Recognition of injury
Initiation of an inflammatory response requires that an inflammatory stimulus be recognized by the body. Endogenous proinflammatory molecules, including cytokines and danger-associated molecular patterns (DAMPs) that are released from dying cells, can stimulate inflammation.
Proinflammatory mediators are also derived from extracellular components such as the extracellular matrix and plasma. Exogenous stimuli, including infectious organisms, are commonly recognized by the body by pattern recognition receptors (PRRs) on tissue cells and macrophages, which recognize specific pathogen-associated molecular patterns (PAMPs), and by receptors that recognize the constant region (Fc) of antibodies bound to pathogens. Signaling through these cellular receptors leads to the release of mediators by cells present at the site of injury.Inflammatory mediators typically have more than one function and can have redundant functions. Mediators often synergize with one another and can have a cascade effect where the action of one mediator depends on previous actions of other mediators. Mediators may have autocrine, paracrine, and/or endocrine effects (Figure 2.1). Importantly, these effects are not antigen specific. Mediators generally exist in inactive forms in the plasma or in intracellular storage pools and are synthesized, released, or activated at the site of injury. They are responsible for hemodynamic and vascular permeability changes that occur during acute inflammation and attract inflammatory leukocytes to the site of injury.
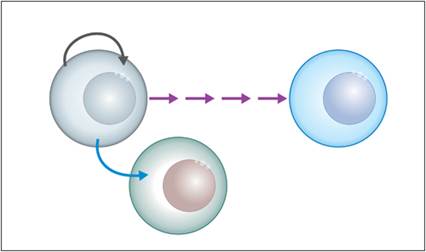
Figure 2.1 Autocrine, paracrine, and endocrine effects. Cell mediators with autocrine effects (gray arrow) signal changes in the same cell that the mediator was secreted from. Paracrine effects (blue arrow) signal nearby cells to alter their function.
Endocrine effects (purple arrows) are observed when cell mediators signal changes in distant cells after being secreted into the plasma or extracellular fluids.
Plasma-derived inflammatory mediators
Kinins
Kinins are potent, slow-acting vasodilators that increase capillary permeability. They mediate pain and produce sustained rubor, calor, and dolor associated with inflammation. They can stimulate the release of histamine and activate the eicosanoid cascade to form leukotrienes and prostaglandins. Kinins are comprised of short peptides derived from plasma protein precursors. Inactive precursor kininogens are broken down by active kallikreins into the shorter, active kinins (Figure 2.2). Bradykinin is the prototype short chain peptide.
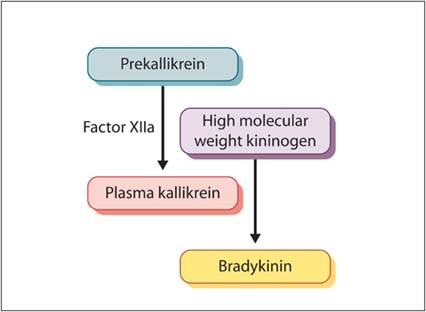
Figure 2.2 Kinins. Inactive precursor kininogens are cleaved to form active kinins, including bradykinin.
Components of the coagulation cascade, including activated Hageman factor (factor XII) and plasmin, can activate pre-kallikreins and initiate production of bradykinin (Del Rosso et al., 2008; Schmaier, 2008). Leukocytes also produce kinins that are similar to bradykinin. Additionally, there are tissue kallikreins, which are released when parenchymal cells are lysed, that bind high molecular weight kininogen and activate it to form bradykinin (Schulze-Topphoff et al., 2008). Kinins are rapidly inactivated by other enzymes in tissues and plasma, especially in the lung, to prevent excessive tissue damage.
Acute phase proteins
When acute injury has occurred in the body, the serum concentrations of acute phase proteins change by >25% during the first few days of an inflammatory response. There is an increase in the concentration of positive acute phase proteins and a decrease in negative acute phase proteins (Table 2.1). Most acute phase proteins are synthesized in the liver. Changes in acute phase protein concentrations reflect the presence and intensity of inflammation and are important diagnostic indicators of inflammation in some species (Figure 2.3).
The major responding acute phase protein differs slightly in different species (Eckersall & Bell, 2010).Table 2.1 Selected acute phase proteins (APPs) in the dog and cat
| Positive APPs | Negative APPs |
| al acid glycoprotein | Albumin |
| C-reactive protein* | Antithrombin |
| Complement factors | Transferrin |
| Haptoglobin | |
| Hepsidin | |
| Ferritin | |
| Fibrinogen | |
| Fibronectins | |
| Mannose-binding lectin | |
| Serum amyloid A*† | |
| * Major APPs in dogs. | |
| * Major APPs in dogs. | |
| † Major APPs in cats. | |
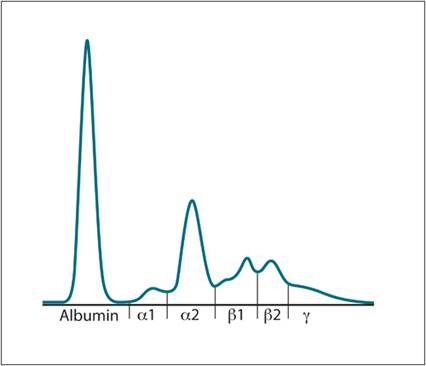
Figure 2.3 Serum protein electrophoresis tracing. An acute phase protein reaction is occurring with increases in alpha- and beta-globulins.