Pathology of the central nervous system
Infectious lesions
Bacterial meningitis
Bacterial meningitis typically presents in a patient who is reluctant to move and extremely painful but otherwise does not show specific, focal neurologic lesions (Table 14.4).
Bacteria may access the CNS by direct implantation (trauma, CSF tap), local spread (diskospondylitis), or hematogenous spread from bacteremia. Common bacterial causes include Staphylococcus spp., Escherichia coli, Pasteurella multocida, Actinomyces spp., Nocardia spp., Streptococcus spp., and, rarely, some anaerobic entities (Tipold & Stein, 2010). Table 14.4 A summary of the significant diagnostic findings with bacterial meningitis
| Signalment | Any | ![tab14.4.jpg]() |
| Clarity | Clear to turbid |
| Color | Possible red/xanthochromia |
| CSF TP | Mild to marked increase |
| CSF cellularity | Acute: mild to marked neutrophilic pleocytosis |
| | Chronic: mixed or mononuclear pleocytosis |
| CNS cytology | Not commonly performed |
| Ancillary testing | Culture, PCR |
| Notes | Bacteria are not commonly observed on CSF even when culture positive |
CSF analysis most commonly reveals a neutrophilic pleocytosis with increased CSF TP (Figures 14.31a–d, 14.32). With chronicity or antibiotic therapy, a mixed or mononuclear pleocytosis may occur. Direct observation of bacteria in the cytologic preparation is rare but can occur (Radaelli & Platt, 2002). In cases with a high index of suspicion, collection in a non-EDTA containing tube for bacterial culture or polymerase chain reaction (PCR) is appropriate, independent of what is found on cytologic evaluation of the sample.
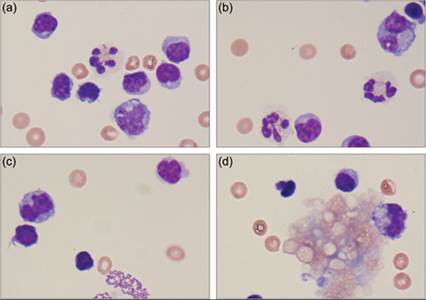
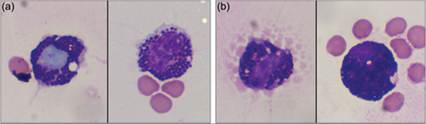
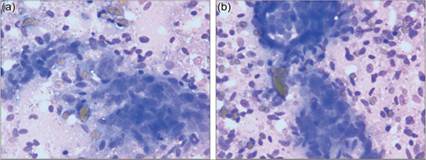
One report of necropsy confirmed bacterial meningitis in the dog found that only one in eight CSF samples grew bacteria on routine cultures (Radaelli & Platt, 2002). ![fig14.31A-D.jpg]()
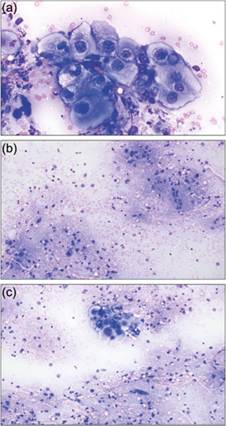
Figure –d 14.31a CSF from an 8-year-old Jack Russell Terrier. TNCC = 286 cells/μl, CSF TP = 472 mg/dl. (a, b) A mixed pleocytosis with small mononuclear cells, large mononuclear cells, and neutrophils is present. Note the small rod-shaped bacteria within the neutrophils. (c) Large mats of rod-shaped bacteria are also present extracellularly. (d) An aggregate of myelin with small round structures inside foamy eosinophilic to basophilic material is present. Although this can be an incidental finding, given the history and cytologic findings, myelomalacia is a more likely cause (Wright–Giemsa, 1,000? magnification). The patient was diagnosed with bacterial meningitis. She responded well to medical management.
Prognosis with bacterial meningitis is variable, depending on the exact etiology, underlying patient factors, and the clinician’s ability to institute appropriate early antimicrobial therapy (Muñana, 1996).
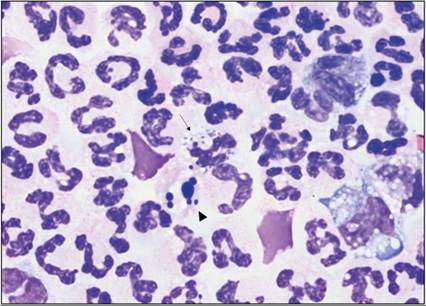
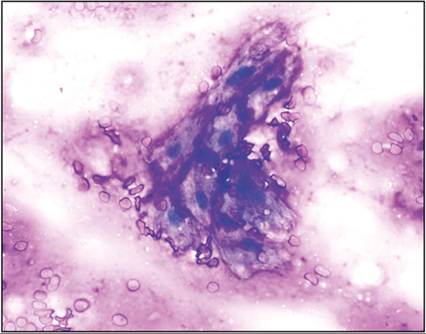
![fig14.32.jpg]()
Figure 14.32 CSF from a 12-year-old mixed breed dog. TNCC = 157,830 cells/μl, CSF TP = 4,158 mg/dl. A marked neutrophilic pleocytosis is present with many neutrophils appearing degenerate. Rare neutrophils contain intracellular cocci bacteria arranged in pairs (thin arrow). A leukocyte undergoing karyorrhexis is also shown (arrowhead), which should not be mistaken for intracellular bacteria or fungal yeast (Wright–Giemsa, 1,000? magnification). The patient had concurrent septic peritonitis, a hepatic abscess, and suspected bacteremia.
Canine distemper virus encephalitis
With adequate vaccination, canine distemper virus (CDV) encephalitis is less common than in years past and vaccine-associated cases are rarely seen (Table 14.5).
Classic clinical signs of CDV encephalitis include chewing gum seizures, myoclonus (rhythmic muscle jerking), vestibular signs, and circling or dementia, depending on the immunocompetence and age at onset of signs (Thomas, 1998). Table 14.5 A summary of the significant diagnostic findings with canine distemper virus encephalitis
| Signalment | Dogs; all ages | ![tab14.5.jpg]() |
| Clarity | Clear |
| Color | Colorless |
| CSF TP | Mild to marked increase |
| CSF cellularity | Young dogs: mild neutrophilic pleocytosis Older dogs: moderate mononuclear pleocytosis |
| CNS cytology | Not commonly performed |
| Ancillary testing | CSF antibody titer, IgG index, RT-PCR |
| Notes | Younger dogs: chewing gum seizures, vestibular dysfunction, myoclonus Older dogs: encephalitis |
CSF findings with CDV encephalitis are dependent on age (Thomas, 1998). Younger dogs typically have a mild neutrophilic pleocytosis with mildly increased CSF TP. Mature dogs have a moderate mononuclear pleocytosis with moderate elevations of CSF TP. Increased CSF TP without concurrent elevations in TNCC are seen (Koutinas et al., 2002). CSF antibody titers IgG index, and RT-PCR have been used to help support a CDV encephalitis diagnosis.
Feline infectious peritonitis meningoencephalitis/meningomyelitis
CNS involvement of the coronavirus infection FIP is typically seen in cats 1,000 cells/μl. Evidence of hemorrhage, including xanthochromia and erythrophagocytosis, is common (Figures 14.33a–d). Elevated immunoglobulin levels, typically IgA, are reported prominent findings. Elevated CSF IL-8, matrix metalloproteinases, and CD11a have been noted in the CSF and could be the cause of the marked pleocytosis.
