Normal pancreas structure
Anatomy
Canine and feline pancreas have the same gross anatomic organization: the organ is divided into three linked parts or into two parts (right and left lobes) united at the body of the pancreas.
In dogs, the right lobe of the pancreas lies dorsomedial to the descending duodenum, approximately from the middle of the ninth intercostal space to the fourth lumbar vertebra (Evans et al., 2013). The body of the pancreas unites the right and the left lobes at an angle of about 45 degrees and is closely linked to the caudal portion of the pyloric region. The left lobe runs from the body of the pancreas to the left of the abdomen, caudo-dorsally to the stomach and craniodorsally to the transverse colon, ending at the level of the cranial pole of the left kidney. As in the dog, feline pancreas follows the descending part of the duodenum but its distal extremity curves cranially in a hook-shaped manner (Barone, 1997). Moreover, following the pyloroduodenal angle, the feline body of the pancreas is more centrally located in the abdomen than it is in the dog. Unlike the dog, the main pancreatic duct and the common bile duct share the same entry into the feline duodenum, which may explain some pathologic relations between the duodenum, the gall bladder (and its bile duct), and the pancreas in cats (Forman et al., 2021).Histology
The pancreas is a lobulated, compound, tubuloacinar gland. It is surrounded by a thin collagenous capsule that gives rise to fine connective tissue septa dividing the gland into distinct lobules. Each lobule contains both exocrine and endocrine parts (Figure 8.1). The exocrine glandular component, which constitutes 80% to 85% of the organ, is responsible for the secretion of the pancreatic juice. The exocrine secretory pancreatic acini consist of typical two-colored spherical clusters of cells with a small central lumen, often difficult to see (Figure 8.2).
The acinar cells are pyramidal oriented cells with a spherical basal to parabasal nucleus and prominent nucleoli. They have a basal area of the cytoplasm that is deeply basophilic resulting from the accumulation of ribosomes and rough endoplasmic reticulum and an apical granular acidophilic cytoplasmic region due to zymogen granules (Banks, 1993; Eurell & Frappier, 2006). Nuclear and cytoplasmic features are both characteristic of cells highly active in protein synthesis (Figure 8.3). The acini open into a continuous short, narrow, intercalated duct, which begins with squamous to cuboidal epithelial centroacinar cells (Eurell & Frappier, 2006; Kierszenbaum et al., 2019). The latter cells extend into the lumen of the acinus and can be regarded as the intra-acinar part of the intercalated duct; their pale nuclei and sparse pale-stained cytoplasm frequently appear in the center of the acini (Figure 8.3). Weak staining of centroacinar cells and intercalated ducts is due to the secretion of water and bicarbonate ions. The intercalated ducts with narrow lumens drain then into larger intralobular ducts that present a central lumen and a cuboidal epithelium in transversal section. Intralobular ducts communicate with interlobular ducts, and progressively ductal epithelium changes from cuboidal to columnar. As the ductal system becomes confluent, the fine connective tissue associated with the acini and smaller ducts becomes thicker. Goblet cells may be observed among the epithelial cells of the larger ducts (Banks, 1993; Eurell & Frappier, 2006). The endocrine glandular component, the islets of Langerhans, produces mainly insulin and glucagon. Pancreatic islets are randomly scattered throughout the exocrine parenchyma and vary in size (Figure 8.1) (Eurell & Frappier, 2006; Young et al., 2006). They are composed of clusters of pale-staining cells supported by a fine collagenous network containing blood capillaries. The endocrine pale cells appear small compared to the large surrounding exocrine acinar cells (Figure 8.3). Lamellated or Pacini’s corpuscles can be observed in the connective tissue of the feline pancreas (Banks, 1993; Eurell & Frappier, 2006). Note that there are differences between histological and cytological observations due to the different areas of the pancreas that samples are collected and prepared from (Figure 8.4). 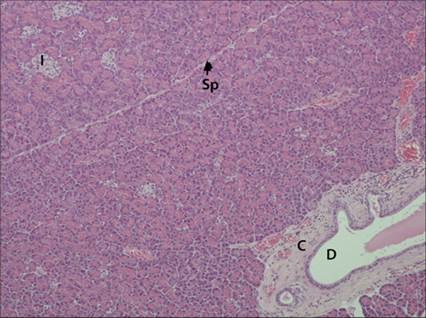
Figure 8.1 Feline pancreas. The mostly represented exocrine component consists of numerous contiguous acini and interlobular duct (D) surrounded by connective tissue (C). Delicate collagenous septa (Sp) are observed between lobules. The endocrine part is composed of clearer clusters of cells, the islets of Langerhans (I), randomly scattered throughout the exocrine part. Hematoxylin and eosin (?40).
