologic descriptions of lymphomas in dogs and cats
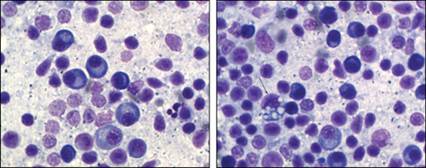
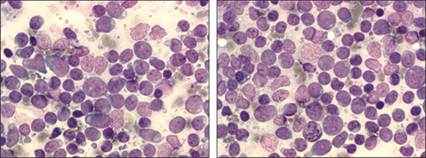
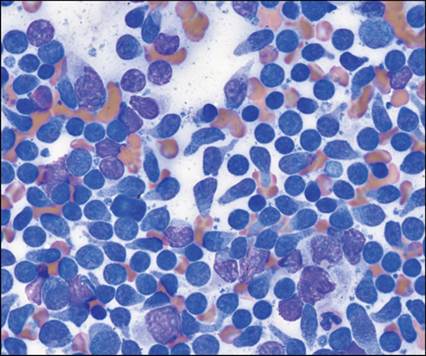
Figure 5.40 A mixed population of small cells and pleomorphic medium/large blasts with moderately abundant, mildly basophilic cytoplasm, indented to convoluted nuclei with smooth chromatin and rare nucleoli.Figure 5.41 High-grade T-cell lymphoma, pleomorphic mixed small and large. Note the mixed population of cells and the presence of occasional plasma cells.
New diagnostic techniques have identified new subtypes of lymphoma, but in order for classification schemes to be clinically relevant, they need to reflect biological behavior, median survival times, and response to tailored therapy. Recently, a WHO subtype has been described as an aggressive B-cell lymphoma and provisionally named diffuse small B-cell lymphoma, (DSBCL, Hughes et al, 2021). This entity is characterized by small cells, with scarce cytoplasm, round nuclei with condensed chromatin and indistinct nucleoli but a high number of mitosis are present. Flow cytometry confirms a prevalence of B cells with low forward scatter properties (suggesting small size). Further studies are still needed to define and validate the diagnostic approach for DSBCL and to identify potential prognostic factors. Currently, cytologic evaluation is a very powerful tool to diagnose lymphoma, but often is insufficient for further characterization of the disease. Immunophenotyping is highly recommended and additional diagnostics, including histologic subtyping, are needed to predict clinical outcomes. Diagnostic staging of lymphoma relies heavily on localization of the neoplastic cells and clinical signs of disease. The WHO guideline for clinical staging of lymphoma in domestic animals is summarized in Table 5.5 (Owen, 1980). In dogs, prognostic factors with a strong association with response to chemotherapy and/or survival include: (1) location of the lymphoid neoplasm; (2) clinical stage; (3) WHO substage; (4) histologic grade; and (5) immunophenotype. For example, a poor prognosis is warranted for patients with mediastinal lymphomas, high-grade B-cell lymphomas with bone marrow infiltration (Marconato et al., 2013b), WHO substage b classification, high-grade T-cell tumors, B-cell tumors with low expression of major histocompatibility complex (MHC) class II or of CD21 (Rout et al. 2020) or high expression of CD25 by flow cytometry or high percentage of Ki67 positive cells, and lymphoma patients with concurrent non-regenerative anemia. Histology may provide information about treatment response as well as overall prognosis. For example, patients with high-grade lymphomas tend to have a better initial response to therapy but have worse median survival times, whereas patients with indolent lymphomas have prolonged survival times. More than 80% of dogs present with stage III or IV lymphoma (Vail et al., 2013). Most cats present with low-grade T-cell lymphomas of the alimentary tract, which generally have a good prognosis (Vail, 2013). Table 5.5 World Health Organization clinical staging of lymphomas in dogs and cats
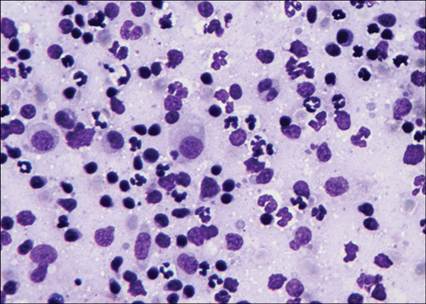
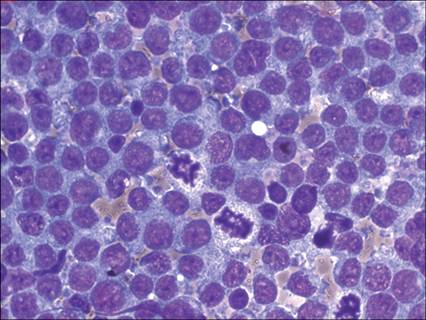
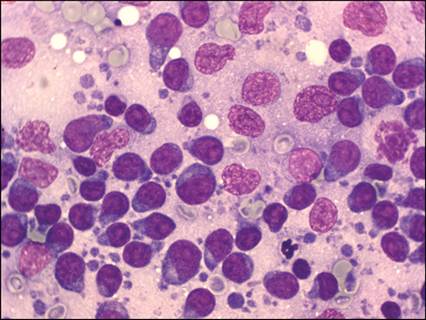
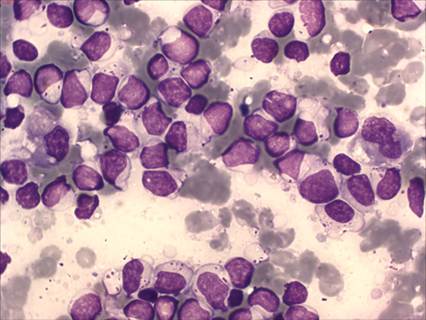