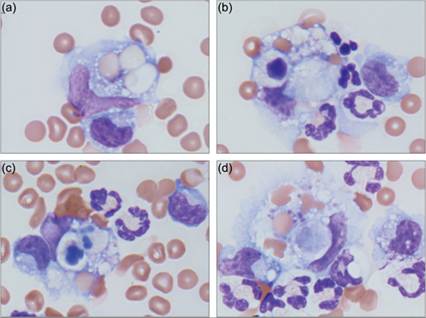
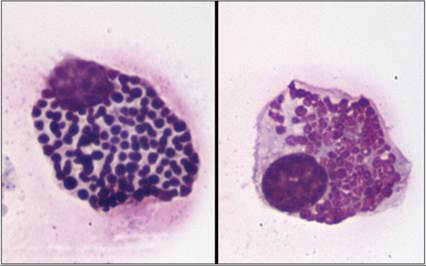
An altered B-cell/T-cell ratio in the blood and CSF, leading to a Th2 response and autoantibody production, can be seen as well. A concurrent peripheral leukocytosis is common (Tipold & Stein, 2010). ![fig14.33A-D.jpg]()
Figures 14.33a–d CSF from a 1-year-old, spayed female German Shorthaired Pointer. TNCC = 4,060 cells/μl, CSF TP = 320 mg/dl. (a) Large mononuclear cells in the sample display pronounced erythrophagocytosis. (b–d) Many large mononuclear cells have phagocytized cellular debris (Wright–Giemsa, 1,000? magnification). Evaluation of synovial fluid from the right carpus and both stifle joints suggested a concurrent immune-mediated polyarthritis; the inflammatory lesions in the CSF are interpreted as part of a systemic autoimmune disease. The infectious agent profile was negative; the patient responded well to prolonged immunosuppression.
As the name implies, the disease commonly requires immunosuppressive doses of glucocorticoids or other immunosuppressive drugs to attain remission. Because the clinical pathology findings with the disease are not highly specific for SRMA, exclusion of other causes of a marked neutrophilic pleocytosis is warranted. Of special note is that many SRMA cases look similar to bacterial meningitis on CSF analysis. Since cytologic detection of bacteria in CSF is not 100% sensitive, culture or other appropriate infectious disease testing before starting immunosuppressive therapy may be warranted in case of suspected SRMA.
Meningoencephalitis of unknown etiology
As definitive diagnosis of immune-mediated inflammatory disease of the CSF requires histopathologic diagnosis, patients with compatible clinical signs, CSF, and imaging findings are often placed under the umbrella diagnosis of meningoencephalitis of unknown etiology (MUE). Histopathologic subtypes of MUE include granulomatous meningoencephalomyelitis (GME), necrotizing leukoencephalitis (NLE), and necrotizing meningoencephalitis (NME).
A T-cell mediated immune-mediated pathogenesis has been proposed for these conditions, although the trigger of this response has not yet been determined (Vitale & Foss, 2019). Granulomatous meningoencephalomyelitis
Granulomatous meningoencephalomyelitis (GME) is an autoimmune inflammatory disease of the canine CNS that accounts for 5–25% of CNS disorders in the dog (Table 14.8; Suzuki et al., 2003; Adamo et al., 2007; Talarico & Schatzberg, 2010). The exact instigator of the autoimmune response is unknown. It presents as large accumulations of mononuclear cells cuffing small blood vessels in the parenchyma and meninges of the cerebrum, brainstem, spinal cord, or rarely cerebellum (Higginbotham et al., 2007). Ocular, focal, or disseminated forms of GME occur; rarely, the focal lesions can appear mass-like on imaging and can be found in the cerebrum with smaller disseminated lesions (Thomas, 1999). GME is typically seen in small breed dogs, especially toy breed and terriers. Females may be overrepresented (Higginbotham et al., 2007).
Table 14.8 A summary of the significant diagnostic findings with granulomatous meningoencephalomyelitis
| Signalment | Small breed dogs, especially toy breeds and terriers. Possible female bias | ![tab14.8.jpg]() |
| Clarity | Clear to turbid |
| Color | Possible red/xanthochromia |
| CSF TP | Moderate to marked increase |
| CSF cellularity | Moderate to marked mononuclear pleocytosis Rarely, neutrophilic pleocytosis |
| CNS cytology | Mononuclear inflammation |
| Ancillary testing | CSF-based autoantibody testing is possible |
| Notes | Necrosis is present but most often not seen |
CSF findings typically include a lymphocytic/small mononuclear pleocytosis (TNCC = 50–900 cells/μl) and increased protein (CSF TP = 40–400 mg/dl) (Figure 14.34; Adamo et al., 2007).
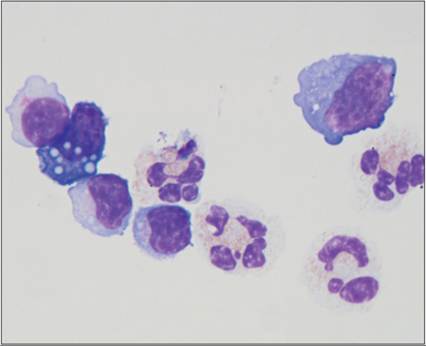
A neutrophilic or large mononuclear pleocytosis may also occur; one study found that 17% of GME patients had a neutrophilic pleocytosis. Confirmed cases of GME have even been found to have normal CSF (Bailey & Higgins, 1986). FNA might be utilized in cases with a focal/mass-type lesion. An inflammatory population would be expected on CNS cytology based on histologic biopsies of GME; however, this has not been reported in the literature. ![fig14.34.jpg]()
Figure 14.34 CSF from a 12-year-old mixed breed dog. TNCC = 426 cells/μl, CSF TP = 136 mg/dl. There is a mixed pleocytosis with small and large mononuclear cells most predominant and lower numbers of neutrophils. Plasma cells, including Mott cells, are also present in the sample and suggest intrathecal immunoglobulin production (Wright–Giemsa, 1,000? magnification). Infectious disease testing was negative. The clinical diagnosis was granulomatous meningoencephalomyelitis. Neurologic signs responded well to immune suppression.
As with SRMA, immunosuppression is a mainstay of GME treatment. CSF analysis and fine needle cytology are not sensitive enough for detection of infectious agents; culture or other diagnostic techniques should be used prior to immunosuppression.
Necrotizing leukoencephalitis
Originally named necrotizing encephalitis and described in the Yorkshire Terrier, necrotizing leukoencephalitis (NLE) has been reported in young (average 4.5 years old) dogs of other breeds as well (Table 14.9; Higginbotham et al., 2007). It can be found in the cerebrum and brainstem with clinical signs associated with the location of the lesion. The inciting cause is unknown.
Table 14.9 A summary of the significant diagnostic findings with necrotizing leukoencephalitis
| Signalment | Yorkshire Terriers, other dogs. Young adults | ![tab14.9.jpg]() |
| Clarity | Clear |
| Color | Colorless |
| CSF TP | Mild to moderate increase |
| CSF cellularity | Mild mixed pleocytosis |
| CNS cytology | Not commonly performed |
| Ancillary testing | CSF-based autoantibody testing is possible |
| Notes | Necrosis is not commonly apparent on CSF |
Histologically, NLE presents as a focal area of necrosis in the white matter of the cerebrum and thalamus. This necrosis is often not observed in CSF analysis; instead there is a mild, typically mixed pleocytosis and mild to moderate CSF TP elevations.
Necrotizing meningoencephalitis
Necrotizing meningoencephalitis (NME) has historically been called pug-dog encephalitis. Similar findings have been reported in non-pug dogs; most are juvenile to young adults (Table 14.10; Higginbotham et al., 2007). An autoimmune process is suspected (Suzuki et al., 2003; Talarico & Schatzberg, 2010). Like NLE, NME consists of focal lesions with a necrotic center. In NME the lesion is typically restricted to the cerebrum.