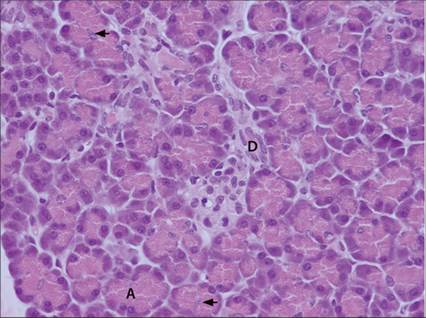
Figure 8.2 Feline pancreas. Exocrine pancreatic acini (A) consist of typical two-colored spherical clusters of cells with a very small central lumen. Pyramid-shaped acinar cells have a basal deep basophilia and an apical granular acidophilia; the spherical nucleus is basal to parabasal. The centers of the acini often contain nuclei of centroacinar cells (arrow). Intercalated duct (D) is lined by a simple low cuboidal epithelium; the small central lumen is filled with eosinophilic pancreatic juice. Hematoxylin and eosin (?400).
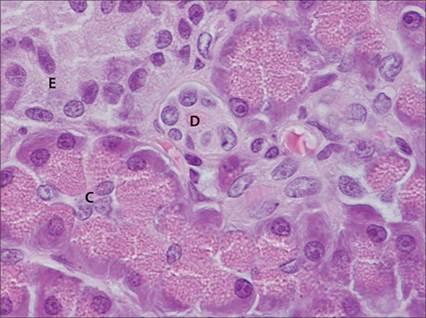
Figure 8.3 Feline pancreas. The polarity of the pyramid-shaped acinar cells can be seen easily at a higher magnification with the basal marked basophilia and the apical granular eosinophilia due to zymogen granules; their round nuclei located basally have prominent nucleoli. The pale nuclei and sparse pale-stained cytoplasm of centroacinar cells (C) appear in the lumen of an acinus. Centroacinar cells represent the intra-acinar part of the intercalated ducts (D) lined by a simple low cuboidal epithelium; the lumen is filled with eosinophilic pancreatic juice.
Endocrine secretory cells (E) constitutive of an islet of Langerhans appear as small pale stained cells in contrast to the acinar cells. Hematoxylin and eosin (?1,000).
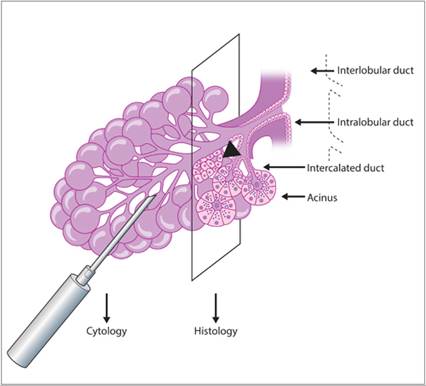
Figure 8.4 Glandular tubuloacinar organization of a pancreatic lobule with differences between histological and cytological observations consecutive to the different sampling methods. Islet of Langerhans (arrowhead)..
Ultrasound
In dogs, the right lobe of the pancreas is more easily seen than the body and the left lobe. In cats, the left lobe which is larger than the right lobe and the body are more easily identified than the right lobe (Etue et al., 2001; Hecht et al., 2007; Larson, 2016; Griffin, 2020); however, in both species, the pancreas is of relatively small size (thickness ranges from 3.5 to 16 mm in clinically normal dogs and from 2.8 to 9.5 mm in healthy cats) (Etue et al., 2001; Penninck et al., 2013). Also, the pancreas is intimately linked to the digestive tract, which is expected to create numerous artifacts. In healthy dogs, the pancreas usually has poorly distinct margins (Larson, 2016) whereas the feline pancreas is a well-defined organ (Griffin, 2020). In both species, the pancreatic parenchyma is isoechoic to slightly hypoechoic to surrounding mesenteric fat (Hecht & Henry, 2007) even if hyperechoic pancreas has been reported in a small population of healthy dogs, suggesting pancreatic hyperechogenicity could be a rare normal variant in the dog (Granger et al., 2015). The regions dorsal and dorsomedial to the descending duodenum, immediately ventral to the right kidney, are scanned for the right pancreatic lobe. The region ventral to the portal vein is scanned for the pancreatic body. Finally, the region caudal to the greater curvature of the stomach and cranial to the transverse colon is scanned for the left pancreatic lobe, extending toward the spleen and the left kidney in the cat (Robben et al., 2005; Larson, 2016; Griffin, 2020).
