Pulmonary ventilation
Respiration, the process of gas exchange, occurs in three steps:
1. Pulmonary ventilation, or breathing, is the mechanical movement of air into (inspiration) and out (expiration) of the lungs.
2. External respiration is the exchange of gases between the lungs and the pulmonary capillaries, which occurs across the respiratory membrane. The blood gains O2 and loses CO2.
3. Internal respiration is the exchange of gases between systemic capillaries and tissue. The blood gains CO2 and loses O2.
Pressure changes during respiration
Inspiration
Boyle's law states that at constant temperature and pressure, there is an inverse relationship between the volume and pressure of a gas:
where P is the pressure of the gas (mL of Hg), and V is the volume (cm3). Therefore, the pressure inside a closed container will decrease as the volume of the container increases, and vice versa. When this law is applied to the lungs, we find that the pressure inside the lungs decreases as the volume of the lungs increases. Air moves into the lungs as a result of a decrease in air pressure within the lungs.
In most animals, inspiration is an active process. The main muscles responsible for quiet inhalation are the diaphragm and the external intercostal muscles. The diaphragm is a dome-shaped muscle innervated by the phrenic nerves. As the diaphragm contracts, it increases the horizontal dimensions of the thoracic cavity, thus increasing the volume of the thorax. This causes the volume of the lungs to expand and thereby decreases the pressure inside the lungs. This results in inspiration.
Contraction of the external intercostal muscles causes the ribs to move Cranially and ventrally, thus increasing the diameter of the thorax.
This accounts for about 25% of the entry of air into the lungs.In a horse at rest, the intrapleural pressure is negative, about 754 mmHg. As inspiration begins, this pressure drops to approximately 744 mmHg. Atmospheric pressure is 760 mmHg at sea level. As the volume of the thoracic cavity increases during inspiration, the parietal pleura is pulled outward, and the visceral pleura is pulled with it. As a result, the pressure inside the lungs, the alveolar pressure, decreases. Air then flows from an area of high pressure (the atmosphere) to an area of lower pressure (the alveoli).
As an animal increases the force of inspiration, additional muscles are engaged. These include the sternocleidomastoid muscles that move the sternum rostrally, the scalene muscles that pull the first two ribs forward, and the pectoralis minor muscles that pull several other ribs forward.
Expiration
Normal expiration is a passive process involving no active muscle contraction. Like inspiration, it is due to pressure gradients, but in an opposite direction. Because of the elastic recoil of the lungs and chest wall, there are two inwardly directed forces resulting in this recoil: (1) the elastic fibers that were stretched during inhalation and (2) the inwardly directed force due to the surface tension arising from the alveolar fluid.
As the neural signals to the diaphragm cease, it relaxes and this dome-shaped muscle moves rostrally, thus decreasing the volume of the thoracic cavity. The external intercostals also relax and allow the ribs to move dorsally and caudally, thus further decreasing the volume of the thoracic cavity. This decreases lung volume and causes alveolar pressure to increase approximately 2 mmHg above atmospheric pressure. As a result, air flows out of the lungs to an area of lower pressure.
During forceful exhalation, the abdominal and internal intercostal muscles contract. This causes the ribs to move caudally and dorsally compressing the abdominal viscera and decreasing the thoracic volume.
This increases pressure inside the thoracic cavity and forces air outward.Other factors involved in pulmonary ventilation
Surface tension of alveolar fluid
Alveolar fluid coats the inside surface of the alveoli. Because of hydrogen bonding, this fluid has a surface
Box 14.2 Surfactant production in premature infants
Premature infants are at risk for respiratory distress syndrome. This is due to the lack of surfactant production, which does not line the alveolar walls until near parturition. The National Institutes of Health recommends broad use of maternal glucocorticoid therapy to stimulate surfactant production in the fetus. In addition, surfactant replacement therapy is recommended in low birth weight immature infants. The preterm lamb is often used as a model for investigating the effects of glucocorticoids on surfactant production and its effects on postnatal development (see Ikegami et al., 1997).
tension. In a sphere such as that found in the alveoli, this surface tension produces an inwardly directed force causing the alveoli to assume the smallest possible diameter. In order to expand the lungs, this surface tension must be exceeded. This surface tension accounts for approximately two-thirds of the lung's elastic recoil.
Surfactant, produced by type II alveolar cells, is a complex of lipids and proteins that reduces the surface tension in much the same way the soap allows lipids to dissolve in aqueous solutions. Since surfactant is one of the last compounds produced during embryonic development, premature animals often have respiratory distress as a result of the underdeveloped respiratory system. In the case of sheep, surfactant is released into the alveolar spaces near the beginning of the fourth month of gestation. Its release correlates with a rise in plasma cortisol levels (Box 14.2).
Compliance of the lungs
The distensibility of the lungs is referred to as lung compliance. High lung compliance means that the lungs will expand easily.
Lung compliance is related to (1) the distensibility of lung tissue and the thoracic cage, and (2) alveolar surface tension. Lung compliance is normally high due to the elasticity of the lung's tissue and decreased alveolar surface tension from surfactant.Compliance can be decreased by several factors: (1) scar tissue formed in the lungs as a result of certain diseases, (2) pulmonary edema resulting from accumulation of fluid in the lungs, (3) insufficiency of surfactant, and (4) decrease in the ability of the thoracic cage to expand.
Airway resistance
The flow of air into the lungs is inversely related to airway resistance:
F = ^.
R
where F is gas flow, P is pressure, and R is resistance. The walls of the airways into the alveoli, particularly the bronchioles, create resistance to airflow. The larger the diameter of the airway, the less the resistance to airflow. The diameter of the airways can be altered by the degree of contraction of the smooth muscle in these airways. Stimulation of the sympathetic nervous system causes relaxation of these walls, which allows air to more readily enter the lungs. Diseases or injuries to the airways can increase airway resistance.
During exercise, animals decrease the airway resistance by dilating the external nares and vasoconstriction of the vascular tissue in the nose. As exercise rate increases, cows and dogs breathe through their mouth in order to bypass the greater airway resistance associated with the nose. However, horses are considered obligate nose breathers and must rely on their ability to decrease airway resistance in order to increase airflow. One can watch the nostrils of a horse flare during exercise (Box 14.3).
Box 14.3 Airway obstruction in short-nosed dogs
The term brachycephalic, or brachiocephalic, means short-nosed and refers to dogs with short muzzles, noses, and mouths. Brachycephalic airway obstruction syndrome (BAOS), also called brachycephalic airway disease (BAD) and brachycephalic airway syndrome (BAS), is an inherited condition in the Cavalier King Charles spaniel, English bulldog, pug, Boston terrier, and Pekingese, in particular.
The throat and breathing passages in brachycephalic dogs often are undersized or flattened.The symptoms of this disorder typically include labored and constant open-mouthed breathing, noisy breathing, snuffling, snorting, excessive snoring, gagging, retching, exercise and/or heat intolerance, general lack of energy, and pale or bluish tongue and gums due to a lack of oxygen. Precautions should be taken to avoid overheating, excessive excitement, and excessive exercise, which may cause increased panting. Excessive barking or panting may cause the throat to swell, which could result in a totally blocked airway. Most importantly, the owner should not let the dog get too hot, particularly in the summer months, and should not allow the dog to become overweight because obesity will exacerbate the respiratory difficulties. If severe, this disorder can result in death from such related causes as heatstroke.
Lung volumes and capacities
The respiratory capacity, or the amount of air that moves in and out of the lungs, depends on the strength of inspirations and expirations. During normal, quiet breathing, the volume of air moving in and out of the lungs is called the tidal volume (TV). Only about 70% of tidal volume reaches the lungs. The remaining portion of the air is found in the airways including the nose, pharynx, larynx, trachea, bronchi, bronchioles, and terminal bronchioles. These airways are collectively called the anatomical dead space.
The minute volume (MV) is the volume of air inhaled and exhaled each minute, and is calculated as