Table 14.10 A summary of the significant diagnostic findings with necrotizing meningoencephalitis
| Signalment | Pugs and other dog breeds. Juvenile to young adults | ![tab14.10.jpg]() |
| Clarity | Clear |
| Color | Colorless |
| CSF TP | Mild to moderate elevations |
| CSF cellularity | Moderate small mononuclear pleocytosis |
| CNS cytology | Not commonly performed |
| Ancillary testing | CSF-based autoantibody testing is possible |
| Notes | Previously called pug-dog encephalitis |
Another distinction between NME and NLE is the decidedly lymphocytic/small mononuclear pleocytosis found in most cases of NME (Higginbotham et al., 2007). Sixteen of 17 cases with histologic confirmation of NME had a small mononuclear predominance with a mean percentage of 90% small mononuclear cells. Neutrophilic, large mononuclear, or mixed pleocytosis, or even normal CSF cell counts can be observed. Otherwise presentation is similar to NLE.
Cerebrovascular accidents/stroke
Previously, it was believed that cerebrovascular accidents (CVAs) did not routinely occur in dogs and cats. However, they are increasingly being recognized in veterinary medicine (Table 14.11; Garosi et al., 2006). Mean age for dogs with a CVA is 8 years, although patients as young as 18 months have been reported. One study found eight of 40 (20%) dogs were Cavalier King Charles Spaniels and another 12% were Greyhounds, which probably is an overrepresentation of these breeds, although a breakdown of the common breeds at the reporting institution was not included to help support or refute this assumption (Garosi et al., 2006). Underlying causes of CVAs in veterinary medicine have not been well documented. Lesions can be located in the telencephalon, thalamus/midbrain, cerebellum, and multifocally. CVAs can be further classified as either ischemic (infarction due to obstruction) or hemorrhagic (due to rupturing of vasculature) events.
Table 14.11 A summary of significant diagnostic findings with cerebrovascular accidents (strokes)
| Signalment | Dogs and cats. Cavalier King Charles Spaniel, Greyhounds may be predisposed | ![tab14.11.jpg]() |
| Clarity | Clear to turbid |
| Color | Possible red/xanthochromia |
| CSF TP | Mild to moderate increase |
| CSF cellularity | Normal to marked neutrophilic or large mononuclear pleocytosis |
| CNS cytology | Not commonly performed |
| Ancillary testing | Diagnosis by imaging. Glutamate quantification may be helpful |
| Notes | Ischemic and hemorrhagic forms exist |
CVAs show signs of hemorrhage on CSF, including increased CSF protein, mild neutrophilic or mononuclear pleocytosis (TNCC 0.7 and deep pain negative may be highly sensitive indicator of a negative outcome
Because of the variable pathology associated with IVDD, CSF findings can be variable. In a series of 30 dogs with IVDD, a median CSF TP of 24.1 mg/dl was reported and 43% had a mild increase in CSF TP (Chamisha et al., 2015). Mild to moderate pleocytosis was seen in 51% of dogs. The incidence of pleocytosis could be further broken down into 23% of cervical cases and 61% of thoracolumbar cases showing pleocytosis (Brisson, 2010). Median TNCC was 52 cells/μl, with various forms of pleocytosis noted (Chamisha et al., 2015). Erythrophagia was noted in only 19% of cases. In other reports, myelin figures have been seen in the CSF of patients with IVDD (Fallin et al., 1996).
Most commonly, CSF analysis does not significantly add to the diagnosis of IVDD; radiographic techniques are sufficiently informative to allow a diagnosis. However, once the diagnosis of IVDD has been made, evaluation of the CSF can be prognostic. A neutrophilic pleocytosis typically is found in acute cases of IVDD. Cases with fewer neutrophils, more large mononuclear cells, lower TP, and lower RBC counts likely have had sufficient time to progress from an acute inflammatory response to a more chronic state and therefore are more likely to have a worse outcome (Srugo et al., 2011; Levine et al., 2014). Recent studies have evaluated several biomarkers and visually determined macrophage:monocyte ratios in CSF as potential prognostic markers in IVDD (Bittermann et al., 2019; Chamisha et al., 2015; Levine et al., 2010). Although results from these studies are somewhat conflicting, myelin basic protein and creatine kinase concentrations have been shown to be highly predictive of return to ambulatory function. (Olby et al., 2020). Further evaluation of the clinical utility of these biomarkers is needed.
Fibrocartilaginous embolus
Fibrocartilaginous emboli (FCE) most commonly, but not exclusively, occur in large and giant breed dogs and domestic shorthair cats (Table 14.14; De Risio & Platt, 2010). Median age in the dog is 5–6 years. The history usually includes a peracute nonprogressive myelopathy that is not painful after the first 24 hours. The lesion is an embolism in the intra-parenchymal spinal cord arteries of material chemically and histologically similar to the nucleus pulposus of intervertebral disks. Several theories have been proposed to explain how this happens. MRI is the preferred diagnostic tool and will demonstrate a focal spinal cord swelling.
Table 14.14 A summary of the significant diagnostic findings with fibrocartilaginous embolism
| Signalment | Large and giant breed dogs, 5–6 years old. Domestic shorthair cats | ![tab14.14.jpg]() |
| Clarity | Clear |
| Color | Possible xanthochromia |
| CSF TP | Mild increase |
| CSF cellularity | Mild to moderate neutrophilic pleocytosis |
| CNS cytology | Not commonly performed |
| Ancillary testing | Diagnosis made by imaging |
| Notes | Peracute history of severe pain/neurologic deficits that becomes pain free after 24 hours |
CSF analysis usually is employed to exclude other causes. CSF abnormalities are found in 45–75% of cases with FCE and include mildly elevated CSF TP, mild to moderate pleocytosis (TNCC = 7–84 cells/μl), and xanthochromia (De Risio & Platt, 2010).
Cystic lesions/hydrocephalus
Cystic structures are occasionally observed during imaging techniques of the neurologic patient (Table 14.15). Subarachnoid cysts are commonly seen in the dorsal subarachnoid space at the first or third cervical vertebrae of younger large breed dogs or caudal thoracic vertebrae of older small breed dogs (Skeen et al., 2003). These structures are typically an intradural outpouching of arachnoid membranes. They may communicate with the CSF (Gnirs et al., 2002).
Table 14.15 A summary of the significant diagnostic findings with cystic lesions and hydrocephalus
| Signalment | Various | ![tab14.15.jpg]() |
| Clarity | Clear |
| Color | Colorless |
| CSF TP | Within reference limits |
| CSF cellularity | Within reference limits |
| CNS cytology | Not commonly performed |
| Ancillary testing | Diagnosis made by imaging |
| Notes | Rarely, congenital malformations or neoplasms can produce cysts |
Hydrocephalus can be caused by obstruction of CSF flow, and can be classified as either internal (within the ventricular system) or external (within the subarachnoid space). The end result of both types of obstruction is the retention of CSF. CSF overproduction is very rarely a cause of hydrocephalus.
Neither of these lesions are truly cysts, in that they are not epithelial lined structures. Aspiration of the fluid areas in cases of subarachnoid cysts or hydrocephalus will produce material similar to normal CSF (Thomas, 1999; Gnirs et al., 2002).
Epidermoid cysts are typically seen in the fourth ventricle in the dog. They are true cysts, being lined by stratified squamous epithelium, and are filled with desquamated cells (Spoor et al., 2013). On cytology, epidermoid cysts have large aggregates of anucleate squamous epithelial cells, which could be mistaken for post-collection artifact of surface epidermal keratin. Epidermoid cysts are congenital lesions representing aberrant location of ectoderm in the neural tube. These structures may develop in the spinal cord and have been reported following spinal trauma or repeated CSF collection. If cysts also contain adnexal differentiation, they are termed dermoid cysts.