Ultrasound-guided fine needle aspiration (US FNA)
Self-evidently, the first step in performing pancreatic US FNA is to visualize the pancreas, which may be difficult, as discussed above. Cordner et al. studied pancreatic cytologic FNA yield and secondary effects in 27 healthy dogs. No acute complication or significant increase in serum canine pancreatic lipase immunoreactivity (cPLI) and trypsine-like immunoreactivity (TLI) values after pancreas US FNA were noted, suggesting that the trauma to the pancreas during this procedure is minimal. However, no aspirate was of sufficient quality to be diagnostic. The authors concluded that US FNA of the normal pancreas is unlikely to provide adequate cytologic sample, incriminating the particular tightly associated fibrovascular network of the normal pancreatic tissue and the limited experience of the operator in pancreas US FNA (Cordner et al., 2010). Crain et al. reported no increase in complication or mortality rates in cats after pancreatic aspiration, concluding feline US FNA was a safe procedure (Crain et al., 2015). In dogs and cats, transabdominal US FNA feasibility is highly dependent on numerous factors such as patient conformation (deep chest, obesity), ultrasound machine performance, and experience of the radiologist (Robben et al., 2005). Fortunately, pancreatic lesions usually facilitate visualization of the pancreas by significantly changing its echogenicity and its size. However, ultrasonographic findings in various pancreatic diseases overlap, usually preventing the radiologist from establishing a definitive diagnosis, and US FNA is needed to obtain additional diagnostic information (Hecht & Henry, 2007; Vanderperren et al., 2014). When fluid is present in the abdomen, cytopathology of the fluid can be diagnostic in the case of exocrine carcinoma, but it has been shown to have a lower success rate than tissue aspiration (Bennett et al., 2001; Armstrong et al., 2012). To increase the success of pancreatic aspiration, the shortest distance as well as the safest route between the skin and the target must be chosen.
Clean, dry, and grease-free glass slides are set out before the procedure and close to the working area in order to shorten the time between the end of aspiration and the expelling of the sample onto the slide (Bjorneby et al., 2002). The needles most currently mentioned in the literature are 22-gauge single-use disposable spinal or cystocentesis needles (VanEnkevort et al., 1999; Bjorneby & Kari, 2002; Cordner et al., 2010). However, one author suggests that a 25-gauge needle would be effective for cytologic evaluation and less traumatic than larger-gauge needles (Mansfield, 2013). This observation is in accordance with recently published 25-gauge EUS FNA needle performance on solid human pancreatic lesions (Anderson et al., 2008; Siddiqui et al., 2009; Varadarajulu et al., 2014) but has yet to be thoroughly studied in veterinary practice in randomized studies. Crain et al. safely aspirated 73 feline pancreas using 20- or 22-gauge hypodermic needles (Crain et al., 2015), and Kook et al. used 19-gauge needles for pancreas EUS FNA on 12 dogs with no reported adverse effects (Kook et al., 2012). However, in human medicine, 19-gauge needles are rarely used because they are considered too rigid to pass through the echoendoscope and because of an increased risk of bleeding (Siddiqui et al., 2009).
Three techniques are mentioned in the literature to guide the needle: indirect guidance, needle guidance system, and freehand guidance. Indirect guidance, which refers to the removal of the transducer before inserting the needle, is, in our opinion, highly risky and should not be considered acceptable, particularly for pancreas FNA. The needle guidance system, which uses a biopsy guide attached to the transducer, is described as the easiest biopsy method, allowing the operator to visualize the theoretical needle path by means of dots or lines superimposed on the screen. The third technique, known as freehand guidance, might sound risky but is, with a little practice, far more satisfying than the systematic use of the needle guidance system because of the movement freedom it allows. Once the needle is inserted in the pancreas, aspiration or fenestration techniques are possible as described in Chapter 1.
The smears must be prepared quickly to avoid clotting (Bjorneby & Kari, 2002); the plunger of the syringe is gently pressed to expel the needle content onto the slide. Several slides might be necessary depending on the specimen amount: indeed, a small drop is enough to avoid artifacts. The sample is then smeared using a blood smear technique, taking care not to crush the cellular material. The smears are immediately air dried and labeled before submission (Bjorneby & Kari, 2002).
Cytology
FNA smears from a normal pancreas are often bloody and of poor quality (Cordner et al., 2010; Borjesson, 2014). The main cell population observed is acinar cells from the exocrine portion of the pancreas as it constitutes 98% of the pancreatic mass (Bjorneby & Kari, 2002; Borjesson, 2014). They are often present in clusters organized in a round acinar pattern, but they can also be isolated and disrupted (Figure 8.5). When samples are very cellular, larger lobules can be observed and are quite similar to other lobulated structures such as those in salivary gland cytology (Figures 8.6a and 8.6b). These cells are small to medium (their nucleus is about 10 µm in diameter), with poorly defined cytoplasmic edges, a polygonal or pyramidal form with a round and uniform basal nucleus, a medium to low nuclear to cytoplasmic (N:C) ratio, and granular cytoplasm (Figure 8.5). The cytoplasm is relatively abundant, basophilic, and contains a large quantity of very small eosinophilic granules, the zymogen granules (Borjesson, 2014). Disrupted cells are often observed and the non-cellular background is often basophilic and granular (Borjesson, 2014). The nuclei contain heterogeneous chromatin (clumped and granular) with small, occasionally prominent nucleoli (Borjesson, 2014).