Cytological criteria for diagnosis of lymphoma Lymphoma should be a differential diagnosis in dogs with generalized peripheral lymphadenopathy (84% of canine cases are multicentric lymphomas) and in cats with signs of gastrointestinal disease or an enlarged internal lymph node (Vail et al., 2013). In most cases of canine lymphoma, the disease is easily diagnosed by cytologic samples that contain a high percentage (often >50%) of large lymphoid cells with a nuclear diameter >15 micrometers (larger than a neutrophil) and one or more prominent nucleoli. Nucleoli are very distinctive in hematopoietic cells, including lymphoid cells, and appear as a ring of clumped chromatin around a central, clear area. Mitosis, also atypical, may be present and suggestive of high grade (Figure 5.48) but mitotic index may be quite variable among different histotypes. Lower numbers of small and intermediate-sized lymphocytes can be present. Plasma cells and inflammatory leukocytes should be rare. In cases where 30–50% of lymphoid cells are large lymphocytes and plasma cells are virtually absent, lymphoma is likely. Lymphomas comprised of small -or intermediate-sized lymphocytes are generally more difficult to definitively diagnose cytologically. If nearly all the cells in a sample are small or intermediate-sized and have a uniform morphology, lymphoma should be suspected and additional diagnostics recommended. Figure 5.48 Cat, peripheral lymph node, FNA. High-grade lymphoma. Prevalent population of pleomorphic large cells with indented to convoluted nuclei. Several mitotic figures, also atypical, are found (May–Grünwald–Giemsa, 1,000? magnification).
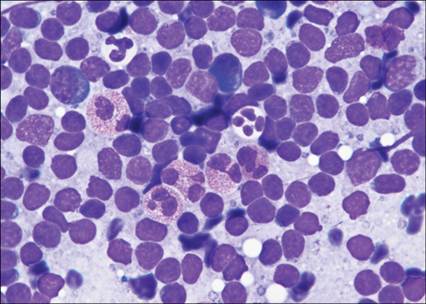
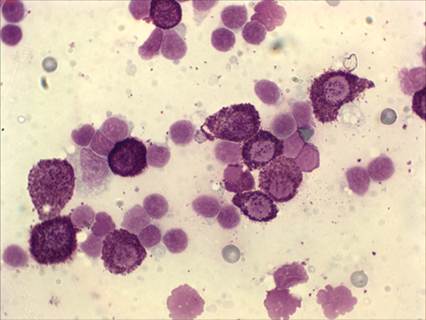
Lymphoma subtypes with distinctive cytologic morphology Large granular lymphocyte lymphoma Large granular lymphocyte (LGL) lymphoma is a specific lymphoma subtype that may be observed in cats, mainly in alimentary lymphoma, and occasionally occurs in dogs, often with splenic or hepatic involvement. In cats with LGL lymphoma, response to therapy and survival are generally very poor; median survival time is approximately 1.5 months (Krick et al., 2008; Moore et al., 2012). However, a recent paper reported a small percentage (about 7%) of cats having LGL lymphoma with long survival (Finotello et al., 2018). In dogs, prognosis varies with the degree of organ and bone marrow involvement. Most neoplastic LGL lymphomas exhibit a cytotoxic T-cell immunophenotype (CD3+CD8+) and are often positive for the aβ-T-cell receptor. More rarely, a natural killer cell phenotype (CD3−) is diagnosed (McDonough & Moore, 2000; Roccabianca et al., 2006). Note that canine patients with chronic lymphoid leukemias often have circulating granular lymphocytes (Tasca et al., 2009), but this disease process is not equivalent to LGL lymphoma and does not carry the same prognosis (Workman & Vernau, 2003). Cytology is characterized by medium-sized lymphoid cells with moderately abundant gray or light blue cytoplasm containing azurophilic magenta granules, often located in a perinuclear area. The granule size may vary from pinpoint to >2 micrometers in diameter (Figure 5.46) and may be surrounded by a clear halo in the cat (Figure 5.47). The nucleus is round to indented and may be condensed without visible nucleoli (in more differentiated forms) or smooth with prominent nucleoli in less differentiated tumors. Care must be taken to distinguish LGL lymphoma from poorly granulated mast cell tumors, in which granules are often homogeneously distributed throughout the cytoplasm. Figure 5.46 Dog, peripheral lymph node, FNA. Large granular lymphocyte lymphoma. Prevalent population of medium-sized cells with clear cytoplasm and variable azurophilic cytoplasmic granules (May–Grünwald–Giemsa, 1,000? magnification).
Figure 5.47 Cat, intestinal lymph node, FNA. Large granular lymphocyte lymphoma. Neoplastic cells often contain large azurophilic granules surrounded by a clear halo, resembling a capsule (May–Grünwald–Giemsa, 1,000? magnification).