Rarely, meningeal carcinomatosis will produce cystic structures (Mateo et al., 2010). Samples from these tumors could contain neoplastic cells on cytologic evaluation of the CSF. Finally, the choroid plexus can form cysts that are either symptomatic or asymptomatic (Galano et al., 2002).
Lysosomal storage diseases
Lysosomal storage diseases are a group of congenital diseases caused by a metabolic deficiency in a catabolic pathway (Table 14.16; Miller & Zachary, 2017). Usually they are the result of a single gene deficiency. On a cellular basis this leads to an inability to break down a specific metabolite, which then builds up in the lysosomes. Typically, the patient presents early in life with a multitude of defects, both within and outside the CNS, depending on the type of lysosomal storage disease. Multiple types of storage disease occur, not all of which are expected to display neurologic effects. GM-1 and GM-2 gangliosidosis, ceroid lipofuscinosis, globoid cell leukodystrophy (Krabbe’s-like disease), mucopolysaccharidosis, and Neimann–Pick type C have been reported to involve the CNS of dogs and cats. Alpha mannosidosis is seen in the cat but has not yet been reported in the dog.
Table 14.16 A summary of the significant diagnostic findings with lysosomal storage diseases
| Signalment | Various breeds of dogs and cats. Typically younger | ![tab14.16.jpg]() |
| Clarity | Clear |
| Color | Colorless |
| CSF TP | Normal to mild increase |
| CSF cellularity | Purple to pink granules noted within cells |
| CNS cytology | Not commonly performed |
| Ancillary testing | Storage material observed in peripheral blood cells. Urine mucopolysaccharidosis screen. Testing for specific metabolite or genetic defect |
| Notes | Multiple forms, most with concurrent congenital malformations |
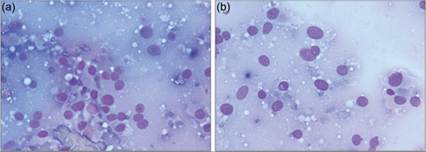
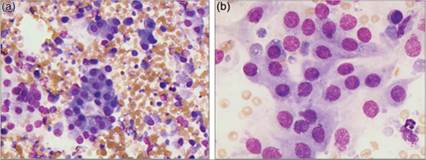
One of the defining cytologic findings of lysosomal storage diseases is an abundance of blue, metachromatic, or pink cytoplasmic material (Figures 14.35a, b, 14.36). This is found within the nervous tissue itself but can also be seen in the large mononuclear population in the CSF and peripheral blood. Special staining of the cells, including periodic acid–Schiff, T-blue, and Luxol fast blue, can be used. Urine oligosaccharide profiles can be used as a screening test. CSF and peripheral blood testing for the retained metabolite or genetic testing for the specific gene defect are commonly used to provide an antemortem diagnosis. Electron microscopy and special staining can be used on histologic samples.
![fig14.35A.jpg]()
Figures 14.35a, b CSF from an 8-month-old, spayed female Boston Terrier presenting for pain when jumping and not being active as a puppy. TNCC = 1 cell/μl, RBC = 300 cells/μl, CSF TP = 49.5 mg/dl. Most of the mononuclear cells had variably sized magenta granules, which often distended the nucleus (Wright–Giemsa, 1,000? magnification). A urine screening was positive for mucopolysaccharidosis. Further characterization of the genetic disorder was not attempted. (Courtesy Dr. Seung Yoo.)
![fig14.36.jpg]()
Figure 14.36 CSF from a 1-year-old, intact male Staffordshire Terrier with presenting complaints of ataxia, tetraparesis, and intermittent mental dullness. MRI changes were consistent with C2-C3 disk protrusion secondary to trauma or traumatic exacerbation of a congenital malformation. TNCC = 2 cells/μl, CSF TP = 64 mg/dl. Low numbers of large mononuclear cells (probably macrophages) are present. They have a small eccentrically placed round nucleus and abundant magenta cytoplasmic globular inclusions (Wright–Giemsa, 1,000? magnification). Further investigation showed strong positive mucopolysaccharidosis in urine and an underlying lysosomal storage disease was suspected. (Courtesy Dr. Laura Brandt.)
Neoplasia
Intracranial neoplasia has been reported in up to 3% of canine cases. In one series of 173 canine primary brain tumors, tumor types with the highest incidence included meningioma (45% of cases), astrocytoma (17%), oligodendroglioma (14%), choroid plexus tumors (7%), and primary CNS lymphoma (4%) (Snyder et al., 2006). Meningioma is the most common intracranial tumor reported in the cat. It accounted for 58.1% of feline primary intracranial tumors; lymphoma (14.4%), pituitary tumors (8.8%), astrocytoma (2.8%), and oligodendroglioma (2.4%) made up the other more populated categories in a series of 160 cats (Troxel et al., 2003). Metastasis and direct extension of extracranial neoplasms occurred in only 5% and 4% of feline intracranial neoplasm cases, respectively. Meningioma is the most common primary spinal cord lesion in the dog (Jose-Lopez et al., 2013). Other primary tumor types rarely found in the CNS of the dog and cat include primitive neuroectodermal tumors, glioblastomas, olfactory neuroblastomas, histiocytic sarcomas, and vascular tumors (Figures 14.37a, b).
![fig14.37A.jpg]()
Figures 14.37a,b CNS cytology from a dog. (a) A neoplastic population of neurons. The cells resemble large pyramidal cells found in the cerebellum with many ruptured cells present (Wright–Giemsa, 500? magnification). (b) Where the cells are well intact, they are roughly triangular with basophilic faintly granular cytoplasm, a large eccentrically located ovoid nucleus with stippled chromatin and single large distinct nucleolus. This morphology is suggestive of a ganglioneuroma (Wright–Giemsa, 1,000? magnification). The cytologic diagnosis was confirmed by histopathology.
Neoplasia is commonly associated with a neutrophilic pleocytosis or increased neutrophil percentage. However, a neutrophilic pleocytosis should not always be expected. One theory to explain the lack of pleocytosis states that some tumor locations are distant enough from the site of sampling or deep enough to prevent significant cellular shedding into the collected CSF. In a series of meningiomas, tumors in the caudal portion of the cranial fossa had higher cell counts, while those in more rostral locations commonly had lower counts (Dickinson et al., 2006). Necrosis inducing inflammation has been used to explain neutrophilic pleocytosis associated with neoplasia; it could also be posited that less necrotic lesions would result in fewer neutrophils being present.
Patients with intracranial tumors are commonly presented when the owner notices a neurologic defect. Often the neurologic defects are the result of the space-occupying effects of the mass on surrounding tissue and not a primary effect of the tumor. A thorough neurologic examination is recommended to localize the lesion. In human medicine, lesion localization is commonly used to narrow down the differential list prior to cytologic evaluation (Powell, 2005). Similarly, lesion location and other magnetic resonance imaging features in dogs may help to prioritize likely differentials for intracranial tumors (Miller et al., 2019b).
Meningiomas account for 45% and 85% of primary intracranial tumors and 22.3% and 59% of all intracranial tumors in dogs and cats, respectively (Table 14.17; Motta et al., 2012). There is a breed predilection in Boxers and dolichocephalic breeds, including German Shepherd Dogs, Golden Retrievers, and Labrador Retrievers. Meningiomas seem more common in domestic shorthair cats. Most canine cases are over 7 years old at diagnosis and most cats are over 9 years old.