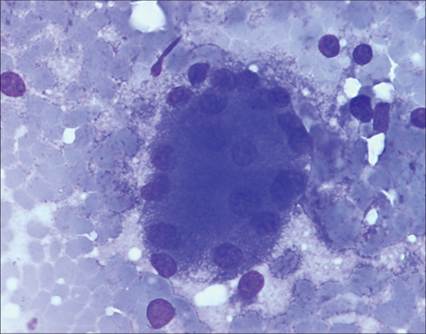
Figure 8.5 Aspirate of a normal pancreas from a dog. Acinar cells. Bloody and granular basophilic background associated with acinar cells. Medium-sized cells with a medium nuclear to cytoplasmic ratio have a pyramidal outline with indistinct cell borders. Their nuclei are eccentric, round with granular and clumped chromatin and a distinct nucleolus. Their cytoplasm is basophilic and characterized by a prominent, coarse cytoplasmic granularity due to zymogen granules. May–Grünwald–Giemsa (?1,000).
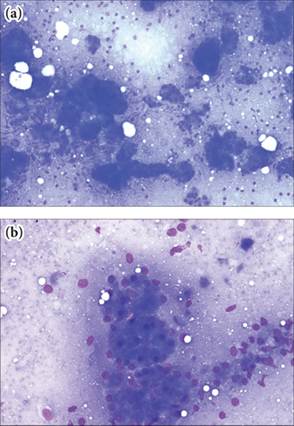
Figure 8.6 a, b Aspirate of a normal pancreas from a cat. Acinar cells. Acinar cells. Bloody and granular basophilic background associated with 2-dimensional microacinar structures and 3-dimensional grape-like clusters and collecting ductal system very similar to salivary gland. May-Grünwald Giemsa (6a: x200; 6b: x400).
Ductal cells can sometimes be seen (Figures 8.7a and 8.7b). These cells are often organized into a typical tubular pattern or in a honeycomb pattern if the ductus is disrupted. The cells are intermediate-sized with a very high nuclear to cytoplasmic (N:C) ratio, a well-defined light basophilic cytoplasm, and an ovoid nucleus with stippled chromatin. Cells are cuboidal in the small ductus and columnar, sometimes ciliated, in the larger ductal structures (Bjorneby & Kari, 2002).

Figures 8.7a,b Aspirate of a normal pancreas from a cat. Ductal cells. (a) Large and smaller ducts connected. May–Grünwald–Giemsa (?100). (b)Cohesive epithelial cells organized in a tubular pattern. Ductal cells are medium sized with a high nuclear to cytoplasmic ratio and a cuboidal shape. Nuclei are ovoid with a stippled chromatin. Cytoplasm is pale and scant. May-Grünwald Giemsa (x400).
Mesothelial cells can also be seen (Figure 8.8) (Yang et al., 2008). These medium to large cells are cohesive and organized in thin sheets occasionally with a cobblestone appearance. They are polyhedral, with a light blue well-defined cytoplasm and a central round to ovoid nucleus composed of finely reticular chromatin. Some inflammatory cells can be seen and should be evaluated in light of the blood contamination and leukocyte count. Because of its anatomic relationship with the stomach, intestine, spleen, and kidney, and depending on the sampling procedure, other organs may be sampled inadvertently in addition to the pancreas (Yang & Tao, 2008).
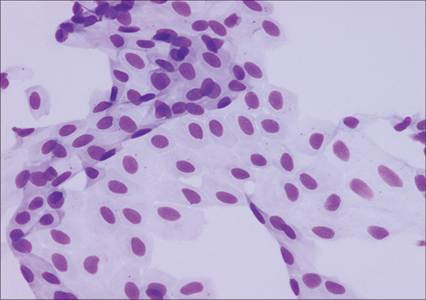
Figure 8.8 Aspirate of a normal pancreas from a cat. Mesothelial cells. Flat sheet of cohesive uniform cells. These medium-sized cells with a medium nuclear to cytoplasmic ratio are polygonal with well-defined cell borders. Their cytoplasm is delicate, and their ovoid nucleus is finely reticulated. May–Grünwald–Giemsa (?400).