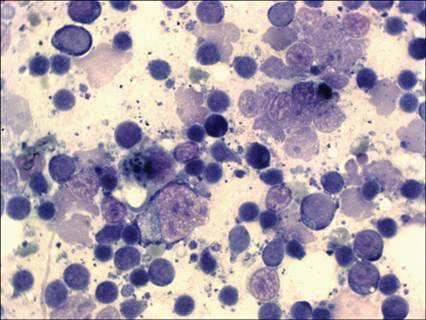
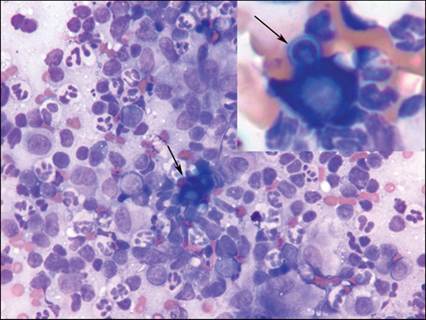
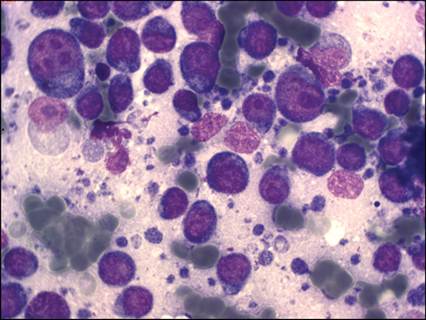
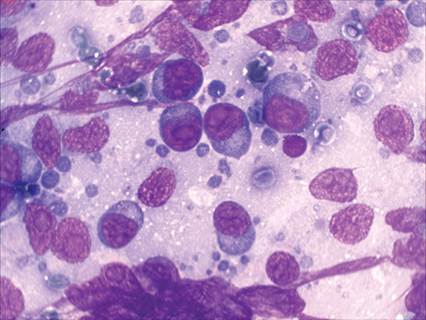
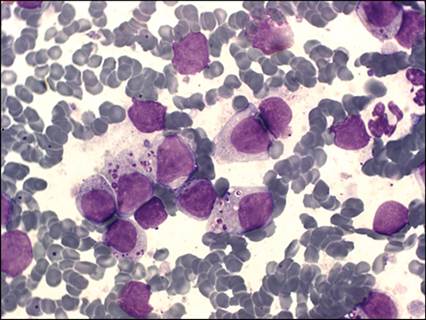
Hodgkin-like lymphoma Hodgkin-like lymphoma is a rare lymphoma subtype occasionally reported in the cat (Valli, 2007; Steinberg & Keating, 2008). This disease generally involves one or a few lymph nodes, mainly in the head or neck region, and is considered an indolent disease with survival times of 1 year or more (Vail, 2013). Cytology shows a very heterogeneous population of cells predominated by small lymphocytes or cells with a plasmacytoid appearance. Large macrophages containing cellular debris are frequent. Immunophenotyping shows a prevalent population of small reactive T cells, although the neoplastic population is assumed to be of B cell origin (T-cell rich, large B-cell lymphoma). Occasionally, some Reed–Sternberg cells (popcorn-like cells) may be found. These are large cells with pale cytoplasm, often binucleated with round to ovoid nuclei and prominent large nucleoli (Figures 5.49, 5.50) and may have a histiocytoid appearance, although Reed–Sternberg cells generally are negative for both B- and T-cell markers (CD79a and CD3, respectively) as well as for dendritic and macrophage markers. These cells are quite distinctive and strongly suggest Hodgkin-like lymphoma, although they are not pathognomonic and histopathology plus immunohistochemistry is mandatory to confirm the diagnosis. Figure 5.49 A large histiocytoid binucleated cell (Reed–Sternberg cell, arrow) is evident in the background of small lymphocytes (May–Grünwald–Giemsa, 400? magnification).Figure 5.50 The Reed–Sternberg cell at higher magnification (May–Grünwald–Giemsa, 1,000? magnification).
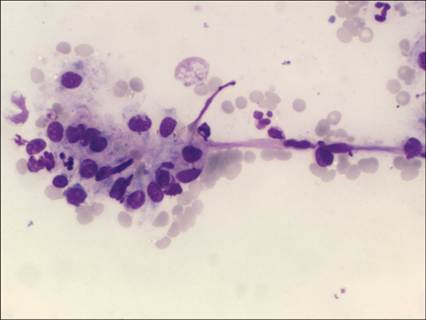
T-zone lymphoma T-zone lymphoma is an indolent lymphoma subtype reported in dogs (Valli et al., 2013). T-zone lymphomas often arise in mandibular lymph nodes and are definitively diagnosed using immunohistochemistry to identify a neoplastic population of CD3+ cells expanding the paracortical zones of a lymph node. In most cases of T-zone lymphoma, the neoplastic cells are negative for CD45 (Seelig et al., 2014; Martini et al., 2015; Stein et al., 2021; Kojima et al., 2022). Cytologically, neoplastic lymphocytes associated with T-zone lymphomas often have a ‘hand-mirror’ or ‘tadpole’ appearance (Valli et al., 2013). The lymphocytes are intermediate-sized with a moderate amount of basophilic cytoplasm that extends away from a round nucleus. The nuclear chromatin is commonly smooth to finely stippled. The extensions of cytoplasm are wide close to the nucleus and taper slightly further away from the nucleus. Unlike samples where cell morphology is artificially altered by a poor smearing technique, ‘hand-mirror’ lymphocytes have cytoplasm that extends away from the nucleus in random directions, relative to each other, on the slide (Figure 5.45). If this cytologic morphology is observed, additional diagnostics (e.g. flow cytometric or immunohistochemical analyses) are recommended to determine if the atypical lymphocytes are CD3+CD45– cells. If this is the case, an indolent T-zone lymphoma is likely. Figure 5.45 Dog, mandibular lymph node, FNA. Possible T-zone lymphoma. There is a marked expansion of intermediate-sized lymphocytes that often have ‘hand-mirror’ morphology (Wright–Giemsa, 1,000? magnification).