Table 14.17 A summary of the significant diagnostic findings with meningioma
| Signalment | Boxers, German Shepherd Dogs, Golden Retrievers, Labrador Retrievers. Domestic shorthair cats | ![tab14.17.jpg]() |
| Clarity | Clear |
| Color | Colorless |
| CSF TP | Possible increase |
| CSF cellularity | Normal to moderate neutrophilic pleocytosis. |
| | Rarely, neoplastic cells seen |
| Lesion location | Intradural, extramedullary. Dog: olfactory, frontal, suprasellar, parasellar region, optic chiasm, cervical spinal cord. Cat: 3rd ventricle, supratentorial and cerebellar meninges |
| CNS cytology | Moderately-sized cohesive cells, intranuclear cytoplasmic inclusions, folded nuclei |
| Ancillary testing | Positive: CD-18, actin. Negative: S-100, CD3, CD79a, PAX5, cytokeratin, GFAP |
| Notes | Multiple histologic types described |
Meningioma
Meningiomas are intradural and extramedullary lesions. In the dog they are commonly diagnosed in the olfactory/frontal region, optic chiasm, suprasellar and parasellar regions, or cervical spinal cord. In the cat, the most common locations include the tela choroidea of the third ventricle, the supratentorial meninges, and the cerebellar meninges. Concurrent meningioma and another intracranial neoplasm were found in 13.9% of feline and 19% of canine meningioma patients (Motta et al., 2012).
The most recent veterinary classification system of meningiomas describes nine variants (Koestner et al., 1999). These include benign, slow growing tumors (including meningothelial, fibroblastic, transitional, psammomatous, angiomatous, papillary, granular, and myxoid subtypes) and more aggressive anaplastic tumors. However, multiple case reports and veterinary texts describe histologic subtypes not included in this classification. Tumor grading following the more recent WHO classification for central nervous system tumors has also been proposed (Belluco et al., 2022). In both the human and veterinary classification systems, meningiomas are graded into three histologic grades (I–III; or benign, atypical, and anaplastic). Classification and grading of meningiomas has prognostic value in human medicine, although the prognostic significance of grade or subtype of meningiomas in veterinary medicine is still uncertain (Jose-Lopez et al., 2013). Recommendations for standardization of canine meningioma grading have recently been proposed to improve intra-observer agreement (Belluco et al., 2022). Metastasis has been reported in the dog and cat but does not appear common.
Although it has been reported that meningiomas often have a neutrophilic pleocytosis, multiple retrospective studies report that the majority of cases had a TNCC (Harms et al., 2009). Intranuclear cytoplasmic pseudoinclusions are round basophilic vacuolated intranuclear structures, which appear to be a bleb of cytoplasm within the nucleus. They have been found in normal hepatocytes, meningiomas, Leydig cell tumors, melanomas, and papillary thyroid carcinomas, among others. Papanicolaou staining may help highlight these inclusions, but they have been reported with Wright–Giemsa staining alone.
![fig14.38A-E.jpg]()
Figures 14.38a–e Aspirate of a mass in the forebrain of a dog. (a) Sheets of cohesively clustered polygonal cells with moderate amounts of basophilic cytoplasm and round to ovoid nuclei are present (Wright–Giemsa, 1,000? magnification). (b) Note the minimal to moderate anisocytosis and anisokaryosis in the cell population (Wright–Giemsa, 1,000? magnification). (c) Hematoidin crystals and aggregates of blue–black granular material (likely hemosiderin) are present and suggest chronic hemorrhage (Wright–Giemsa, 500? magnification). (d) Several areas of the slide had increased numbers of nondegenerate neutrophils and cellular debris (Wright–Giemsa, 500? magnification). (e) The pink extracellular felt-like material is a dense aggregate of neuropil. Nuclei of glial cells are present within the neuropil (Wright–Giemsa, 1,000? magnification).
![fig14.39A-C.jpg]()
Figures 14.39a–c CNS cytology from a dog. (a) Large aggregates of spindloid cells are present. (b) Nucleoli are round with granular chromatin and poorly distinct nucleoli. (c) There is a lack of vasculature; however, minimal pink fibrillar extracellular material is present (Wright–Giemsa, 500? magnification).
Neoplastic cells do not appear to be a common finding in CSF samples but have been reported; the presence of neoplastic cells may be related to the location of the primary lesion (Harms et al., 2009). When present, meningiomas appear as aggregated and individualized cells with moderate amounts of basophilic, finely granulated cytoplasm, a paranuclear clear zone, round to oval nuclei, finely stippled chromatin, indistinct nucleoli, and rare erythrophagocytosis. Most cells are polygonal, although rare spindloid cells can be present.
Cytologically, distinction of the subtypes of meningioma is often not possible. However, occasional whorling arrangements of epithelial-like cells around a central hyalinized necrotic mineral core (psammoma body) suggest a psammomatous meningioma, and spindle cells in a storiform pattern can suggest a fibroblastic meningioma (Motta et al., 2012). The presence of magenta cytoplasmic granules within neoplastic meningeal cells may support a granular-type meningioma (Figure 14.41).
![fig14.40A.jpg]()
Figures 14.40a,b Imprint of a mass from a mixed breed dog. Dense aggregates of pleomorphic meningeal cells are present, which have poorly distinct cell borders that give the impression of a spindloid cell, ovoid nucleoli, and, where visible, a poorly distinct single nucleolus (Wright–Giemsa, 500? magnification).
![fig14.41.jpg]()
Figure 14.41 Imprint of an intradural extramedullary mass extending from L4 to the caudal aspect of L5 in an 8-year-old spayed female domestic shorthair cat. Dense aggregates of meningeal cells are present which are polygonal to spindloid in shape with uniform round to oval nuclei and moderate amounts of pale basophilic cytoplasm containing bright magenta granulation. Aggregates of cells are closely associated with copious amounts of bright pink extracellular matrix material. Histopathologic evaluation confirmed a granular-type meningioma with coexpression of cytokeratin and vimentin (Wright–Giemsa, 500? magnification).
There is a reported overlap of morphologies between meningiomas and astrocytomas; both can appear as spindloid cells and they have been grouped in some studies (Platt et al., 2002). Meningiomas should stain positive with patchy areas for CD-18 and actin. They should also be negative for S-100, lymphoid markers, cytokeratin, and glial fibrillary acidic protein (GFAP).
Astrocytoma
In the dog, Boxers and Boston Terriers are more likely to have astrocytomas (Table 14.18; Figures 14.42a, b; Snyder et al., 2006). Astrocytomas make up about 17% of intracranial tumors in the dog and 2.8% of intracranial tumors in the cat. They are commonly found in the telencephalon, diencephalon, and cerebellum and are intra-axial lesions (Lee & Tihan, 2015).
Table 14.18 A summary of the significant diagnostic findings with astrocytoma
| Signalment | Boxers, Boston Terriers | ![tab14.18.jpg]() |
| Clarity | Clear |
| Color | Colorless |
| CSF TP | Possible increase |
| CSF cellularity | Normal to moderate neutrophilic pleocytosis. Rarely, can find neoplastic cells which look similar to monocytes |
| Lesion location | Intra-axial. Telencephalon, diencephalon, cerebellum |
| CNS cytology | Elongate tumor cells arranged around thin-walled vessels |
| Ancillary testing | Positive: vimentin, S-100, GFAP |
| Notes | Can look like monocyte/macrophage or meningioma on cytology |
![fig14.42A.jpg]()
Figures 14.42a,b Tissue from a 10-year-old, neutered male Boxer with a 1-day history of seizures. On necropsy a red mass was present in the base of the left piriform lobe. (a) The neoplastic cells have scant cytoplasm and abundant fibrillary processes. Several areas of hemorrhage and pseudopalisading around necrotic areas are present along the left side of the image (H&E, 200? magnification). (b) A closer image (500? magnificaion) helps to demonstrate the fibrillary processes (upper left) and an area of hemorrhage (lower right). The amount of hemorrhage is not uncommon; it imparted a red color to the lesion grossly. Diagnosis of this mass was a fibrous astrocytoma. (Case courtesy Dr. Greta Krafsur.)