The respiration rate varies by species (Table 14.1). Because of the anatomical dead space, not all of the minute volume is available for gas exchange. The alveolar ventilation rate (AVR) is that portion of the tidal volume that actually reaches the site of gas exchange:

If an animal inhales more forcefully, it can increase the volume of air entering the lungs above normal tidal volume (Fig.
14.8). The additional inhaled air is called the inspiratory reserve volume. Similarly, an animal can force more air out of its lungs than occursTable 14.1. Tidal volume and respiration rate.1

Data from Swenson and Reece (1993).
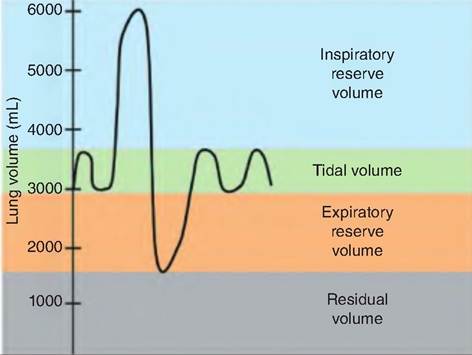
Fig. 14.8. Respiratory volumes and capacities. During quiet respiration, the volume of air inspired and expired is called the tidal volume. The additional air brought into the lungs during a forced inspiration is called the inspiratory reserve volume, and the additional air that can be expired during a forced expiration is called the expiratory reserve volume. The air remaining in the lungs after a forced expiration is called the residual volume.
Henry's law
Henry's law says that the quantity of a gas that will dissolve in a liquid is proportional to its partial pressure and its solubility coefficient. Therefore, gases will dissolve in body fluids more readily if they have a greater partial pressure and solubility coefficient. The solubility coefficient of CO2 is 24 times higher than that of O2. Therefore, CO2 dissolves in blood more readily than O2. In contrast, the solubility of nitrogen is very low, so even though atmospheric air has 79% N2, it has very little effect on body functions.
during quiet respiration. This additional volume exhaled is called the expiratory reserve volume. Following a forced expiration, the air remaining in the lungs is the residual volume.