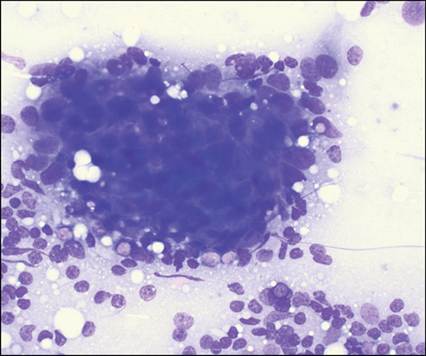
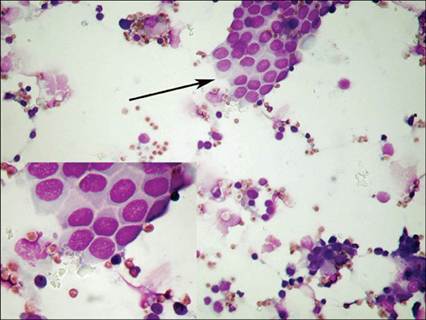
Metastatic neoplasia Metastatic disease is suspected if atypical cells are detected in cytologic smears of lymph node aspirates. Suspected neoplastic cells should be carefully evaluated for features of malignancy to ensure the cells have not simply been aspirated from tissue located close to the lymph node. Lymph nodes affected by metastatic diseases often show concurrent hyperplasia. When superimposed lymph node hyperplasia is present, a benign, mixed lymphoid population is observed with increased numbers of reactive plasma cells and/or macrophages. Lymph node cytology has high specificity but low sensitivity for metastatic disease due to the small sample size of a cytology aspirate; false-negative results occur if neoplastic cells are not aspirated. Histology and immunohistochemistry should be performed before excluding lymph node metastasis. Epithelial tumors metastasize to regional lymph nodes relatively frequently. Detection of neoplastic cells in lymph nodes is not rare with adenocarcinomas (Figure 5.51) and squamous cell carcinomas (Figure 5.52), and this finding affects prognosis. Neoplastic cells may be observed individually or in small clusters and they are easily distinguishable from the lymphoid population due to the large size and the morphologic appearance of the neoplastic cells. However, neoplastic cells from anaplastic carcinomas may metastasize singularly and are more difficult to differentiate from large lymphoid blasts or reactive macrophages. Figure 5.51 Dog, prescapular lymph node, FNA. A large cluster of epithelial cells is found among several small lymphocytes. Fewer intermediate and large lymphocytes as well as mildly increased numbers of plasma cells were present (not shown). Previously, this patient was diagnosed with a mammary carcinoma, suggesting metastasis from the mammary tumor (Wright–Giemsa, 500? magnification).
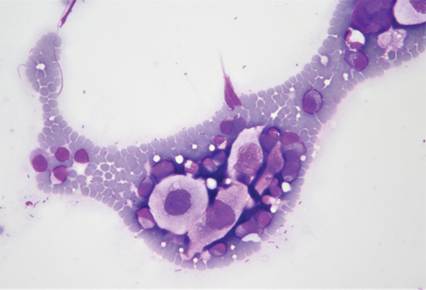
Figure 5.52 Cat, mandibular lymph node, FNA. Voluminous atypical epithelial cells with abundant clear cytoplasm and angular margins suggesting metastasis from an oral squamous cell carcinoma (May–Grünwald–Giemsa, 600? magnification).
Nonepithelial neoplasms metastasize through lymphatic vessels less commonly than epithelial tumors, but in some cases lymph node metastases may be found. Oral melanoma has a high tendency to metastasize to submandibular lymph nodes. Neoplastic cells may be spindle-shaped to oval to round and may occasionally be found in small clusters. Fine brown/black granules may be observed (Figure 5.53), but are lacking in aspirates from amelanotic melanomas, making this tumor type much more difficult to identify. Neoplastic melanocytes must be differentiated from melanin laden macrophages (melanophages) that may accompany melanocytic tumors or reactive conditions. Granules in melanophages are generally more variable in size and larger than seen in melanocytes, and cytoplasmic vacuoles are frequently found. Hemangiosarcoma may also metastasize to lymph nodes. Neoplastic cells are generally individualized, spindle-shaped, large, and may contain phagocytized erythrocytes, blue–black hemosiderin pigment, or small vacuoles. Figure 5.53 Dog, mandibular lymph node, FNA. Several large spindle cells, often cont aining fine black granules, indicating a metastasis from an oral malignant melanoma (May–Grünwald–Giemsa, 1,000? magnification).