Smears of astrocytomas are slightly more cellular than normal brain. In keeping with the astrocyte’s role of providing nutritional support to neurons and forming part of the blood–brain barrier, astrocytomas typically have thin-walled, demarcated, and branching blood vessels with streams of elongate tumor cells radiating from the vessel margins and possessing long, thin cytoplasmic processes (Vernau et al., 2001). Their cytoplasm is faintly eosinophilic with an extensive network of randomly criss-crossing eosinophilic fibrillary cytoplasmic processes. Cytologically, low-grade astrocytomas on CSF have been described as appearing similar to histiocytes, monocytes, or foamy macrophages. Astrocytomas are vimentin, S-100, and GFAP positive (Cantile & Youssef, 2015).
Oligodendroglioma
Oligodendrogliomas have been reported in older domestic shorthair and Maine Coon cats, with a mean age of 9 years (Table 14.19; Troxel et al., 2003). In dogs, Boxers and Boston Terriers are more likely to have oligodendrogliomas (Snyder et al., 2006). They make up approximately 2.4% of intracranial tumors in the cat and 14% of intra-cranial tumors in the dog. These tumors are often located in the temporal lobe or prosencephalon as intra-axial lesions.
Table 14.19 A summary of the significant diagnostic findings with oligodendroglioma
| Signalment | Boxers, Boston Terriers. Domestic shorthair and Maine Coon cats | ![tab14.19.jpg]() |
| Clarity | Clear |
| Color | Colorless |
| CSF TP | Possible increase |
| CSF cellularity | Normal to moderate neutrophilic pleocytosis. Rarely, can find neoplastic cells, which are large round cells with abundant cytoplasm and globular projections |
| Lesion location | Intra-axial. Temporal lobe, prosencephalon |
| CNS cytology | Honeycombed, glomerular tufts of capillaries, tightly packed cells with fine granular chromatin. Mucoid material common |
| Ancillary testing | Negative: cytokeratin, GFAP |
| Notes | Mass is grossly gelatinous/mucoid |
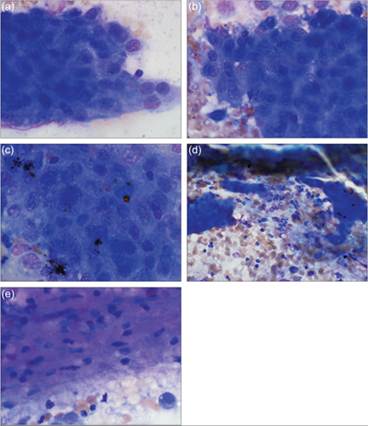
Oligodendrocytes are glial cells responsible for myelination of neurons. As such, they have a soft, gelatinous to mucoid texture that can be appreciated during smear preparation and have a honeycombed appearance on histopathology (Figures 14.43a–d; Vernau et al., 2001). Many vascular structures with glomeruloid capillary tufts are observed in these tumors. Cytology smears are often highly cellular, with many closely packed cells that have a round nucleus and fine, granular chromatin. When present, nucleoli are small and single. This morphology does not appear to be retained in fluid preparations. When they are visible on cytologic preparations of CSF, oligodendrogliomas have been described as large cells with a round nucleus and abundant deeply basophilic cytoplasm, which often have globular projections (Dickinson et al., 2000). Rare neoplastic cells in pairs or aggregates and occasional mitotic figures have been noted. Oligodendrogliomas are GFAP negative (Cantile & Youssef, 2015).
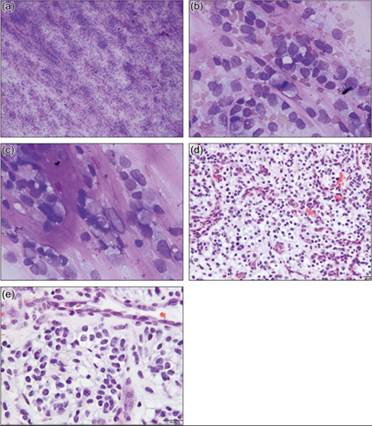
![fig14.43A-E.jpg]()
Figures 14.43a–e Canine oligodendroglioma. (a) The specimen is highly cellular and has many branching capillaries and abundant pink extracellular material. Cells are sometimes arranged in linear arrays separated by strands of extracellular material (Wright–Giemsa, 100? magnification). (b) Nucleated cells are predominantly round cells that have large, variably shaped nuclei and a moderate amount of pale gray–blue cytoplasm. Anisocytosis and anisokaryosis are mild. The nuclei have stippled chromatin and usually lack appreciable nucleoli. The cytoplasm often has low to moderate numbers of small clear vacuoles and/or a small amount of very fine pink granular material. Thin strands of pink extracellular matrix material separate neoplastic cells. (c) Extracellular matrix material may also more abundant, forming thick branching structures (Wright–Giemsa, 500? magnification). (a–c courtesy Dr. Sara Connolly.) (d) Neoplastic cells have hyperchromatic round nuclei with moderate atypia, rare mitoses, pale eosinophilic to vacuolated cytoplasm, and distinct cellular borders. There is pronounced microvascular proliferation (H&E, 200? magnification). (e) Higher magnification of the neoplastic population illustrating mitotic figures and microvascular proliferation (H&E, 400? magnification). (c, d courtesy Dr. J. M. Jankovsky.)
Ependymoma
Ependymoma is rarely seen. Several cases have been well described (Rand et al., 1994b; Vernau et al., 2001; Vural et al., 2006; Traslavina et al., 2013; Woolford et al., 2013; Gibson et al., 2021). The mean age in a group of 18 cats with ependymoma was 9 years; a clear breed predisposition was not evident (Table 14.20). Ependymomas in dogs have a less predictable age distribution and may affect young to middle-aged dogs. These tumors tend to arise in the lateral, third, or fourth ventricle and form an intraventricular mass when intracranial but may also originate from the spinal cord (Pancotto et al., 2013; Miller et al., 2019a; Gibson et al., 2021). They are typically well-demarcated lesions.
Table 14.20 A summary of the significant diagnostic findings with ependymoma
| Signalment | Dog and cat | ![tab14.20.jpg]() |
| Clarity | Clear |
| Color | Colorless |
| CSF TP | Possible increase |
| CSF cellularity | Normal to moderate neutrophilic pleocytosis. Rarely, neoplastic cells seen |
| Lesion location | Intraventricular or spinal cord |
| CNS cytology | Ciliated columnar cells with pseudorosette and true rosette formation |
| Ancillary testing | Cat: positive GFAP. Dog: equivocal GFAP |
| Notes | Confirm cilia on electron microscopy if needed |
Ependymomas have been reported to smear easily on cytologic preparation (Vernau et al., 2001). One case affecting the spinal cord of a dog exfoliated for fine needle aspiration (Gibson et al., 2021). Consistent, but not pathognomonic, histologic and cytologic features of ependymomas are branching papillary structures, pseudorosettes, and true rosette formations (Figures 14.44a, b; Woolford et al., 2013). Pseudorosettes are palisading layers of ependymal cells with their ependymal processes facing inward around a blood vessel. A true rosette is a tubular formation of ependymal cells around an empty cavity. Nuclei are eccentrically placed, round to ovoid, and have a cribriform chromatin pattern. The cytoplasm is eosinophilic with distinct borders. Necrotic cells seem to be a common feature. Ultrastructural demonstration of cilia can help confirm a diagnosis of ependymoma (Cheville, 2009). These tumors should stain positive for GFAP in the cat. GFAP staining appears inconsistent in the dog; most documented cases are GFAP negative, although GFAP staining within pseudorosettes and/or rosettes has been reported in canine ependymomas (Cantile & Youssef, 2015; Miller et al., 2019a).