Metastasis of round cell tumors also occurs frequently. Lymph node aspirates may be a part of the staging procedure for mast cell tumors. Since detection of mast cells in lymph nodes may be a normal feature, the issue of the percentage of mast cells in a lymph node aspirate must be considered if metastasis is suspected. Generally, a percentage higher than 3% mast cells with atypical morphologic characteristics (e.g. poorly granulated cells, binucleation) is suggestive of lymph node infiltration (Figure 5.54). The presence of foci of aggregated mast cells may strongly support the hypothesis of metastatic disease, as this feature is rarely recognized in normal cytologic aspirates. Eosinophilic infiltration accompanying the primary neoplasia may also be present. Less frequently, transmissible venereal tumors (TVTs) invade lymph nodes. Cells from TVTs are round with gray cytoplasm, often vacuolated, and have a round nucleus with coarse chromatin. Plasma cell tumors (multiple myeloma and plasmacytoma) do not typically invade lymph nodes, but in some cases neoplastic plasma cells may be found (Figure 5.55). It may be difficult to differentiate severe plasma cell hyperplasia from a metastatic plasma cell tumor. In these cases, bone marrow aspirates and serum protein electrophoresis are recommended. Figure 5.54 Dog, peripheral lymph node, FNA. Mast cell tumor. Many well-differentiated, granulated mast cells are found in the draining lymph node from a dog with cutaneous mastocytoma (May–Grünwald–Giemsa, 1,000? magnification).
Figure 5.55 Dog, peripheral lymph node, FNA. Plasma cell tumor. Several plasma cells with mild signs of malignancy. The high percentage of cells in spite of the minimal atypia supports the diagnosis of a well-differentiated plasma cell tumor (May–Grünwald–Giemsa, 400? magnification).
Extranodal lymphoid neoplasms including cutaneous epitheliotropic lymphoma, chronic lymphoid leukemia, and acute lymphoid leukemia may infiltrate lymph nodes. Cutaneous epitheliotropic lymphoma (mycosis fungoides) cells are variable in size, with moderately abundant, lightly basophilic cytoplasm, sometimes with fine purple granules, and an indented nucleus that is occasionally cerebriform (Sezary cell-type) and poorly visible nucleoli (Figure 5.56). These cells generally exhibit a T CD8+ phenotype, which may be useful for tracking the infiltration in the lymph nodes and in the bone marrow. Leukemias that infiltrate lymph nodes generally cause mild to moderate lymphadenomegaly and only rarely efface the normal resident lymphoid population (Figures 5.57, 5.58). Complete blood count (CBC), examination of peripheral blood smears, and bone marrow aspiration cytology are needed to fully characterize infiltrative leukemias. Molecular testing is often needed to definitively diagnose the presence of metastatic lymphoid cells within a lymph node. Figure 5.56 Dog, axillary lymph node, FNA. Mycosis fungoides. Several large lymphoid cells with mildly basophilic cytoplasm, several vacuoles, oval or indented nuclei, and several mitotic figures. This feature is suggestive of lymph node metastasis from cutaneous epitheliotropic lymphoma (May–Grünwald–Giemsa, 1,000? magnification).
Figure 5.57 Dog, peripheral lymph node, FNA. Chronic lymphocytic leukemia. Presence of many neoplastic small lymphoid cells with clear cytoplasm admixed with resident and reactive lymph nodal population (May–Grünwald–Giemsa, 1,000? magnification).
Figure 5.58 Dog, peripheral lymph node, FNA. Acute myeloid leukemia. Large blast cells with an indented nucleus and clear perinuclear halo (resembling monoblasts) are admixed with resident and reactive lymph nodal population; some neutrophils are also evident. Flow cytometry confirmed the monoblastic origin of the neoplastic cells (May–Grünwald–Giemsa, 1,000? magnification).
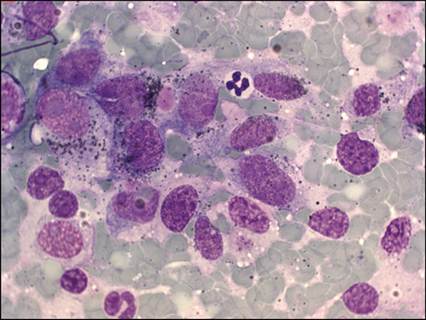
Histiocytic diseases (mainly disseminated histiocytic sarcoma and malignant histiocytosis) frequently metastasize to lymph node. Tumor cells may be identified by their large size and pleomorphism (Figure 5.59). Malignant histiocytes often have abundant cytoplasm that is lightly basophilic and vacuolated; in some subtypes, erythrophagocytosis may be found. Nuclei are bean-shaped or convoluted, with prominent nucleoli, and are frequently multinucleated. Although hystiocytic lineage-specific markers are lacking, immunostaining for CD18, CD45, CD11c, CD11d, CD1, and MHC class II may help to confirm cytologic suspicion and define the subtype of the disease (Moore, 2014). Figure 5.59 Dog, peripheral lymph node, FNA. Disseminated histiocytic sarcoma. Several large, pleomorphic histiocytoid cells, isolated or in clusters, with several malignancy signs, replace most of the resident lymphoid population (May–Grünwald–Giemsa, 400? magnification) (courtesy Ugo Bonfanti).
Spleen Indications for sampling Sampling for splenic cytology by fine needle biopsy, preferably without aspiration, is indicated in cases of splenomegaly and when changes in ultrasonographic aspects of the spleen have been identified. In addition, the spleen may be investigated in staging procedures for mast cell tumors, lymphoma, and histiocytic diseases. Book et al. (2011) reported splenic infiltration as a prognostic factor predicting survival in dogs with mast cell tumors. However, a study that evaluated healthy dogs and dogs with cutaneous mastocytoma concluded that the significance of finding increased numbers of mast cells in splenic aspirates, without any concurrent ultrasonographic changes, is too low to support splenic aspiration as a staging tool (Finora et al., 2006). A recent paper reported more than 30% false-negative results in staging cutaneous mast cell tumors via cytology when compared to histology (Ku et al., 2017). Some authors suggest that care should be taken in performing aspiration from splenic masses because of the possible dissemination of neoplastic cells along the needle tract or the rupture of blood-filled masses (Osborne et al., 1974; Johnson et al., 1989). However, several studies (Ballegeer et al., 2007, Watson et al. 2011; Christiansen et al., 2016) reported percutaneous ultrasound-guided FNA as sufficiently safe and accurate, providing a high agreement with histologic biopsies. Sampling FNA or fenestration may be performed without general anesthesia, but ultrasound-guided sampling is highly recommended. Dogs should be placed in right lateral or dorsal recumbency and surgical disinfection of the skin should be performed. Body movement should be carefully avoided by sedation or restraint, particularly if thrombocytopenia is present. Whichever technique is employed, a 21–23-gauge needle should be used to minimize hemodilution and reduce complications. Fine needle fenestration is the preferred method of collecting splenic cytology samples because it allows for minimal hemodilution and adequate cellularity (Leblanc et al., 2009). Collection of a sample for ancillary techniques (flow cytometry and molecular biology) requires FNA; coating of the syringe and needle with 4% EDTA helps to avoid clotting. Regardless of the sampling technique, smears should be prepared in the same manner as blood films to minimize rupture of splenic cells and erythrocytes. If splenectomy is performed, impression smears can be prepared so that an immediate diagnosis may be made. The fresh cut tissue should be gently blotted onto absorbent paper before making imprints to remove excess blood and tissue fluids. Staining techniques are similar to those used for other lymphoid tissues and, if necessary, ancillary staining can be performed. Cytologic features related to sampling Ultrasound gel is often found in smears of splenic aspirates and should not be confused with granules from LGLs or mast cells. Blood contamination severely affects many cytologic smears by masking the relevant cell population. In addition to erythrocytes, cells from circulating blood may affect interpretation if severe leukocytosis is present, and may lead to a false interpretation of splenitis. Platelet clumps are another common component of peripheral blood in the sample. Extra- or perisplenic cells may be collected in the needle during sampling. In particular, mesothelial cells may be found isolated or in small clusters with a honeycomb appearance (Figure 5.60). This finding is considered incidental. Figure 5.60 Dog, spleen, FNA. Large sheet of mesothelial cells (arrow) with honeycomb appearance (inset). This feature is suggestive of sampling contamination and does not have any pathological meaning (May–Grünwald–Giemsa, 400? magnification) (courtesy U. Bonfanti).
Normal anatomy and cytology The spleen is surrounded by a thick capsule composed of fibroelastic tissue and smooth muscle cells. The capsule is covered by peritoneum and extends into the splenic parenchyma in trabeculae. The parenchyma is divided into red pulp, mainly composed of erythrocytes intermingled with a reticular stroma, blood vessels, and endothelial sinuses, and white pulp, composed of periarterial lymphatic sheets and lymphatic nodules supported by the reticular stroma. Splenic nodules may resemble primary or secondary follicles according to their activation status. The splenic artery enters the hilus of the organ and branches in an arterial tree, continuing in fine pulp capillaries, often surrounded by pericapillary macrophage sheets supported by reticular fibers (ellipsoids). The capillaries end in a terminal capillary that opens into the reticular stroma of the red pulp or into venous sinuses. Erythrocytes and lymphoid cells are the prevalent cell populations in splenic cytology samples. Their proportion may vary according to the area sampled and blood contamination. Lymphoid cells are mainly composed of mature small lymphocytes but, if germinal centers are sampled, blasts may be present in high percentages. Immunophenotyping of splenic lymphoid cells showed that T cells predominate (52%) in adult dogs, being mainly composed of T helper (CD4+) cells (32%). Approximately 25% of cells are B cells in adult dogs, but they may be the prevalent population (52%) in newborn puppies (Faldyna et al., 2005). In addition to erythrocytes and lymphocytes, a few macrophages and plasma cells may be found. Due to the normal activity of removal of damaged red blood cells, splenic macrophages may contain hemosiderin pigment (staining blue–black) or hematoidin crystals (golden yellow). Other cells that may normally be found at low percentages are mast cells, neutrophils, endothelial cells, and fibrocytes. The presence of aggregates of connective reticular tissue, often surrounded by macrophages (ellipsoids) or containing endothelial cells, fibrocytes, and lymphoid cells, is a normal cytologic feature (Figure 5.61). Figure 5.61 Dog, spleen, FNA. Macrophages embedded in fine reticular fibers surrounding a capillary structure. This feature is consistent with ellipsoids and does not have any pathological meaning (May–Grünwald–Giemsa, 400? magnification).