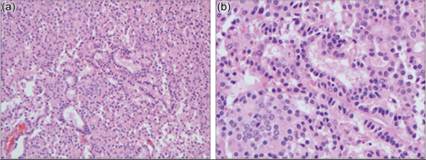
![fig14.44A.jpg]()
Figures 14.44a,b Feline ependymoma. (a) Histologically, there is a population of large cuboidal to columnar cells. Several true rosettes (cells arranged around an open space) and pseudorosettes (cells arranged around a blood vessel) are present (H&E, 200? magnification). (b) A close-up image of branching tubular structures. Note the barely discernible ciliated apical surface of the columnar cells lining the tubules (H&E, 500? magnification). (Case courtesy Dr. Sushan Han.)
Choroid plexus tumors
Choroid plexus tumors in the dog make up approximately 7–10% of all primary intracranial CNS tumors, but they are only rarely found in the cat (Table 14.21). The masses arise from choroid plexus epithelium found in the lateral, third, and fourth ventricles or the lateral apertures and are the most common tumors found in an intraventricular location (Westworth et al., 2008; Miller et al., 2019b). Both choroid plexus papillomas and choroid plexus carcinomas have been described, with more cases being carcinomas than papillomas (64% and 36%, respectively). Choroid plexus tumors commonly occur in middle-aged dogs, with a mean age of 6 years. Golden Retrievers may be overrepresented.
Table 14.21 A summary of the significant diagnostic findings with choroid plexus tumors
| Signalment | Golden Retrievers, 6 years old. Rare in cats | ![tab14.21.jpg]() |
| Clarity | Clear |
| Color | Colorless |
| CSF TP | Possible increase |
| CSF cellularity | Normal to moderate neutrophilic pleocytosis One-half of cases have neoplastic cells: moderately-sized cells, abundant granular cytoplasm, oval nuclei, and irregular nucleoli |
| Lesion location | Intraventricular. Lateral, 3rd, 4th ventricle |
| CNS cytology | Papillary and medusoid-shaped fronds, sheets and clusters of columnar cells with basal nuclei |
| Ancillary testing | Positive: cytokeratin and GFAP |
| Notes | Carcinomas may have more anisokaryosis |
On intraoperative cytology, choroid plexus tumors are grossly soft and friable and spread easily into smears (Figures 14.45a, b; Vernau et al., 2001). They have abundant blood vessels, which often branch into papillary and medusoid-shaped fronds. There are large numbers of cells in sheets and clusters. Occasionally, cells are individualized. When in sheets and clusters, the epithelial cells are columnar with a basally located nucleus. The individualized cells are small with plentiful eosinophilic cytoplasm that does not form extended processes. Nuclei are round to ovoid with finely granular chromatin, a dark-staining nuclear border, and one or more prominent nucleoli. Carcinomas have been reported to display more prominent anisokaryosis, but were otherwise similar to papillomas.
![fig14.45A.jpg]()
Figures 14.45a,b Cytology from an extra-axial mass in the area of the 4th ventricle with involvement of the vermis, brainstem, and pons of an 8-year-old English Bulldog. (a) Large cohesive clusters of cells are present and are associated with abundant red blood cells (Wright–Giemsa, 500? magnification). (b) Polygonal to elongate cells with lightly basophilic cytoplasm and a round nucleus are present. There is minimal anisocytosis and anisokaryosis (Wright–Giemsa, 1,000? magnification). Histologic evaluation confirmed the tissue was from the choroid plexus and suggested it was a papilloma.
Reports in the veterinary literature suggest that choroid plexus cells should be cytokeratin positive and GFAP negative (Cantile & Youssef, 2015). Interestingly, human choroid plexus cells are positive for vimentin as well as cytokeratin and are GFAP negative (Sarnat, 1998).
There is the suggestion that the CSF TP content is higher in choroid carcinomas than papillomas: median 108 mg/dl compared with 34 mg/dl, respectively (Westworth et al., 2008). Neoplastic cells are found in the CSF of approximately half of the cases. Choroid plexus carcinomas have been described as moderately sized cells, with abundant slightly granular, vacuolated, and basophilic cytoplasm and round to oval nuclei with coarse chromatin and irregular nucleoli (Pastorello et al., 2010). Occasional mitotic figures are also seen. Intraventricular or subarachnoid metastasis has been noted on MRI and can help to support the malignant nature of choroid plexus tumors (Westworth et al., 2008). A case of a choroid plexus papilloma and concurrent meningioma has been reported in a 7-year-old female English Cocker Spaniel (Espino et al., 2009).
Primary CNS lymphoma has been described in both dogs and cats (Table 14.22). Retrospective studies suggest that it is more common in the cat than the dog, although both are at a low incidence rate (Troxel et al., 2003; Snyder et al., 2006). CNS lymphoma is more likely to be a component of multicentric lymphoma than a primary disease; only eight of 23 (34.8%) cats with intracranial lymphoma had primary CNS lymphoma. In cats, diffuse cerebral or brainstem involvement on MRI was predictive of lymphoma (Troxel et al., 2003). Both T- and B-cell primary CNS lymphomas have been described in the dog and cat; most cases tend to be T-cell in origin (Koestner et al., 1999), although a retrospective study involving mostly FeLV+ cats showed a B-cell predominance (Mello et al., 2019). In humans, a quarter of human immunodeficiency virus-positive patients with neurologic signs have primary CNS lymphoma. A specific association between feline immunodeficiency virus and primary CNS lymphoma has not been found.
Table 14.22 A summary of the significant diagnostic findings with primary CNS lymphoma
| Signalment | Dog and cat | ![tab14.22.jpg]() |
| Clarity | Clear |
| Color | Colorless |
| CSF TP | Moderate increase |
| CSF cellularity | Mild pleocytosis, most commonly mononuclear or mixed. Possible neoplastic lymphocytes |
| Lesion location | Diffuse or mass lesion. Diffuse cerebral or brainstem involvement on MRI is predictive |
| CNS cytology | Discrete cells with minimal cytoplasm and high N:C ratio |
| Ancillary testing | Immunocytochemistry or immunohistochemistry. PARR, or flow cytometry may be a low yield test |
| Notes | More commonly is component of multicentric lymphoma |
Primary central nervous system lymphoma
On intraoperative smear preparations there are few prominent and branched vessels, with many individualized round cells morphologically similar to lymphomatous cells noted elsewhere in the body (Vernau et al., 2001; Lee & Tihan, 2015). Primary CNS lymphoma can produce cytologic smears that are highly cellular with an angiocentric arrangement. The smears can often be devoid of intermingled brain tissue.
Given how highly exfoliative lymphoma is elsewhere in the body, it would be expected that lymphoma would be easily detected on CSF cytology. However, lymphoma was diagnosed on CSF cytology in only 20% of cats with confirmed intracranial or spinal lymphoma in a recent study (Durand et al., 2022). This is consistent with previous studies that showed CS Flymphoma to be poorly exfoliative in the CSF for both cats and dogs (Troxel et al., 2003; LaRue et al., 2018). 65% of cats in the Durand study had a mild pleocytosis without overtly neoplastic cells (median TNCC = 16.5 cells/ μl) with mononuclear or mixed pleocytosis being most common. A concurrent increase in total protein is another commonly reported finding, with mean values ranging from 54.5 to 93 mg/dL across retrospective studies (Troxel et al., 2003; Durand et al., 2022).