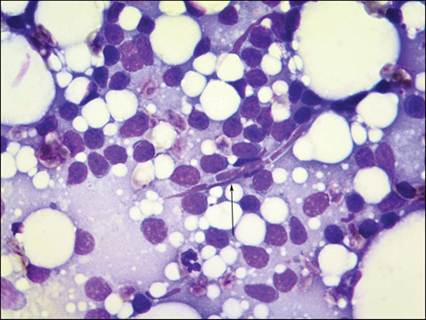
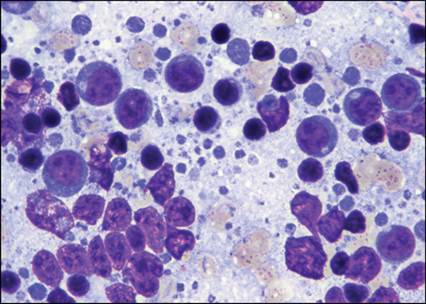
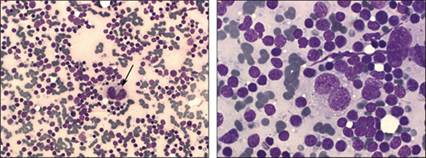
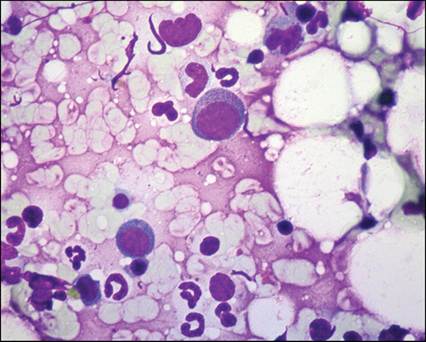
Extramedullary hematopoiesis The spleen is a major hematopoietic organ in fetal life. This function decreases after birth but it remains potentially inducible in cases of bone marrow failure or ineffective hematopoiesis. EMH is the most common cytologic finding in splenic aspirates, being present in approximately 24% of samples from dogs (O’Keefe & Couto, 1987). Often, clinical disease associated with EMH cannot be detected in these patients. Myelolipoma is a rare benign condition characterized by a marked EMH in the context of several lipid droplets and small clusters of normal appearing adipocytes (Figure 5.62). This disease process needs to be confirmed histologically. Severe EMH has been associated with chronic hemolytic anemia, myelo- and lymphoproliferative disorders, nonregenerative anemias with bone marrow failure, and splenic hemangiosarcoma (Bertazzolo et al., 2005). Detection of excessive numbers of macrophages with erythrophagocytosis may support a diagnosis of immune-mediated anemia. Evaluation of CBC data and a bone marrow aspirate are recommended if underlying disease is suspected. Splenomegaly is uncommon in animals with EMH, but hypoechoic nodules may be found. The detection of erythroid, myeloid, and megakaryocytic precursors is diagnostic for EMH (Figure 5.63). Sometimes, islets of immature erythroid cells surrounding macrophages (nurse cells) may be found. Figure 5.62 Dog, spleen, FNA. Myelolipoma. Myeloid and erythroid precursors and immature cells supporting extramedullary hematopoiesis, several lipid droplets, and normal adipocytes (May–Grünwald–Giemsa, 1,000? magnification).
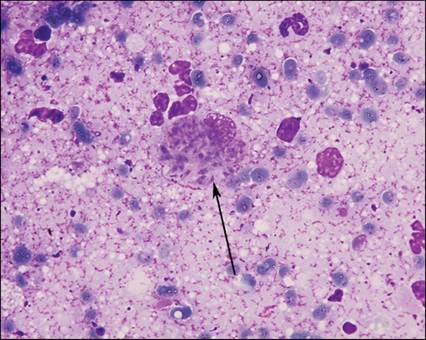
Figure 5.63 Dog, spleen, FNA. Extramedullary hematopoiesis. A large megakaryoblast and several erythroid immature cells are evident (May–Grünwald–Giemsa, 1,000? magnification).
Reactive hyperplasia The term splenic hyperplasia may be related to a variety of non-neoplastic conditions that lead to a diffuse enlargement of the spleen or to nodular focal lesions. Reactive hyperplastic spleen has an increase in the numbers of macrophages and plasma cells (Figure 5.64). Small lymphocytes are still the predominant lymphoid population, but medium to large lymphocytes frequently are increased. Mast cells may also be increased and are often associated with sheets of reticular fibers and capillaries. Neutrophils may be found and support possible concurrent inflammation. Figure 5.64 Dog, spleen, FNA. Reactive hyperplasia and extramedullary hematopoiesis. Several plasma cells and hematopoietic immature cells are found (May–Grünwald–Giemsa, 1,000? magnification).
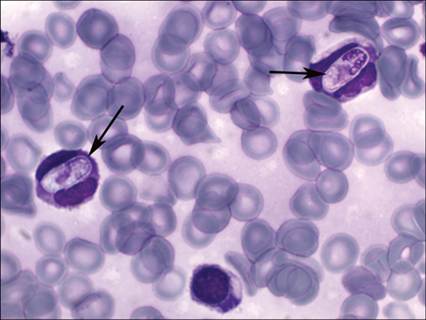
Splenitis Splenitis may be due to infectious or noninfectious diseases including immune-mediated diseases and malignancies. Concurrent peripheral blood evaluation is mandatory to determine if inflammatory cells are a component of the peripheral blood or a true infiltrate. Although detection of organisms may be challenging with infectious etiologies, splenic cytology may increase the sensitivity of peripheral blood smear examination alone. Leishmaniasis, histoplasmosis, cytauxzoonosis, babesiosis (Figure 5.65), hepatozoonosis (Figure 5.66), erhlichiosis, and anaplasmosis may cause histiocytic splenitis. Figure 5.65 Dog, spleen, FNA. Babesiosis. Four round to piriform merozoites of B. canis are found in an erythrocyte (arrow) (May–Grünwald–Giemsa, 2,000? magnification).
Figure 5.66 Dog spleen, FNA. Hepatozoonosis. Large cigar-shaped gamonts are visible in two neutrophils (arrows) (May–Grünwald–Giemsa, 2,000? magnification).
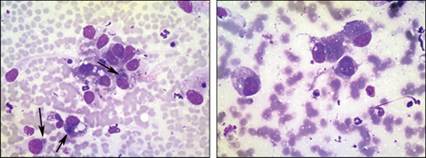
The term hemophagocytic syndrome is used to describe a wide range of different conditions characterized by an increased number of macrophages showing erythrophagocytosis and concurrent peripheral cytopenias. This condition is not rare in dogs, whereas it is quite rare in cats. Hemophagocytic syndrome may be idiopathic or associated with immune-mediated, infectious, or neoplastic diseases (Weiss, 2007). The distinction between reactive hemophagocytic syndrome and neoplastic hemophagocytic histiocytic sarcoma is often difficult. Non-hematopoietic neoplasia Neoplastic conditions commonly affect the spleen. Neoplastic diseases were present in approximately half of the samples from splenectomized dogs (Neer, 1996); this percentage was slightly lower (37%) in cats (Spangler & Culbertson, 1992). Hemangiosarcoma is the most common neoplasm of the spleen. Hemangiosarcoma has a poor prognosis since it tends to metastasize rapidly via blood flow or rupture of the primary splenic lesion. In a cytologic study on a cohort of 19 dogs with hemangiosarcoma, cytologic features were very variable (Bertazzolo et al., 2005). However, there are some common features that can lead to suspicion of hemangiosarcoma in an FNA or an impression smear. Blood contamination is often abundant and acute erythophagocytosis or hemosiderin-laden macrophages are frequent findings. Cellularity may be variable, likely depending more on the histologic subtype than on the sampling technique used. Cells may exfoliate singly or in loose clusters, or may aggregate in epithelioid-like nests mimicking epithelial architecture (Figure 5.67). Neoplastic cells are large, ranging from spindle to stellate to oval, with moderately abundant basophilic cytoplasm, sometimes with multiple punctate vacuoles (Figure 5.68). The nucleus is ovoid with coarse chromatin and one or more prominent nucleoli. Anisocytosis and anisokaryosis are common features. Binucleated and multinucleated cells are often found. Cytologic diagnosis of poorly differentiated hemangiosarcomas may be challenging. Immunophenotyping for positivity to factor VIII-related antigen and CD31 supports a diagnosis of hemangiosarcoma. Figure 5.67 Clusters of pleomorphic mesenchymal cells varying from polygonal to spindle. Erythrophagocytosis (arrows) is a common feature. Figure 5.68 Large globoid, to stellate hemangioblasts, with deeply basophilic cytoplasm, and several microvacuoles (May–Grünwald–Giemsa, 600? magnification) (courtesy U. Bonfanti).
Other primary mesenchymal tumors are rare in the spleen, but fibrosarcoma, leiomiosarcoma, osteosarcoma, liposarcoma, myxosarcoma, and pleomorphic undifferentiated sarcoma have been reported (Spangler et al., 1994). Cytologic aspects of these tumors are not different from those in other tissues. As in other lymphoid tissues, metastases of many tumor types may be found in the spleen. Hematopoietic neoplasia Primary or metastatic hematopoietic tumors may occur in the spleen. In many cases, splenic aspiration is a part of the staging procedure following a diagnosis of mastocytoma, lymphoma, or histiocytic diseases. In other cases, the spleen is the only organ involved and ultrasound-guided FNA is performed to investigate ultrasonic abnormalities or focal lesions.
More medical literature on Medic.Studio
More on the topic Microbiology:
-
Infectious diseases -
Internal diseases -
Obstetrics and Gynaecology -
Pediatrics -
Veterinary medicine -
-
Conflictology -
Ecology -
Economy -
Finance -
History -
Law -
Medicine -
Philosophy -
Religious studies -
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||