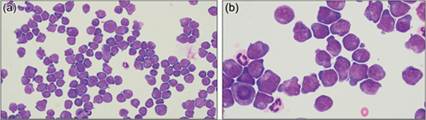
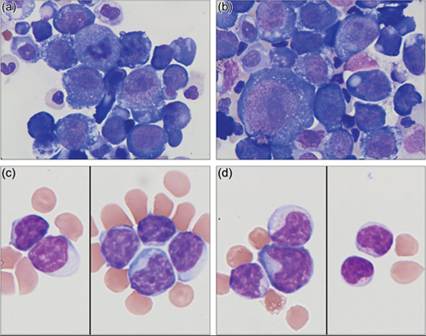
As with lymphoma elsewhere in the body, neoplastic lymphocytes are easiest to detect cytologically when they present with typical lymphoid nuclear to cytoplasmic ratio, deeply basophilic cytoplasm, and large round nuclei with nucleoli (Figures 14.46a, b). They can also present as less pleomorphic small cells, granular lymphocytes, or highly pleomorphic cells that do not resemble lymphocytes at all (Figures 14.47a–d; Fernandez et al., 2013).
![fig14.46A.jpg]()
Figures 14.46a,b CSF from a dog, TNCC and TP unavailable. (a) There is a population of individualized round cells with a high nuclear to cytoplasmic ratio. Nuclei appear round to slightly indented with finely stippled chromatin. Cytoplasm is deeply basophilic and often contains a zone of perinuclear cytoplasmic clearing. These cells measure 1.5–2? the diameter of a neutrophil, consistent with a large-cell lymphoma. The cells were CD3+ and CD79a- on immunocytochemistry, which confirmed the diagnosis of T-cell lymphoma (Wright–Giemsa, 500? magnification). (b) Closer evaluation reveals one to multiple prominent nucleoli per nucleus. Rare cells contain cleaved nuclei. Note the mitotic figure at the bottom right of the image (Wright–Giemsa, 1,000? magnification).
![fig14.47A-D.jpg]()
Figures 14.47a–d Cytomorphology in CNS lymphoma can also be variable. CSF from a 9-year-old Boxer. TNCC = 4,200 cells/μl, CSF TP = 330 mg/dl (a, b); CSF from a 10-year-old mixed breed dog with diffuse lesions in the CNS on MRI. TNCC = 13 cells/μl, CSF TP = 149 mg/dl (c, d). (a) There is a pleomorphic population of large mononuclear cells that have minimal amounts of deeply basophilic cytoplasm, round nucleus, stippled chromatin, and one to several prominent nucleoli. Note the mitotic figure in the upper center of the image. (b) The neoplastic cells occasionally have clear cytoplasmic vacuoles (right side of image). The cytomegalic cell in the lower left corner has an oblong nucleolus, which is larger than the adjacent small mononuclear cell (Wright–Giemsa, 1,000? magnification). Flow cytometry was requested but could not be performed. PCR for lymphoma found a clonal rearrangement of the T-cell receptor, supporting a diagnosis of T-cell lymphoma. (c) The predominant cell type is small mononuclear cells, which have minimal amounts of basophilic cytoplasm and a round to indented nucleus with clumped chromatin. Nuclei measure approximately 1.5 times the size of a red blood cell. The morphology is most suggestive of a small to intermediate-sized lymphocyte. (d) Most of these cells had few small pink cytoplasmic granules located beside the nucleus. The large number of granulated lymphocytes was interpreted as evidence of lymphoma (Wright–Giemsa, 1,000? magnification).
Flow cytometry and PCR for antigen receptor rearrangements (PARR) in lymphocytes to support a diagnosis of lymphoma can be used on dog and cat CSF samples. Based on anecdotal experiences and well-established facts from analysis outside the CNS, several limitations to the technique should be recognized. Flow cytometry studies require a fairly large number of viable cells for evaluation. One human study found that a full flow cytometry evaluation had higher likelihood of being inconclusive when CSF cellularity was located. Bright pink cytoplasmic granules are prominent, along with variably distinct cytoplasmic vacuolation. Significant anisocytosis and mild to moderate anisokaryosis are present (Wright–Giemsa, 500? magnification).
Metastatic and invasive neoplasia
Metastatic neoplasia to the CNS is fairly common, occurring in up to 8.8% of extra-neural malignant neoplasms in one study (Heck et al., 2018). Most often these tumors look cytologically similar to their appearance outside the nervous system.
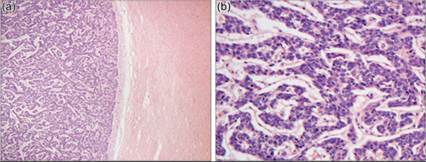
Carcinomas of mammary, intestinal, urothelial, prostatic, and cutaneous squamous cell origin have produced meningeal carcinomatosis in dogs (Figures 14.49a, b; Mateo et al., 2010; Pancotto et al., 2013). Metastatic hemangiosarcoma, lymphoma, melanoma, and less commonly osteosarcoma or histiocytic sarcoma have also been described in dogs (Heck et al., 2018).
![fig14.49A.jpg]()
Figures 14.49a,b Cortex, metastatic mammary tumor. (a) The neoplastic tissue (left) compresses the adjacent nervous tissue (right). This mass-effect on normal tissue is the most common cause of clinical signs (H&E, 50? magnification). (b) At higher power, neoplastic epithelial cells form ribbons and indistinct tubular structures reminiscent of normal mammary gland (H&E, 200? magnification). (Case courtesy Dr. Paula Schaffer.)
Lymphoma and osteosarcoma are the most common forms of metastatic spinal neoplasia in the cat (Marioni-Henry, 2010). These are also relatively common differentials for feline intracranial metastatic tumors; others include pulmonary adenocarcinoma, squamous cell carcinoma, fibrosarcoma, hemangiosarcoma, myxosarcoma, pleomorphic or unclassified sarcoma, and unclassified carcinoma (Troxel et al., 2003).
Several tumors arising from locations outside the CNS may impinge on or invade neural tissue, including vertebral osteosarcomas or nasal tumors (Cantile & Youssef, 2015). Cytologic evaluation of these lesions should not involve intentional sampling of the CNS, although evidence of neural tissue may rarely be identified incidentally or during post-mortem examination (Figure 14.50a–c).
![fig14.50A-C.jpg]()
Figures 14.50a–c Post-mortem FNA of a right mandibular mass in a 14-year-old spayed female Bichon Frise with a history of oral squamous cell carcinoma. MRI revealed lysis of the right mandible and calvarium with extension of the mass into the cerebral cortex. (a) Cohesive clusters of rounded to polygonal squamous epithelial cells are present, which often contain many punctate, perinuclear cytoplasmic vacuoles. Moderate to marked anisocytosis and anisokaryosis, dyskeratosis, prominent and variably sized nucleoli, and occasional binucleation or multinucleation support a squamous cell carcinoma (Wright–Giemsa, 500? magnification). (b) Areas of the same slide contain frothy, pink to purple extracellular material with embedded nuclei and pale-pink ribbon-like structures, compatible with neuropil (Wright–Giemsa, 200? magnification). (c) Individualized and clustered malignant squamous epithelial cells are closely associated with aggregates of neuropil. The cytologic features supported the MRI findings of tumor extension into the cerebrum (Wright–Giemsa, 200? magnification).